접수일: 2017년 12월 11일, 게재승인일: 2017년 12월 15일 책임저자: 양은주, 경기도 성남시 분당구 구미로 173번길 82
13620, 분당서울대학교병원 재활의학과
Tel: 031-787-7734, Fax: 031-787-4056 E-mail: [email protected]
유방암에서의 어깨재활
분당서울대학교병원 재활의학과
양은주ㆍ임재영
Upper Limb Dysfunction and Rehabilitation for Breast Cancer Patients
Eun Joo Yang, M.D., Ph.D. and Jae-Young Lim, M.D., Ph.D.
Department of Rehabilitation Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
Cancer rehabilitation is a complex discipline that involves the interaction of diverse health care providers. Optimum health care management requires a multi-discipline approach.
This study describes our care system for providing compre- hensive management of upper limb dysfunction (ULD) for breast cancer survivors. Cancer treatment continuous, com- prehensive care includes physical rehabilitation and ex- ercise that integrated with disease treatment. After referral to the department of rehabilitation, the type of ULD is diag- nosed and categorized based on symptoms and physical examination. Specific rehabilitation programs are recom- mended according to the specific diagnosis. We developed a surveillance rehabilitation system for early detection and proper diagnosis of ULD after breast cancer treatment, and a continuous management system including a prevention, diagnosis and rehabilitation program. A surveillance pro- gram would allow healthcare providers to detect ULD early, affording better opportunities to prevent progression to the subclinical stage and to institute continuous care plans from the inpatient to the outpatient settings. (Clinical Pain 2017;16:69-76)
Key Words: Breast cancer, Upper limb dysfunction, Surveil- lance, Rehabilitation
INTRODUCTION
Upper limb dysfunction (ULD) has been reported as the most common problem after breast cancer, and it appears
to occur more frequently in persons with breast cancer than in the nondisabled population.1,2 Recently, in many studies, upper limb problems have been highlighted as one of treat- ment-related upper limb morbidities after surgery or radiation.3 ULD is a barrier to the successful restoration of function.4 In fact, upper limb problems developed after breast cancer treatment has been confined to lymphedema previously.5,6 However, various types of ULD such as per- sistent pain on shoulder or arm, limited range of motions (ROMs) and muscle atrophy have been developed over the long term, and also the high prevalence of ULD has been reported.7 Optimal upper body function is essential for maintaining independent living, performing tasks requiring physical strength, and general quality of life (QoL).8 Therefore, the ULD as a factor lowering patients’ QoL needs to be identified along with the fundamental treatment of breast cancer patients. Functional approach and the inter- disciplinary exchange of their opinion and interdisciplinary treatment system are required based on the change of rec- ognition related to QoL.9
A prospective surveillance model may be useful to de- tect breast cancer related lymphedema (BCRL) at an early stage, when the opportunities to reduce risk or slow pro- gression are optimal. A surveillance program would allow healthcare providers to detect BCRL symptoms early, af- fording better opportunities to prevent progression to the subclinical stage and to institute continuous care plans from the inpatient to the outpatient settings.10 Well-designed clinical pathway in conjunction with surgery and adjuvant therapies would be effective to manage the ULD related to breast cancer properly.11 It includes diverse treatments and care programs including treatment protocol, education ma- terials, exercise program, multimedia materials, etc. To de- veloping the care system for early detection and proper re- habilitative management of ULD, diagnostic criteria and categorization should be defined and specific management principles for each dysfunction should be organized. We have established the hospital cohort of breast cancer pa-
tients focused on treatment-related dysfunctions from 2006 in which over 600 participants registered. Based on the da- ta from the cohort, we were able to define and categorize each dysfunction and to suggest a model for multisectoral consulting system about ULD during and after breast can- cer treatment.
The prospective surveillance program was implemented in May 2011 to identify high-risk lymphedema patients who would benefit from comprehensive surveillance by a transdisciplinary team, with an emphasis on early detection and prevention of lymphedema. A care plan was initiated immediately after surgery for all patients who underwent axillary lymph node dissection (ALND) to identify patients at high risk of lymphedema.
This review will describe our multidisciplinary care sys- tem for providing comprehensive management of ULD for breast cancer survivors.
ASSESSMENT OF ULD
In physical examinations for upper limb function, an ROM, an upper extremity circumference and a shoulder strength were measured. Local tenderness on muscles and the sign of impingement syndrome also were included to evaluate the dysfunctions. Considering those findings from physical examinations, we categorized the ULDs into four major disease entities; impingement syndrome, adhesive capsulitis, lymphedema and myofascial pain syndrome (MPS).7 The pain intensity of patients was assessed by us- ing the pain score at rest and during activity by visual ana- logue scale (VAS) and brief pain inventory (BPI). BPI is an instrument for evaluating pain that measures both the intensity of pain and the degree to which pain interferes with a patient’s life.12 BPI uses an 11-point numeric rating scale (0 = ‘no pain’ and 10 = ‘pain as bad as you can imag- ine’) to evaluate the intensity of pain. The BPI includes a seven item pain interference scale that consists of the same 0∼10 response scale to the question: “describe how, dur- ing the last twenty four hours, pain has interfered with your: 1) general activity, 2) mood, 3) walking ability, 4) normal work (includes both work outside the home and housework), 5) relations with other people, 6) sleep, and 7) enjoyment of life.” The Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire was used to measure the functional status and symptoms associated
with different degrees and levels of ULD.13 The DASH questionnaire consists of 30 items, each of which has five possible responses. Twenty-one items ask about the degree of difficulty involved in performing different physical ac- tivities, six ask about symptoms, and the remaining three ask about psychosocial effects of spine problems.14 On physical examination, active shoulder ROM of affected and unaffected upper limb was measured with a goniometer ac- cording to a standardized protocol in forward flexion, ab- duction, and external rotation. The upper limb circum- ference of affected limb was measured with a measuring tape. The circumferences of axilla, above elbow, elbow, be- low elbow, wrist and metacarpophalangeal joint were taken at axilla, 10 cm proximal to the lateral epicondyle, at epi- condyle, 10 cm distal from the lateral epicondyle, at wrist and at metacarpophalangeal joint, respectively.15
LYMPHEDEMA
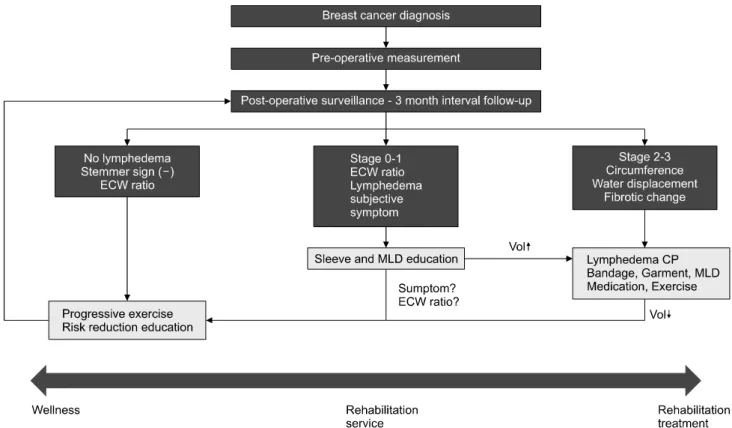
Lymphedema stage was determined by assessing reduc- tion of swelling with elevation, pitting with pressure, and the presence of fibrotic changes, by using the International Society of Lymphedema classification.16 In our institute, the prospective surveillance model was implemented in May 2011 to identify high-risk lymphedema patients who would benefit from comprehensive surveillance by a trans- disciplinary team, with an emphasis on early detection and prevention of lymphedema (Fig. 1). A care plan was ini- tiated immediately after surgery for all patients who under- went ALND to identify patients at high risk of lymphedema.
To detect subclinical lymphedema, we used a multi-fre- quency bioelectrical impedance analyzer (BIA) according to the manufacturer’s instructions. If the clinical lymphede- ma stage is greater than two, complex decongestive therapy (CDT) performed by specially trained lymphedema thera- pists, is considered to be the international standard of care.
Such therapy seeks to move lymphatic fluid to an area from which it may drain, thus reducing swelling. The therapy features manual lymph drainage (MLD), progressive active and action-assisted exercises, and compression therapy.
Patients with stage 0 or 1 subclinical lymphedema com- menced progressive strengthening exercises; they were in- structed in modified progressive weight-lifting exercises.
Patients participated in a supervised program run in the hospital and continued the program at home. Strengthening
Fig. 1. Clinical pathway for the prospective rehabilitation model of care.
exercises commenced with the aid of a thera-band. After checking shoulder strength using a manual muscle strength test, an appropriate thera-band was prescribed, as was the number of exercise repetitions. This number was pro- gressively increased if no symptoms were evident after three sessions. If the fluid volume decreased after intensive treatment, the patients returned to 3-month surveillance un- til 1 year after surgery, and were then screened at 6-month intervals.17
ASSESSMENT OF QoL
QoL was assessed using two validated questionnaires that were developed by the European Organization for Research & Treatment of Cancer Quality of Life Question- naire (EORTC).18-20 One questionnaire assesses cancer-spe- cific QoL (EORTC QLQ-C30) and the other evaluates site-specific (breast cancer) QoL (EORTC QLQ-BR23).18,21 The EORTC QLQ-C30 is a patient self-rating questionnaire that is composed of five (multi-item) function scales, which assess physical, role, social, emotional and cognitive func- tions, and three multi-item symptom scales, five sin-
gle-items that assess symptoms such as dyspnea, insomnia, appetite loss, constipation, diarrhea. A final item evaluates the perceived economic consequences of the disease.
Furthermore, a global health status/QoL-score can be computed. It consists of two items that assess the global health status and the global QoL. The breast cancer module QLQ-BR23 compromises 23 items. Systemic therapy side effects, arm symptoms, breast symptoms, body image and sexual functioning are evaluated by means of five mul- ti-item scales, in addition, three single items assess sexual enjoyment, hair loss and future perspective. According to the guidelines provided by the EORTC, all scores of the QLQ-C30 and -BR23 were transformed linearly so that all scales ranged from 0 to 100.22 In the function scales higher scores represents a better level of functioning. While in the symptom scales/items a higher score marks a higher level of symptomatology or problems. The contents of education after surgery include Shoulder ROM exercise education to prevent joint adhesion, pectoralis mobilization and stretch- ing to prevent pectoralis tightness or shortening, deconges- tive exercises to prevent lymphedema by enhancing the lymphatic passage, and core exercise for breast re-
construction by transverse rectus abdominis muscle (TRAM) flap surgery. Skin care, infection or trauma prevention, cau- tions of arm use to prevent lymphedema and diet recom- mendations were included.
THE CRITERIA FOR ULD AND THE PRINCIPLE OF TREATMENT 1. Lymphedema
The measurement of arm circumference at pre-defined positions relative to the olecranon is the traditional method used to diagnose secondary lymphedema. To increase the sensitivity of diagnosis, we considered that lymphedema was present when the difference in circumference at a single point of measurement was greater than 1 cm. Lymphostasis was defined as a difference of less than 1 cm in circum- ference, or a difference in circumference confined to the axillary area in an early period after surgery. CDT repre- sents the current international standard of care for lymphe- dema management. CDT is a multimodal system that in- corporates MLD, short-stretch compression bandaging, skin care, therapeutic exercise, and elastic compression garments.23
2. Adhesive capsulitis
The diagnosis of adhesive capsulitis is made based on history and physical examination when other causes of pain and motion loss have been eliminated.24 Passive gleno- humeral motion is measured with the patient supine and with scapulothoracic motion constrained by manual pres- sure on the acromion. External rotation, abduction, and in- ternal rotation are most affected. Adhesive capsulitis is di- agnosed if limitation of passive external rotation of the hemiplegic shoulder of at least 20o is observed compared with the unaffected side.
3. Rotator cuff disease (RCD)
Patients with rotator cuff injuries frequently note anterior shoulder pain that occurs with overhead activity and at night while trying to sleep. Symptoms such as stiffness, weakness, and catching may also be present. If the Hawkins’ test, supraspinatus test, and Neer’s test, which have good sensitivity and specificity, are positive, patients are directed to obtain diagnostic imaging with ultra- sonography. RCD, including rotator cuff tendonitis or ten- dinopathy, subacromial impingement, and calcific tendoni-
tis, was diagnosed with ultrasonography as defined by Soble et al.25 Manual approaches such as stretching, mas- sage, or active and passive ROM exercises are generally recommended for treatment. Pharmaceutical interventions such as nonsteroidal anti-inflammatory drugs (NSAIDs), tramadol, or, potentially opioid analgesic trials may be add- ed on physical therapies to minimize functional limitations.
Interventional procedures may include triggering point in- jections, intra-articular or subacromial injection, or capsular distention.
MPS
MPS is a regional pain syndrome characterized by the presence of myofascial trigger points. MPS is determined by the presence of distinctive clinical characteristics of my- ofascial trigger points, which include circumscribed spot tenderness in a nodule that is part of a palpably tense band of muscle fibers, patient recognition of the pain evoked by pressure on the tender spot as familiar, referred pain in the pattern characteristic of trigger points in that muscle, a lo- cal twitch response, painful restriction of stretch ROM, and some weakness of that muscle.26
PECTORALIS TIGHTNESS
The evaluation of pectoralis tightness consisted of meas- urements of passive shoulder ROM, including forward flexion, external rotation, and horizontal extension, made with a goniometer according to a standardized protocol. In the absence of definitive diagnostic criteria to rule out pec- toralis tightness or to establish the degree of limitation en- suing from this condition,27 pectoralis tightness was defined as the presence of limitation of forward flexion by more than 10o, with no limitation of external rotation and limited horizontal abduction of more than 10o based on our clinical experience. Horizontal abduction was defined as the max- imal degree of scapular retraction in the horizontal plane with 90o of elbow flexion and 90o of shoulder abduction.
Manual approaches such as stretching, massage, or active and passive ROM exercises are generally recommended for treatment. Interventional procedures may include triggering point injections. Pharmaceutical interventions such as NSAIDs may be added on physical therapies to minimize functional limitations.
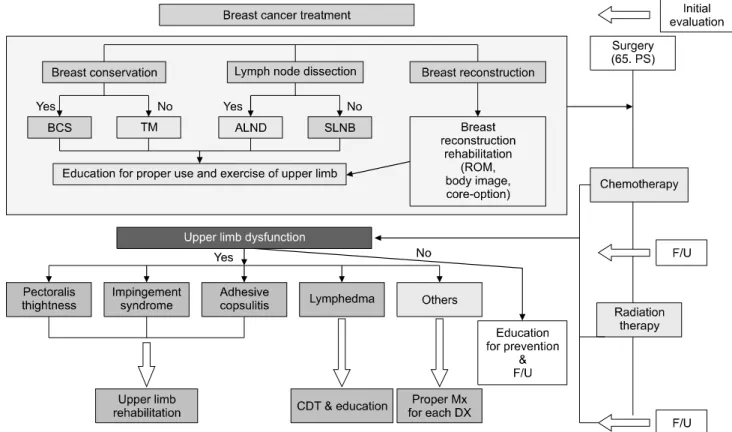
Fig. 2. Clinical pathway for rehabilitation of breast cancer patients focused on the upper limb dysfunction. BCS: breast conserving surgery, TM: total mastectomy, ALND: axillary lymph node dissection, SLNB: sentinel lymph node biopsy, CDT: complex deconges- tive therapy, Text book: instructions on lymphedema prevention and upper limb dysfunction.
POST-MASTECTOMY PAIN SYNDROME (PMPS)
PMPS is a chronic pain condition, typically neuropathic in nature, which can occur following breast surgery.28,29 Chronic pain was defined as PMPS based on its character- istics, location, and timing, using the same criteria at each time point to ensure comparability. Pain was assessed for neuropathic characteristics, including numbness, pins and needles, burning, and stabbing. Pain location was recorded as being on the same side as the surgery, on the chest wall, at the axilla, or on the ipsilateral arm. Chronic pain was defined as continuous or intermittent pain that persisted for longer than the normal healing time of 3 months.
AXILLARY WEB SYNDROME (AWS)
AWS was diagnosed based on the presence of taut, pal- pable cords originating in the axilla and extending distally along the anterior surface of the arm, often below the
elbow.30 Pain generally responds to NSAIDs. Opioid an- algesics might be necessary during passive and active as- sisted ROM if the pain is severe. Therapy involves in- cremental ROM activities, topical heat, manipulation to soften and potentially ‘pop’ the cords, and provision with a home exercise program.30
CLINICAL PATHWAY FOR ULD (Fig. 2)
(1) Patients with breast cancer received cancer treatment were classified into several groups according to breast con- servation, axillary lymph node dissection and breast reconstruction. (2) Patients were evaluated whether ULD was developed or not in the OPD clinic visit after surgery.
(3) Patients were treated or educated according to the ULD.
In the periodic follow-up in the clinics of surgery, medical oncology, radiation oncology, rehabilitation and plastic sur- gery, history taking and physical examination to detect any problems related to cancer treatment were performed. If the diagnosis of ULD such as pectoral muscle tightness, RCD,
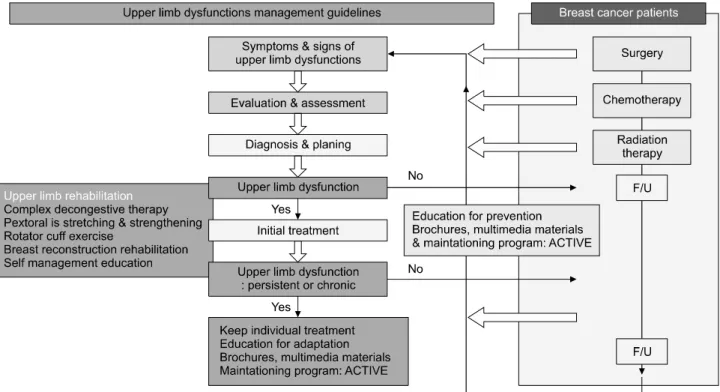
Fig. 3. Rehabilitation program according to the severity of upper limb dysfunction of breast cancer patients.
adhesive capsulitis, lymphedema, etc. got it done, stand- ardized therapy was provided (refer to treatment part). If lymphedema was found, CDTand education were provided.
Possible complications other than these dysfunctions were also investigated while they were followed up. For PMPS, neuropathic pain medication and desensitization technique were applied. In AWS, mobilization of band like fibrotic or collected lesion was provided. Even if not frequent, axil- lary or long thoracic nerve injury was developed usually in extensive surgery cases. In the first visit, if definite dys- function was not detected, the prevention strategy for lym- phedema or other potential ULD kept going on. (4) Patients were reevaluated whether ULD was developed or not and check the change of function at 2nd (6 month) follow-up (5) Bio-Psycho-Social model approach is necessary.
ULDs MANAGEMENT GUIDELINES (Fig. 3)
ULD may be seen at various treatment phases so, assess- ment coincides with standard follow-up appointments for disease management and recurrence surveillance from diagnosis. If functional limitations are noted, the types of ULD are diagnosed and categorized based on symptoms,
physical examinations and assessment of pain and dis- abilities. Individualized rehabilitation intervention could be initiated. After finishing primary treatment, reassessment visit also provides to evaluate the change of function. If there is no ULD, baseline tests and measures are repeated at each follow-up visit in an effort to identify changes and to detect early signs of ULD as the surveillance program.
This reassessment visit also provides an opportunity for pa- tient education on prevention and early detection of com- mon ULDs as well as education about exercise and health-promoting behaviors using multimedia and brochures.
If the dysfunctions are sustained and changed to chronic states, education of accommodation may be more effective approach than trying to be completely cured.
MEANING OF THE MULTIDISCIPLINARY CARE SYSTEM
Our multidisciplinary care system for ULD for breast cancer patients provide early detection and proper treat- ment for ULD which may be developed in all treatment phases. Building cooperating system with multisectoral and multidisciplinary approach, our care system could provide
comprehensive and continuous care system from pre- vention to rehabilitation. By reducing the prevalence and severity of ULD, our system could improve QoL of cancer patients and decrease medical cost. The perception about QoL of cancer patients has been changed. With functional approach, it is needed to establish guideline for supportive cancer care with communication between the disciplines.
Increases in life expectancy for women with breast cancer have emphasized the need for improved QoL for women during or after breast cancer treatment. Physical function is one of the strongest determinants of health-related QoL.
The term “function” refer to a patient’s ability to function in life; for example, impairments in body functions and body structures including shoulder pain, limitation of ROM,31 or lymphedema32 can negatively affect the in- dividuals’ self-image,33 the relationship with the partner and can lead to social isolation.34 Functional outcome is in- fluenced by a wide variety of different factors. A number of cancer- and treatment-related aspects affect functional outcome including tumor site, stage, operative procedures, use of radio(chemo)therapy and recurrence. Therefore, it is needed that comprehensive and multisectoral approach for diagnosis and management of dysfunction in cancer patients. Now, it is the time to evaluate the current func- tional states of cancer survivors and develop treatment strategies to improve physical and psychosocial functions of cancer survivors. However, there is lack of medical and social consensus about cancer rehabilitation. Cheville and Tchou35 reported that the increasing emphasis on quality survivorship is an opportunity for cancer rehabilitation, bar- riers to rehabilitation arise from human, academic, logistic and financial sources. Our care system has significance be- cause the ULD is referred from multisectoral joint treat- ment by changing the perception about function and QoL of medical oncologists, surgeon, radiation oncologist, plas- tic surgeon and psycho-oncologist through diagnosis to sur- vivorship phase and may be developed as a good model for cancer rehabilitation.
CONCLUSION
We developed the multidisciplinary care system for early detection and proper diagnosis of ULD after breast cancer treatment and the continuous management system including prevention, diagnosis and rehabilitation program. By re-
ducing the prevalence and severity of ULD, our system could improve QoL of cancer patients and decrease medi- cal cost. To assess the effectiveness of our multidiscipli- nary care system, a randomized controlled trial is needed.
REFERENCES
1. Yang EJ, Kim BR, Shin HI, Lim JY. Use of the interna- tional classification of functioning, disability and health as a functional assessment tool for breast cancer survivors. J Breast Cancer 2012; 15: 43-50
2. Yang EJ, Park WB, Seo KS, Kim SW, Heo CY, Lim JY.
Longitudinal change of treatment-related upper limb dys- function and its impact on late dysfunction in breast cancer survivors: a prospective cohort study. J Surg Oncol 2010;
101: 84-91
3. Blomqvist L, Stark B, Engler N, Malm M. Evaluation of arm and shoulder mobility and strength after modified radi- cal mastectomy and radiotherapy. Acta Oncol 2004; 43:
280-283
4. Satariano WA, Ragland DR, DeLorenze GN. Limitations in upper-body strength associated with breast cancer: a com- parison of black and white women. J Clin Epidemiol 1996;
49: 535-544
5. Larson D, Weinstein M, Goldberg I, Silver B, Recht A, Cady B, et al. Edema of the arm as a function of the extent of axillary surgery in patients with stage I-II carcinoma of the breast treated with primary radiotherapy. Int J Radiat Oncol Biol Phys 1986; 12: 1575-1582
6. Erickson VS, Pearson ML, Ganz PA, Adams J, Kahn KL.
Arm edema in breast cancer patients. J Natl Cancer Inst 2001; 93: 96-111
7. Yang EJ, Park WB, Seo KS, Kim SW, Heo CY, Lim JY.
Longitudinal change of treatment-related upper limb dys- function and its impact on late dysfunction in breast cancer survivors: a prospective cohort study. J Surg Oncol 2010;
101: 84-91
8. Swedborg I, Wallgren A. The effect of pre- and post- mastectomy radiotherapy on the degree of edema, should- er-joint mobility, and gripping force. Cancer 1981; 47:
877-881
9. Stubblefield MD, Schmitz KH, Ness KK. Physical func- tioning and rehabilitation for the cancer survivor. Semin Oncol 2013; 40: 784-795
10. Stout Gergich NL, Pfalzer LA, McGarvey C, Springer B, Gerber LH, Soballe P (2008) Preoperative assessment en- ables the early diagnosis and successful treatment of lymphedema. Cancer 112(12): 2809–2819
11. Stout NL, Binkley JM, Schmitz KH, Andrews K, Hayes
SC, Campbell KL, et al. A prospective surveillance model for rehabilitation for women with breast cancer. Cancer 2012; 118(8 Suppl): 2191-2200
12. Yun YH, Mendoza TR, Heo DS, Yoo T, Heo BY, Park HA, et al. Development of a cancer pain assessment tool in Korea: a validation study of a Korean version of the brief pain inventory. Oncology 2004; 66: 439-444
13. Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am J Ind Med 1996; 29: 602-608
14. Lee JY, Lim JY, Oh JH, Ko YM. Cross-cultural adaptation and clinical evaluation of a Korean version of the dis- abilities of arm, shoulder, and hand outcome questionnaire (K-DASH). J Shoulder Elbow Surg 2008; 17: 570-574 15. Gjorup C, Zerahn B, Hendel HW. Assessment of volume
measurement of breast cancer-related lymphedema by three methods: circumference measurement, water displacement, and dual energy X-ray absorptiometry. Lymphat Res Biol 2010; 8: 111-119
16. International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema. 2009 Consensus Document of the International Society of Lymphology.
Lymphology 2009; 42: 51-60
17. Yang EJ, Ahn SY, Kim EK, Kang EY, Park Y, Lim JY, Kim SW. Use of a prospective surveillance model to pre- vent breast cancer treatment-related lymphedema: a sin- gle-center experience. Breast Cancer Res Treat 2016; 160:
269-276
18. Yun YH, Bae SH, Kang IO, Shin KH, Lee R, Kwon SI, et al. Cross-cultural application of the Korean version of the European Organization for Research and Treatment of Cancer (EORTC) Breast-Cancer-Specific Quality of Life Questionnaire (EORTC QLQ-BR23). Support Care Cancer 2004; 12: 441-445
19. Dirmaier J, Zaun S, Koch U, Harfst T, Schulz H.
Psychometricproperties of the EORTC Quality of Life Questionnaire in inpatient cancer rehabilitation in Germany.
Palliat Support Care 2004; 2: 115-124
20. Montazeri A, Harirchi I, Vahdani M, Khaleghi F, Jarvandi S, Ebrahimi M, et al. The EORTC breast cancer-specific quality of life questionnaire (EORTC QLQ-BR23): trans- lation and validation study of the Iranian version. Qual Life Res 2000; 9: 177-184
21. Michels FA, Latorre Mdo R, Maciel Mdo S. Validity, reli- ability and understanding of the EORTC-C30 and EORTC-BR23, quality of life questionnaires specific for breast cancer. Rev Bras Epidemiol 2013; 16: 352-363 22. Zawisza K, Tobiasz-Adamczyk B, Nowak W, Kulig J,
Jedrys J. Validity and reliability of the quality of life ques- tionnaire (EORTC QLQ C30) and its breast cancer module (EORTC QLQ BR23). Ginekol Pol 2010; 81: 262-267 23. Bernas MJ, Witte CL, Witte MH; International Society of
Lymphology Executive Committee. The diagnosis and treatment of peripheral lymphedema: draft revision of the 1995 Consensus Document of the International Society of Lymphology Executive Committee for discussion at the September 3-7, 2001, XVIII International Congress of Lymphology in Genoa, Italy. Lymphology 2001; 34: 84-91 24. Rietman JS, Dijkstra PU, Geertzen JH, Baas P, De Vries
J, Dolsma W, et al. Short-term morbidity of the upper limb after sentinel lymph node biopsy or axillary lymph node dissection for Stage I or II breast carcinoma. Cancer 2003;
98: 690-696
25. Soble MG, Kaye AD, Guay RC. Rotator cuff tear: clinical experience with sonographic detection. Radiology 1989;
173: 319-321
26. Borg-Stein J, Simons DG. Focused review: myofascial pain. Arch Phys Med Rehabil 2002; 83(3 Suppl 1):
S40-S47, S48-S49
27. Kim SM, Park JM. Normal and abnormal US findings at the mastectomy site. Radiographics 2004; 24: 357-365 28. Smith WC, Bourne D, Squair J, Phillips DO, Chambers
WA. A retrospective cohort study of post mastectomy pain syndrome. Pain 1999; 83: 91-95
29. Macdonald L, Bruce J, Scott NW, Smith WC, Chambers WA. Long-term follow-up of breast cancer survivors with postmastectomy pain syndrome. Br J Cancer 2005; 92:
225-230
30. Moskovitz AH, Anderson BO, Yeung RS, Byrd DR, Lawton TJ, Moe RE. Axillary web syndrome after axillary dissection. Am J Surg 2001; 181: 434-439
31. Tasmuth T, von Smitten K, Kalso E. Pain and other symp- toms during the first year after radical and conservative sur- gery for breast cancer. Br J Cancer 1996; 74: 2024-2031 32. Kim MG, Lee HS. Growth-inhibiting activities of phenethyl
isothiocyanate and its derivatives against intestinal bacteria.
J Food Sci 2009; 74: M467-M471
33. Shimozuma K, Ganz PA, Petersen L, Hirji K. Quality of life in the first year after breast cancer surgery: re- habilitation needs and patterns of recovery. Breast Cancer Res Treat 1999; 56: 45-57
34. Knobf MT. Symptoms and rehabilitation needs of patients with early stage breast cancer during primary therapy.
Cancer 1990; 66(6 Suppl): 1392-1401
35. Cheville AL, Tchou J. Barriers to rehabilitation following surgery for primary breast cancer. J Surg Oncol 2007; 95:
409-418