Etiologies and Predictors of ST-Segment Elevation Myocardial Infarction
7
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
수치
관련 문서
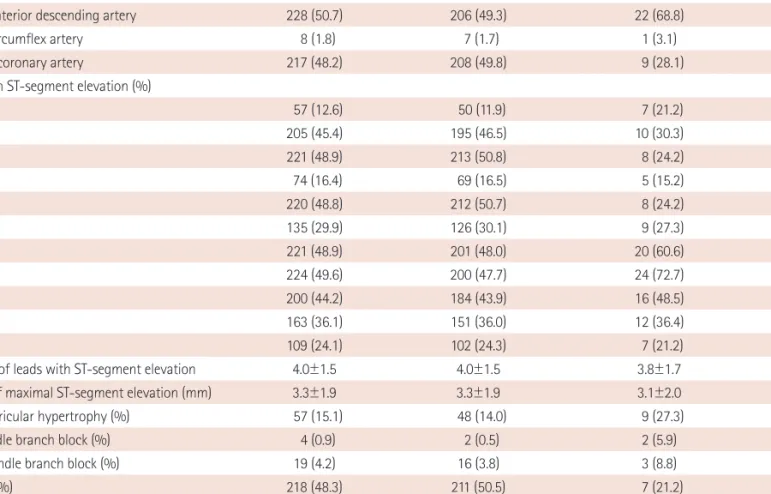
Results: On presenting ECG, 32.5% of patients had ST-segment depression, 24.2% of patients had T-wave inversion, 13.3% of patients had Q-wave, 6.7% of patients
Rapid reperfusion in ST-elevation myocardial infarction (STEMI) is the most critical factor in saving a patient's life. 1) Compared to the thrombolysis era when STEMI was only
A recent French study on the role of MVR in patients with STEMI presenting with cardiogenic shock and resuscitated cardiac arrest showed that MVR may improve 6-month survival
However, very little re- search has been conducted to clarify the impact of exercise training on clinical outcomes in patients with ST-elevation myocardial infarction
Background The aim of this study was to assess the impact of more aggressive pharmacological treatment on short-term clinical outcomes in patients with acute non
Clinical Benefit of Low Molecular Weight Heparin for ST-segment Elevation Myocardial Infarction Patients Undergoing Primary Percutaneous Coronary Intervention with
It is uncertain that atorvastatin pretreatment can reduce myocardial damage in patients undergoing primary percutaneous coronary intervention (PCI) for ST-segment elevation
The aim of this study is to investigate the clinical outcomes of the elderly patients with Non ST-segment elevation myocardial infarction (NSTEMI) undergoing coronary ar- tery
