INTRODUCTION
The lateral nasal wall is anatomically quite complex, so most cases of the congenital anomalies occur therein.
Its anatomical complexity predisposes subjects to inflam- matory disease. In normal subjects, the lateral nasal wall bears the ostia of the paranasal sinuses, and its mucosa lines the sinuses. This wall also bears the nasal turbinates, which are exquisite projecting scrolls of bone covered by the mucous membrane. The turbinate is important for 2 reasons: it is used as a surgical landmark during endo- scopic sinus surgery, and it plays an important role in the physiologic functions of the nose and its related paranasal sinuses. Hypogenesis or agenesis of the turbinate disrupts delicate processes of both turnover and drainage of mu- cosal secretions.1) 2) Bilateral middle and inferior turbinate agenesis is extreamly rare.
We report herein a case of bilateral inferior and middle tur- binate agenesis which was manifested as atrophic rhinitis.
CASE
A 27-year-old woman presented with nasal obstruction, crust formation, anosmia, and foul odors. Her symptoms
had begun 10 years earlier. She had no history of nasal surgery, cosmetic surgery, or trauma. Furthermore, she had no history of infectious diseases-including tubercu- losis and syphilis, granulomatous diseases, sarcoids and Wegener's disease, and radiation therapy.
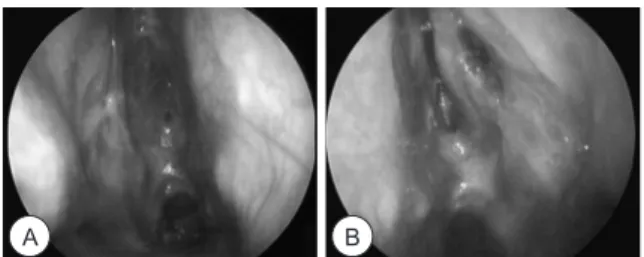
Endoscopic examination revealed severe atrophy of the nasal mucosa, crusts with foul odors, purulent discharge in both nasal cavities as well as the absence of both inferior and middle tubinates (Fig. 1). This finding was confirmed by computed tomography (CT). CT also revealed mucosal inflammation in the bilateral ethmoid sinuses, which were poorly developed, and the left maxillary sinus (Fig. 2).
J Rhinol 20(2), 2013
- 139 -
www.ksrhino.or.kr
Primary Atrophic Rhinitis with Bilateral Turbinates Agenesis
Chul Chang, MD and Won Kyoung Kong, MD
Department of Otorhinolaryngology – Head and Neck Surgery, CHA Bundang Medical Center, CHA University, Seongnam, Korea
ABSTRACT
In this paper, we report a case of bilateral inferior and middle turbinate agenesis, a rare anomaly. A 27-year-old woman presented with nasal obstruction, crust formation, anosmia, and foul odors. Anterior rhinoscopic examina- tion revealed the absence of the middle and inferior turbinates on both sides. The patient had no history of nasal or sinus surgery. She denied over having expelled anything of significance from her nasal cavity. She had no history of infectious disease-including tuberculosis and syphilis, granuolomatous diseases, sarcoids, Wegener's disease, and radiation therapy. There have been few reports on bilateral turbinate agenesis.
KEY WORDS : Agenesis·Turbinate·Rhinitis.
Address correspondence and reprint requests to Chul Chang, MD, De- partment of Otorhinolaryngology – Head and Neck Surgery, CHA Bun- dang Medical Center, CHA University, 351 Yatap-dong, Bundang-gu, Seongnam-si, Gyeonggi-do 463-712, Korea
Tel: +82-31-780-5340 · Fax: +82-31-780-5348 E-mail: [email protected]
Received for publication on May 14, 2013 Accepted for publicatoin on August 13, 2013
Fig. 1. Endoscopic view of both nasal cavity(A:Right, B:Left) with a 0-degree scope showing a purulent discharge, bloody crusts, and absence of tubinates.
A B
C D
140 / J Rhinol 20(2), 2013
The inflammation was not completely controlled by con- tinual medical therapy. The patient underwent endoscopic sinus surgery and thereafter irrigated the nasal cavity with a mixture of saline and olive oil,vitamin E solution for 1 month.
At the 3-month follow-up, the nasal cavity was clean and infection was resolved (Fig. 3).
Her medical history was obtained again, and she denied that she had any masses in her nose or had expelled any tissue from her nose. There is no specific finding in her dietary, hereditary, or hormonal condition associated with atrophic rhinitis.
DISCUSSION
In humans, 3 or 4 turbinates are located on either side of the nasal cavity. Most of the nasal cavities have 3 tur- binates: inferior, middle, and superior. A fourth turbinate can be located above the superior turbinate, which is called the supreme turbinate.1) 2) The embryological devel- opment of the lateral wall is a complex process. In the 9th to 10th weeks of fetal development, 5 ethmoturbinals, 1 maxilloturbinal, and 6 major furrows develop on the lateral nasal wall. The inferior turbinate develops from the maxilloturbinal. The agger nasi is the remnant of the ascending portion of the ethmoturbinal, and the uncinate process develops from the descending portion of the first ethmoturbinal. The middle turbinate develops from the second ethmoturbinal, and the superior turbinate devel- ops from the third ethmoturbinal. With further develop- ment, a second set of folds and grooves develops between
the middle and inferior turbinates. The first and second turbinals fuse to form the ethmoidal bulla.3) The inferior turbinate plays an important role in the physiology of the nasal cavity. The inferior portion of the nasal cavity makes up over 50% of nasal airflow. Total inferior turbinectomy can radically change the physiology of the nasal mucosa.
In particular, the procedure can lead to incomplete warm- ing of inspired air and inefficient mucociliary transport in the nose.2) These changes may result in a decrease in de- fense activity and lead to crusting and/or atrophic rhinitis.
Moreover, drainage of mucosal secretions of the paranasal sinuses can be disturbed, as in our patient. In addition to these physiologic functions, the middle and inferior tur- binates are often used as surgical landmarks during endo- scopic sinus surgery.4) 5)
Atrophic rhinitis, also known as ozena, is a chronic nasal disease characterized by progressive atrophy of the nasal mucosa and formation of dry crusts.6) Its causes still remain uknown. Culture results usually demonstrate Klebsiella ozaenae, Corynebacterium diphtheriae, or the Perez-Hofer bacillus.7) Atrophic rhinitis can be of the pri- mary (idiopathic) or secondary type. Secondary atrophic rhinitis is caused by overzealous intranasal surgeries, such as extensive submucosal septal resection and total inferior turbinectomy.8)
Other etiology are heredity factor, endocrine imbalance:
the disease tends to start at puberty and mostly involves females, racial factors: whites are more susceptible than natives of equatorial Africa, nutritional deficiency: vita- mins A or D, or iron, autoimmune disease: viral infection or some other unidentified insult may trigger antigenicity of the nasal mucosa.
One of the most widely used treatments is nasal irriga- tion. This can be used with curative intent or as mainte- nance therapy. Irrigations are used to prevent the forma- tion of the hallmark extensive crusting. To achieve this result, irrigations must often be done multiple times in a day. As a result, patient compliance is often difficult. The type of irrigation used varies by author, and numerous solutions have been suggested. No evidence of benefit of one solution over the other has been noted. Suggested for- mulas include normal saline, a sodium bicarbonate saline solution, or a mixture of sodium carbonate, sodium bibo- rate, and sodium chloride in plain water. The frequency of usage varies, but can be adjusted by the patient as needed to prevent crusting.
Other topical methods are used to prevent drying or increase hydration. These include the application of anti- evaporation compounds. Examples of these compounds noted in the literature include glycerine, mineral oil, or menthol mixed with paraffin. These are usually used as adjuncts, and may be applied following irrigation proce-
Fig. 2. Coronal OMU CT of Turbinates dysgenesis. Poorly devel- oped ethomoidal cells and absence of both turbinates.
Fig. 3. endoscopic examination demonstrates clear right(A) and left(B) nasal cavities one month postoperatively
A
A
B
B
Chang et al : Bilateral Turbinates Agenesis / 141 dures. Hydration therapies include the application of pilo-
carpine or atropine to the mucosa to stimulate the remain- ing mucous glands. Little information on the effectiveness of these therapies is available.
Systemic or oral therapies are often used in conjunc- tion with the topical treatments. The most common type of systemic therapy is antibiotics. Currently, oral antibiotic therapies involve either tetracycline or a floroquinolone.
Just as the “curative” irrigations, these are only given to resolve the purulent discharge and foul odor, and then are discontinued in favor of maintenance irrigation therapy.
Other therapies have been suggested based on individual responses. These include potassium iodide to increase na- sal secretions, vasodilators to increase blood flow to the atrophic mucosa, Corticosteroids have been proposed as an adjuvant by some, but others consider nasal steroids contraindicated in this condition. Vasoconstrictors for subjective nasal congestion are contraindicated due to the poor vascularization of the mucosa.
Atrophic rhinitis is an uncommon disorder in many parts of the world. This has led to controversies in regards to ev- ery portion of the disease, from etiology to management.
Current understanding suggests that this is a single con- dition which may arise either primarily from yet uncon- firmed factors, or results secondarily from insult to the na- sal cavities. The treatment of this condition often involves multiple treatment modalities; and can be local, systemic, or surgical. Since cases are rare, no formal recommenda- tions for treatment exist, and care must be tailored to the needs or desires of the patient. In cases of doubt, however, it is useful to remember the course of the disease process.
Atrophic rhinitis has been noted to resolve or lessen dra- matically, typically during the fifth decade of life. When considering the timing or consequence of therapies, this should always be tempered with the understanding that the patient is likely to undergo resolution or improvement with a tincture of time.
In our case, we believe that crusting and inflammatory
changes in both nasal cavities were due to the absence of turbinates. To the best of our knowledge, there have been only a few reports similar to ours. We presented a rare case of atrophic rhinitis patient with bilateral middle and inferior turbinate agenesis.
This case was presented at The 86th Annual congress of Korean Society of Otorhinolaryngology–Head and Neck Surgery April 28 2012
This case report has been approved by the Institutional Review Board of CHA Medical Center. Patient consent for publication has been obtained by the authors.
저자역할(Author Contributions)
장철, 공원경은 본 연구에서 모든 자료에 접근할 수 있으며, 자료의 완 전성과 자료 분석의 정확성에 책임을 지고 있습니다. 연구 기획 : 장 철, 공원경, 자료 해석 및 분석 : 장철, 공원경, 논문초안 : 장철, 공원 경, 논문수정 : 장철, 공원경, 연구 총괄 : 장 철
REFERENCES
1) WH. H. The nose and paranasal sinuses. In: WH. H, editor. Anat- omy for surgeons. 3rd ed., New York: Harper & Row; 1982. p.
233-7.
2) Hilberg O, Grymer LF, Pedersen OF, Elbrond O. Turbinate hyper- trophy. Evaluation of the nasal cavity by acoustic rhinometry. Arch Otolaryngol Head Neck Surg. 1990;1163:283-9.
3) Stammberger H. Functional Endoscopic Sinus Surgery: The Messerklinger Technique. Philadelphia: B.C. Decker,1991.p.49- 4) Arslan H, Aydinlioglu A, Bozkurt M, Egeli E. Anatomic variations 88.
of the paranasal sinuses: CT examination for endoscopic sinus sur- gery. Auris Nasus Larynx. 1999;261:39-48.
5) Rao VM, el-Noueam KI. Sinonasal imaging. Anatomy and pathol- ogy. Radiol Clin North Am. 1998;365:921-39, vi.
6) Zohar Y, Talmi YP, Strauss M, Finkelstein Y, Shvilli Y. Ozena re- visited. J Otolaryngol. 1990;195:345-9.
7) Shehata MA. Atrophic rhinitis. Am J Otolaryngol. 1996;172:81-6.
8) Shehata M, Dogheim Y. Surgical treatment of primary chronic atro- phic rhinitis (an evaluation of silastic implants). J Laryngol Otol.
1986;1007:803-7.