Received: February 8, 2017 Revised: May 25, 2017 Accepted: June 5, 2017.
Corresponding author: Dae-Hyun Kim
Department of Family Medicine, Keimyung University College of Medicine, 56 Dalseong-ro, Jung-gu, Daegu 41931, Korea Tel: +82-53-250-7548, Fax: +82-53-250-7071, E-mail: [email protected]
Copyright Ⓒ 2017 The Korean Academy of Clinical Geriatrics
This is an open access article distributed under the term s of the Creative Com m ons Attribution Non-Com m ercial License (http://creativecom m ons.org/ licenses/by-nc/4.0) which perm its unrestricted non-com m ercial use, distribution, and reproduction in any m edium , provided the original work is properly cited.
한국 노인에서 악력 저하와 관련된 요인
오병택, 황영시, 이준영, 박상균, 홍승완, 서영성, 김대현 계명대학교 의과대학 가정의학교실
Factors Related with Hand Grip Strength in Korean Elderly
Byung-Taek Oh, Young-Si Hwang, Jun-Young Lee, Sang-Kyun Park, Seung-Wan Hong, Young-Sung Suh, Dae-Hyun Kim
Department of Family Medicine, Keimyung University College of Medicine, Daegu, Korea
Background: Hand grip strength is important to identify old people with functional limitation. The objective of this study was to investigate the factors related with Reduction of Hand grip strength in Korean elderly.
Methods: Korean community-dwelling elderly (n=3,598, male/female 1,577/2,021) at the first wave (2006) of KLoSA (Korean Longitudinal Study on Aging) were used for analysis. Hand grip strength was assessed with Dynamometer for 2times each arm and we calculated hand grip index. Hand grip strength, Socioeconomic status, Health related status was assessed through personal interviews by a trained interviewer with Computer Assisted Personal Interviewing (CAPI).
Results: 1,684 subjects (46.8%) were classified as Low hand grip strength group (<26 kg for male, <18 kg for female).
Age, sex, MMSE score, education, employment, living with spouse, social activity, depression scale (Center for epidemio- logic studies depression scale, CESD-10), function (Activity of daily living, ADL), smoking, drinking, BMI (Body mass index), hypertension and diabetes was significantly related with low hand grip strength. Low hand grip strength ratio for age 70∼74 and ≥75 were 1.68 (1.40∼2.02) and 2.89 (2.39∼3.50) compare to younger age group, female was 2.04 (1.73∼2.40), cognitive impairment was 1.84 (1.57∼2.16), no exercise group was 1.34 (1.13∼1.58). Among health-related factors, alcohol consumption and diabetes were significantly higher in low grip strength group. Among physical/psychological factors, cognitive impairment (MMSE≤23), function (ADL), depression scale (CESD-10), obesity were significantly different after multivariates adjustment.
Conclusion: Age, sex, education, employment, alcohol consumption, diabetes, cognitive impairment, depression scale (CESD-10), function (ADL), exercise, obesity were significantly related with cognitive decline in Korean elderly.
Key Words: Frailty, Hand grip strength, Elderly
서 론
평균수명의 연장으로 인구 고령화가 빠른 속도로 진 행되고 있다. 평균 수명은 61.9세(1970년)에서 81.9세 (2013년)로 증가하고 65세 이상 노인인구의 비율은 2015 년 현재 13.1%에서 2020년에는 15.6%, 2060년에는 40%
대에 이를 것으로 추정된다.1) 이처럼 빠른 속도로 고령 화가 진행됨에 따라 건강 노화와 노쇠(frailty)에 대한 관 심이 증가하고 있다.
노쇠란 노화에 따라 장애와 사망의 위험이 높아지는 것을 의미하며, ‘고령기에 다양한 원인으로 여러 장기의 생리적 예비능이 줄어 들어, 스트레스를 견디는 힘이 떨 어지고, 장애, 질병, 입원, 사망과 같은 부정적 건강상태 가 생기기 쉬운 상태’로 정의한다. 노쇠는 기능적 감소, 삶의 질 저하의 실질적 시작점이며, 장애, 입원, 사망을 예견하는 주요 인자이므로 이를 조기 발견하고 중재하 여 고령자에서 장애, 사망이나 질병 발생을 예방할 수 있다.2)
노쇠의 평가요인으로 사용되는 악력(grip strength)은 일상생활의 다양한 영역에서의 활동과 관련된 근력과 손기능을 좌우하여 노인의 기능적 삶에 많은 영향을 주 며, 노년기 건강에 중요하다. 악력은 노인의 건강지표로 신체기능과 비례하며 사망률과도 관련이 있다.3,4)
악력 감소가 노인의 삶에 여러 가지 영향을 미치지만 우리나라에서 악력에 대한 연구는 부족한 실정이므로 노동부의 고령화 연구 패널조사(Korean Longitudinal Study on Aging, KLoSA)를 이용하여 65세 이상 노인에서 악력 감소와 연관된 요인에 대해서 파악하고자 한다.
대상 및 방법
1. 조사대상
본 연구는 악력 감소와 이와 관련된 요인들을 파악하 기 위해 노동부의 고령화연구 패널조사(Korean longitu- dinal study on aging, KLoSA)의 1차년도 조사연구자료를 분석하였다. KLoSA는 제주도를 제외한 우리나라에 거주 하는 45세 이상 중고령자 성인들을 대상으로 노인들의 사회적 관계, 건강, 경제상태를 조사한 자료로서 2006년 부터 자료수집을 시작하여 2년 간격으로 동일한 응답자 를 추적 조사하였다. KLoSA에 포함된 한국인들은 컴퓨 터를 이용한 대인 면접(computer assisted personal inter-
viewing, CAPI)을 통하여 인구사회학적, 사회경제적 요인 과 노쇠 연관 요인들 그리고 병력을 수집하였다. 노쇠 연관 요인들로는 일상생활활동(activity of daily living, ADL), 악력 지수, CESD-10 (center for epidemiologic stud- ies depression scale) 설문지에 의해 평가된 우울증이 포함 되었다. 병력으로는 고혈압, 당뇨병에 대해 수집하였다.
본 연구에서는 2006년 1차 조사에 참여한 10,254명 중, 대상자가 65세 미만이거나 악력 측정을 하지 않은 경우는 제외하였고 최종적으로 3,598명의 노인이 연구 분석에 참여하였다.
2. 악력의 평가
악력을 측정하기 위해 사용된 지표는 악력지수이다.
악력지수는 악력계(TANITA NO6103, Tokyo, Japan)를 사용하여 양손의 악력을 각각 2번씩 측정한 값들의 전체 평균값을 이용하였다. 손이 불편할 경우 반대쪽 손만 측 정한 값을 이용하였다.
악력의 저하는 아시아 근감소증 연구회(Asian Working Group of Sarcopenia) 기준에 따라 남성의 경우 악력 지수 26 kg, 여성의 경우 악력 지수 18 kg을 기준으로 하였다.5)
3. 인구사회학적 요인 평가
인구사회학적 요인에는 나이, 교육수준, 배우자와의 관계, 거주지역, 노동여부가 포함되었다. 나이는 65∼69 세, 70∼74세, 75세 이상의 세 그룹으로 구성하였다. 교 육수준은 초등학교 졸업 이하, 중학교 졸업 이하, 고등 학교 졸업 이상의 세 그룹으로 범주화 하였다. 배우자와 의 관계는 배우자와 같이 사는지 여부로 나누었다. 거주 지역 구분은 서울특별시 또는 광역시이면서 동부일 경 우 대도시, 도이면서 동부일 경우 중소도시, 그리고 읍 면부로 나누었다, 노동 여부는 현재 고용 되어 근로하는 지를 확인하였다.
4. 생활건강 요인 평가
생활건강 요인에는 흡연과 음주, 고혈압과 당뇨병 유 병여부가 포함되었다.
흡연은 현재 담배를 피우고 있으면 현재 흡연자로, 과 거 5갑 이상 담배를 피운 적이 있으면 과거흡연자로, 5 갑 이상 담배를 피운 적이 없으면 비흡연자로 구분하여 현재 흡연자를 한 그룹으로 과거 흡연자와 비흡연자를 다른 그룹으로 구성하였다.
음주는 요즘에도 술을 마시는 경우 현재 음주자로, 요 즘은 술을 끊은 경우 과거 음주자로, 원래 술을 잘 마시 지 못하거나 마신 적 없는 경우 비음주자로 구분하여 현 재 음주자를 한 그룹으로 과거 음주자와 비음주자를 다 른 그룹으로 구성하였다.
5. 신체정신 요인 평가
신체정신 요인에는 인지능력과 우울증 여부, 일상생 활 수행 능력, 평소 운동 여부와 비만 여부 등이 포함되 었다.
인지 능력은 한국판 간이 정신상태 검사(Korean ver- sion of the mini-mental state examination-Korea, MMSE-K) 를 이용하여 지남력, 기억력 등을 측정하는 30개 문항의 점수를 총합하여 지수화 하였다. 이러한 인지기능점수가 23점 이하일 경우 인지기능 저하 그룹으로 인지기능점 수가 24점 이상일 경우 인지기능 정상 그룹으로 나누었 다.6)
우울증 여부는 Radloff가 개발한 Center for Epidemiologic Studies-Depressed Mood Scale (CESD-10)척도를 사용하였 다. CESD-10은 지난 일주일간 본인의 느낌과 행동에 대 한 10가지 문항의 질문에 대해 4점 리커트형 척도로 조 사한다. 각 설문 문항에서 있다/없다에 각각 ‘1점’과 ‘0 점’을 부여한 후 모두 더한 값이 4점 이상이면 우울증이 있다고 분류하였다.7) 일상생활 수행 능력(activities of dai- ly living, ADL)은 Kim 등8)에 의해 개발된 한국어판 바텔 일상활동지표(Barthel ADL index)를 이용하여 측정하였 다. 한국어판 바텔 일상활동지표는 옷 갈아입기, 세수/양 치/머리감기, 목욕/샤워하기, 식사하기, 방 밖으로 나가 기, 화장실 이용하기와 대소변 조절하기를 수행하는데 있어 다른 사람의 도움이 필요한지 여부에 따라 측정하 였다. 일상 생활을 하는데 있어 부분적인 도움을 필요로 하거나 전적으로 도움이 필요할 경우 ‘1’, 도움을 필요로 하지 않으면 ‘0’으로 하였다. 본 연구에서는 기본적인 일 상 생활 수행 능력 항목을 모두 합하여 ADL 지수화 점수 가 1 이상일 경우 의존적인 것으로 분류하였다. 평소 운 동을 1주일에 1회 이상 했을 경우 ‘예’, 그렇지 않을 경우
‘아니오’로 구성하였다. 과체중 여부는 체질량지수(Body mass index)에 따라 23을 초과 할 경우 과체중군으로 분류 하고 23 이하일 경우 비과체중군으로 분류하였다.
6. 통계 분석
본 연구의 통계 분석은 SPSS (Version 21.0; SPSS inc., Chicago, IL)를 이용하였다.
먼저 연구대상자의 일반적 특성을 분석하기 위하여 기술통계를 이용하였는데, 이 중 연속적인 변수들은 독 립표본 t-검정, 명목변수들은 카이제곱검정을 실시하였 다. 대상자들을 악력 정상인군과 악력 저하군으로 나누 어 연령(year, continuous), 성별, 결혼 여부, 인지기능 (MMSE-K score, continuous), 우울증 여부(yes or no), 학력 (<Elementary, Middle, ≥High), 고용 상태(yes or no), 거 주지(Metropolitan, City, Urban), 배우자와 함께 사는지 여 부(yes or no), 사회 활동정도(≤6/year, 1∼2/month, ≥ 1/week), 음주(Current or Past/None), 흡연(Current or Past/None), 운동(≥1/week or no), BMI (continuous), 고혈 압(yes or no), 당뇨(yes or no)에서의 차이를 비교하기 위 해 독립표본 t-검정을 시행하였다.
악력 저하군에 미치는 여러 요인을 분석하기 위해서 악력 저하군과 악력정상군에서 인구 사회학적 요인, 생 활 건강 요인, 신체 정신 요인을 다중회귀분석방법을 이 용하여 교차비(Odds ratio)를 분석하였다(Model 1=raw, Model 2=adjusted by age, sex, exercise, obesity, Model 3=adjusted by age, sex, exercise, obesity, employment, Cognitive impairment, ADL, CESD-10). 모든 분석에서 유 의수준은 P<0.05로 양측성 검정을 하였다.
결 과
1. 연구 대상자의 일반적 특성
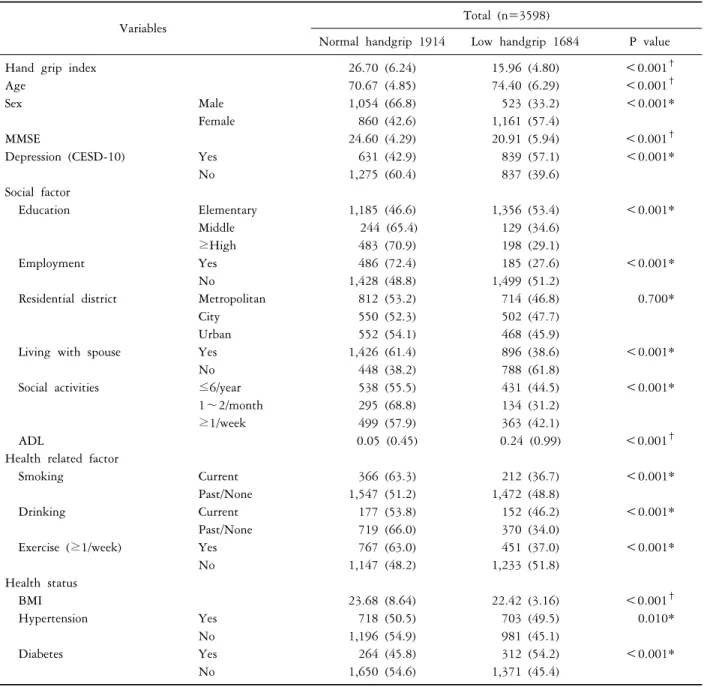
총 3,598명의 대상자가 최종 연구에 포함되었고 그 중 1,914명의 악력이 정상으로 분류되었고, 1,684명의 악력 은 정상보다 낮다고 분류되었다.
악력 저하군의 평균 나이는 74.4세였고 그 중 남성이 523명(33.2%), 여성이 1,161명(57.4%)이었고 악력 정상군 은 평균 나이가 70.67세, 남성은 1,054명(66.8%), 여성은 860명(42.6%)으로 악력 저하군이 유의하게 연령이 높고 여성의 비율이 높았다. 악력 저하군은 그렇지 않은 군에 비해 운동을 1주일에 1회 이상하는 사람(451명 vs 767명, P<0.001)이 적고, 비만도(22.42 vs 23.68, P<0.001)가 더 낮았다. 악력 저하군은 MMSE score가 더 낮았으며 (20.91 vs 24.60, P<0.001), 우울증이 더 많이(839명 vs 631명, P<0.001) 있었다. 악력 저하군은 악력 정상군보
Table 1. General characteristics of Normal handgrip strength and Low handgrip strength group
Variables Total (n=3598)
Normal handgrip 1914 Low handgrip 1684 P value
Hand grip index 26.70 (6.24) 15.96 (4.80) <0.001
†Age 70.67 (4.85) 74.40 (6.29) <0.001
†Sex Male 1,054 (66.8) 523 (33.2) <0.001*
Female 860 (42.6) 1,161 (57.4)
MMSE 24.60 (4.29) 20.91 (5.94) <0.001
†Depression (CESD-10) Yes 631 (42.9) 839 (57.1) <0.001*
No 1,275 (60.4) 837 (39.6)
Social factor
Education Elementary 1,185 (46.6) 1,356 (53.4) <0.001*
Middle 244 (65.4) 129 (34.6)
≥High 483 (70.9) 198 (29.1)
Employment Yes 486 (72.4) 185 (27.6) <0.001*
No 1,428 (48.8) 1,499 (51.2)
Residential district Metropolitan 812 (53.2) 714 (46.8) 0.700*
City 550 (52.3) 502 (47.7)
Urban 552 (54.1) 468 (45.9)
Living with spouse Yes 1,426 (61.4) 896 (38.6) <0.001*
No 448 (38.2) 788 (61.8)
Social activities ≤6/year 538 (55.5) 431 (44.5) <0.001*
1∼2/month 295 (68.8) 134 (31.2)
≥1/week 499 (57.9) 363 (42.1)
ADL 0.05 (0.45) 0.24 (0.99) <0.001
†Health related factor
Smoking Current 366 (63.3) 212 (36.7) <0.001*
Past/None 1,547 (51.2) 1,472 (48.8)
Drinking Current 177 (53.8) 152 (46.2) <0.001*
Past/None 719 (66.0) 370 (34.0)
Exercise (≥1/week) Yes 767 (63.0) 451 (37.0) <0.001*
No 1,147 (48.2) 1,233 (51.8)
Health status
BMI 23.68 (8.64) 22.42 (3.16) <0.001
†Hypertension Yes 718 (50.5) 703 (49.5) 0.010*
No 1,196 (54.9) 981 (45.1)
Diabetes Yes 264 (45.8) 312 (54.2) <0.001*
No 1,650 (54.6) 1,371 (45.4)
Values were presented as mean (SD) or n (%), *analyzed by Chi-square test
†analyzed by t-test.
MMSE: mini-mental status examination, ADL: activities of daily living, CESD: center for epidemiologic studies short depression scale.
다 고용되어 있는 사람(185명 vs 486명, P<0.001)이 적 었으며, ADL 점수(0.24 vs 0.05, P<0.001)는 더 높았다.
이 외에 두 군은 교육 수준, 음주 여부, BMI, 고혈압 유 병 여부에서 유의한 차이를 보였으나 거주지에 대해서 는 비 독립적인 것으로 나타났다(Table 1).
2. 여러 요인에 따른 악력 저하
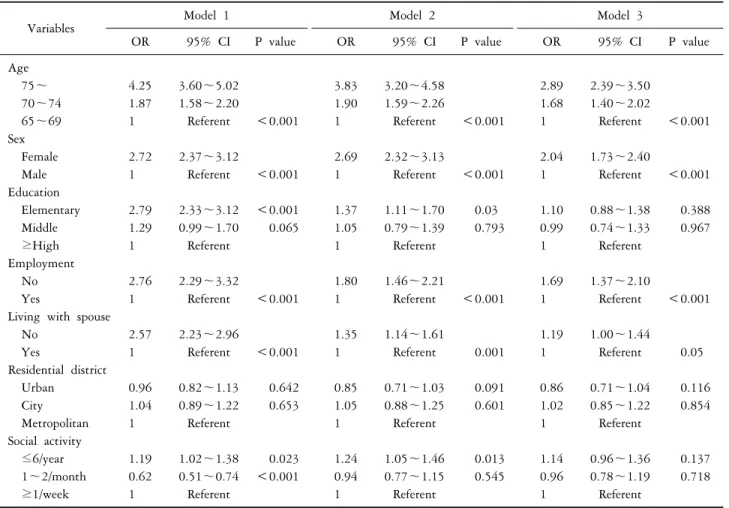
인구사회학적요인에 따른 악력 저하군에 속할 위험도 를 나이, 성별, 운동 여부, 비만 여부(overweight or Non-
overweight), 노동 여부, 인지 기능 저하(yes or no), 일상 생활 활동(independent or dependent)), CESD-10에 따른 우울증 여부(yes or no)로 다변량 보정하였다(Table 2).
대상자의 연령에 따른 악력 저하군에 속할 우도비 (95% 신뢰구간)는 65∼69세 그룹에 비해서 70∼74세 그 룹, 75세 이상 그룹일 때 각각 1.68 (1.40∼2.02), 2.89 (2.39∼3.50)였다. 노동을 하지 않는 그룹은 악력 저하군 에 속할 우도비가 1.69 (1.37∼2.10)로 노동을 하고 있는 그룹에 비해서 높았다. 성별 간 비교 하였을 경우 여성
Table 2. Hand grip strength ratio according to Social factors
Variables Model 1 Model 2 Model 3
OR 95% CI P value OR 95% CI P value OR 95% CI P value
Age
75∼ 4.25 3.60∼5.02 3.83 3.20∼4.58 2.89 2.39∼3.50
70∼74 1.87 1.58∼2.20 1.90 1.59∼2.26 1.68 1.40∼2.02
65∼69 1 Referent <0.001 1 Referent <0.001 1 Referent <0.001
Sex
Female 2.72 2.37∼3.12 2.69 2.32∼3.13 2.04 1.73∼2.40
Male 1 Referent <0.001 1 Referent <0.001 1 Referent <0.001
Education
Elementary 2.79 2.33∼3.12 <0.001 1.37 1.11∼1.70 0.03 1.10 0.88∼1.38 0.388
Middle 1.29 0.99∼1.70 0.065 1.05 0.79∼1.39 0.793 0.99 0.74∼1.33 0.967
≥High 1 Referent 1 Referent 1 Referent
Employment
No 2.76 2.29∼3.32 1.80 1.46∼2.21 1.69 1.37∼2.10
Yes 1 Referent <0.001 1 Referent <0.001 1 Referent <0.001
Living with spouse
No 2.57 2.23∼2.96 1.35 1.14∼1.61 1.19 1.00∼1.44
Yes 1 Referent <0.001 1 Referent 0.001 1 Referent 0.05
Residential district
Urban 0.96 0.82∼1.13 0.642 0.85 0.71∼1.03 0.091 0.86 0.71∼1.04 0.116
City 1.04 0.89∼1.22 0.653 1.05 0.88∼1.25 0.601 1.02 0.85∼1.22 0.854
Metropolitan 1 Referent 1 Referent 1 Referent
Social activity
≤6/year 1.19 1.02∼1.38 0.023 1.24 1.05∼1.46 0.013 1.14 0.96∼1.36 0.137
1∼2/month 0.62 0.51∼0.74 <0.001 0.94 0.77∼1.15 0.545 0.96 0.78∼1.19 0.718
≥1/week 1 Referent 1 Referent 1 Referent
Model 1: raw, Model 2: adjusted by age, sex, exercise, obesity, Model 3: adjusted by age, sex, exercise, obesity, employment, Cognitive impairment, ADL, Depression (CESD-10).
의 우도비가 2.04 (1.73∼2.40)로 나타났다.
생활 건강 요인에 따라 다변량 보정을 하였을 경우 음주에 따른 악력 저하군에 속할 우도비는 1.61 (1.21∼
2.15)로 나타났고, 당뇨병이 있을 경우 악력 저하군에 속 할 우도비가 1.54 (1.26∼1.89)로 유의하게 나타났다 (Model 3=adjusted by age, sex, exercise, obesity, employ- ment, Cognitive impairment, ADL, CESD-10) (Table 3).
신체 건강 요인에 따라 다변량 보정을 하였을 경우 대상자가 일주일에 1회 이상 운동을 하지 않았을 경우 악력 저하군에 속할 우도비는 1.34 (1.13∼1.58)로 높게 나타났다. 대상자가 BMI상 과체중일 경우 BMI가 정상 혹은 낮을 경우보다 악력 저하군에 속할 우도비가 0.67 (0.57∼0.78)로 낮게 나타났다. 인지 능력이 정상인 군에 비해 인지 능력 저하가 있는 군의 우도비는 1.84 (1.57∼
2.16)로 더 높았다. ADL 지수에서 생활이 독립적인 군에 비해 생활이 의존적인 군의 우도비는 2.02 (1.36∼2.99)
로 높았다. 또한 CESD-10에 의한 우울증이 없는 군보다 우울증이 있는 군의 우도비는 1.53 (1.31∼1.79)으로 높게 나타났다(Model 3=adjusted by age, sex, exercise, obesity, em- ployment, Cognitive impairment, ADL, CESD-10) (Table 4).
고 찰
본 연구를 통하여 65세 이상 노인에서 악력의 저하에 영향을 미치는 요인은 노화, 현재 노동 여부, 성별, 음주 여부, 당뇨병, 인지 기능 저하, ADL 지수, 우울증 여부, 운동 여부, 과체중 여부 등이 있음을 밝혀냈다. 그 동안 노쇠와 연관되는 여러가지 연구가 진행되고 있으나 악 력에 관한 연구는 아직 미흡하다.
악력의 근력 평가는 간단하면서도 비침습적인 지표로 이용될 수 있고,9) 정형화된 도구로 평가자가 다르거나 악력 측정기의 종류가 다르더라도 신뢰성 있게 측정 가
Table 3. Hand grip strength ratio according to Health status factors
Variables Model1 Model2 Model3
OR 95% CI P value OR 95% CI P value OR 95% CI P value
Alcohol
Yes 1.67 1.30∼2.14 1.70 1.29∼2.24 1.61 1.21∼2.15
No 1 Referent <0.001 1 Referent <0.001 1 Referent <0.001
Smoking
Yes 0.61 0.51∼0.73 0.96 0.77∼1.19 0.92 0.73∼1.16
No 1 Referent <0.001 1 Referent 0.691 1 Referent 0.472
HTN
Yes 1.19 1.04∼1.37 1.14 0.98∼1.33 1.10 0.94∼1.29
No 1 Referent 0.010 1 Referent 0.088 1 Referent 0.244
DM
Yes 1.42 1.19∼1.70 1.67 1.37∼2.04 1.54 1.26∼1.89
No 1 Referent <0.001 1 Referent <0.001 1 Referent <0.001
Model 1: raw, Model 2: adjusted by age, sex, exercise, obesity, Model 3: adjusted by age, sex, exercise, obesity, employment, Cognitive impairment, ADL, Depression (CESD-10).
HTN: Hypertension, DM: Diabetes mellitus.
Table 4. Hand grip strength ratio according to Physical/Psychological factors
Variables Model 1 Model 2 Model 3
OR 95% CI P value OR 95% CI P value OR 95% CI P value
Cognitive impairment
Yes (≤23) 3.34 2.91∼3.83 2.01 1.72∼2.36 1.84 1.57∼2.16
No (≥24) 1 Referent <0.001 1 Referent <0.001 1 Referent <0.001
ADL
Dependent 3.97 2.83∼5.59 2.86 1.95∼4.19 2.02 1.36∼2.99
Independent 1 Referent <0.001 1 Referent <0.001 1 Referent <0.001
Depression (CESD-10)
Yes 2.03 1.77∼2.32 1.70 1.46∼1.98 1.53 1.31∼1.79
No 1 Referent <0.001 1 Referent <0.001 1 Referent <0.001
Exercise (≥1/week)
No 1.83 1.59∼2.11 1.46 1.25∼1.71 1.34 1.13∼1.58
Yes 1 Referent <0.001 1 Referent <0.001 1 Referent <0.001
Obesity
Overweight 0.59 0.51∼0.68 0.66 0.57∼0.76 0.67 0.57∼0.78
Non-overweight 1 Referent <0.001 1 Referent <0.001 1 Referent <0.001
Model 1: raw, Model 2: adjusted by age, sex, exercise, obesity, Model 3: adjusted by age, sex, exercise, obesity, employment, Cognitive impairment, ADL, Depression (CESD-10).
ADL: Activity of daily living, CESD: center for epidemiologic studies short depression scale, Overweight: BMI>23, Non-overweight:
BMI≤23
능한 장점을 가지고 있다.10,11) 또한, Pahor 등12)과 Cesari 등13)에 따르면 신체 한 부위의 근력이 다른 부위의 근력 과 밀접한 연관이 있어 악력기로 측정된 악력이 하지 근 력의 측정을 대용할 수 있으므로, 노쇠에 따른 체력의 변화를 평가하기에 매우 유용한 지표로 볼 수 있다.14) 그리고 55세 이상 남녀를 대상으로 악력과 DXA 및
Bioelectrical impedance analysis (BIA)로 측정한 근육량의 상관성을 분석한 연구에서 남녀 모두 악력과 근육량에 유의한 상관관계를 보였다.15)
본 연구에서는 악력과 인지기능 장애, 일상생활 능력 에서도 상관관계가 있음을 확인하였고 이는 다른 연구 들에서도 유사한 결과를 보였다. 1991년부터 1995년까
지 71∼91세 노인을 대상으로 한 Giampaolin 등16)의 연 구에서는 악력이 남성 노인에 있어 일상 생활 능력의 제 한성을 예측할 수 있었으며, Alfaro-Acha 등17)은 7년간의 전향적 연구를 통해 65세 이상 노인에 있어서 기초 측정 악력이 낮을수록 인지 기능이 낮아짐을 보고하였다. 또 한, Rantanen 등18)은 1999년 25년간의 전향적 코호트 연 구를 통해 45∼68세의 중년 남성에게서 악력이 25년 후 삶의 기능적 부분의 예측 인자가 될 수 있음을 조사하였 다. 최근에는 우리 나라에서도 악력이 노인의 주관적 건 강을 예측하는 주요 변수가 될 수 있음을 Hong 등19)이 보고하였고, Yong20)은 정상 노인과 치매 노인의 손기능 과 인지 기능의 상관 관계에서 치매 노인의 손 장악력이 높을수록 인지 기능이 높은 상관 관계가 있음을 보고하 고 있다.
우리 연구의 강점은 악력 저하가 기존 연구와 마찬가 지로 인지 기능 장애나 ADL 의존 여부 등이 악력 저하 와 유의한 상관관계를 보이지만, 인지기능이나 일상 생 활 능력과의 연관성 외에도 당뇨병, 우울증 같은 질환과 도 연관이 있음을 보여 평상 시 신체 정신적 건강 상태 및 운동이나 노동 여부, 음주 여부와 같은 개인 생활적 요인에 대한 구체적인 연구가 필요함을 보여주고 있다.
그러나 본 연구에는 몇 가지 제한점이 있다. 첫째, 본 연구는 노동부의 고령화연구패널조사를 바탕으로 한 단 면조사로 악력의 감소와 노화, 인지 능력 등의 요인과 인과적 관계를 규명하긴 어렵다. 따라서 이에 대해 추적 연구가 필요한 실정이다. 두 번째, 악력의 감소 기준은 아직까지 논란이 있는 상태로 본 연구에서는 양측 악력 을 두 번 측정하여 평균을 낸 악력 지수를 이용하여 남 자 악력 지수 26 kg, 여자 악력 지수 18 kg의 아시아 근 감소증을 기준으로 정의하였다. 하지만 European working group on sarcopenia in older people에서는 남자 악력 지수 30 kg, 여자 악력 지수 20 kg인 것처럼21) 여러가지 기준 이 존재하므로 이에 대해 연구가 추가적으로 필요하다.
결론적으로 본 연구에서는 대규모 표본을 이용하여 65세 이상 남녀 노인에게서 악력 저하에 미치는 여러 가 지 요인들을 확인하였다. 이미 알려진 인지기능이나 일 상 생활 능력 외에도 당뇨병, 우울증, 운동 여부나 노동, 운동 여부에 대해서도 연관이 있었다. 그러므로 노인의 기능적인 삶에 많은 영향을 주고 노쇠를 조기 발견하여 장애나 질병 발생을 예방할 수 있는 악력에 대한 다각도 적이며 전향적인 연구가 필요할 것이다.
REFERENCES