PGHN
Original Article
A Clinical Study of the Relationship between Obesity and Pubertal Development in Girls
Hui Kwon Kim, M.D., Jong Yoon Lee, M.D., Eun Ju Bae, M.D., Won Il Park, M.D., Hong Jin Lee, M.D. and Phil Soo Oh, M.D.
Department of Pediatrics, Hallym University Medical Center, Chuncheon, Korea
Purpose: Recently, public interest in obesity and earlier pubertal development has been increasing. The purpose of this study was to analyze the relationship between obesity and pubertal development in girls.
Methods: A total of 158 girls presenting with earlier pubertal development from July 2008 to June 2010 were included in the study. Their mean age was 8.27±1.3 years and the mean bone age advancement was 1.86±0.3 years.
Results: Based on weight-for-height percentiles, their obesity rate was 9.2% and overweight rate was 15.8%.
However, for body mass index (BMI), the result was a bit different; with an obesity rate of 13.2% and overweight rate of 24.3%. About 40% of the girls had a family history of early maturation. Among them, 25.7% had a maternal history, 4.6% paternal and 7.2% both. However, 60% of them had no family history. We then classified these girls into families with one son and one daughter, and those with two daughters. In one-son/one-daughter families, 69.3%
were the first children and 30.7% were second. In two-daughter families, 65.3% were the first and 34.7% were second.
We found that 67.5% had a history of taking herbal medicine.
Conclusion: The obesity and overweight rates in girls with earlier pubertal development were higher than those of normal girls, but with a small discrepancy between weight-for-height percentile and BMI-based results. Furthermore, taking herbal medicine seems to be a potential factor for earlier pubertal development in Korea. (Pediatr Gastroenterol Hepatol Nutr 2012; 15: 175∼182)
Key Words: Earlier pubertal development, Obesity, Weight-for-height percentile, Body mass index, Herbal medicine
Received:March 21, 2012, Revised:June 14, 2012, Accepted:July 3, 2012
Corresponding author: Phil Soo Oh, M.D., Department of Pediatrics, Hallym University Medical Center, 77 Sakjooro, Chuncheon 200-704, Korea. Tel: +82-33-240-5169, Fax: +82-33-255-6244, E-mail: [email protected]
Copyright ⓒ 2012 by The Korean Society of Pediatric Gastroenterology, Hepatology and Nutrition
This is an openaccess article distributed under the terms of the Creative Commons Attribution NonCommercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
INTRODUCTION
Recently, public interest in earlier pubertal develop- ment has been increasing. The onset age of puberty is affected by genetic factors, nutritional status, obe-
sity, environmental hormones, and stress. As the standard of living has improved in Korea, an earlier onset of puberty is the trend [1]. This is particularly distinct for girls, and it has been reported to be asso- ciated with increased leptin due to obesity [2,3].
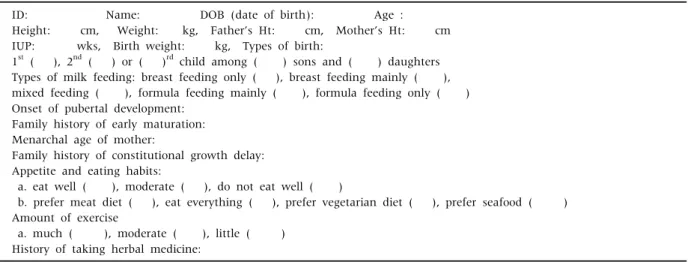
Table 2.Questionnaires
ID: Name: DOB (date of birth): Age :
Height: cm, Weight: kg, Father’s Ht: cm, Mother’s Ht: cm IUP: wks, Birth weight: kg, Types of birth:
1st ( ), 2nd ( ) or ( )rd child among ( ) sons and ( ) daughters Types of milk feeding: breast feeding only ( ), breast feeding mainly ( ), mixed feeding ( ), formula feeding mainly ( ), formula feeding only ( ) Onset of pubertal development:
Family history of early maturation:
Menarchal age of mother:
Family history of constitutional growth delay:
Appetite and eating habits:
a. eat well ( ), moderate ( ), do not eat well ( )
b. prefer meat diet ( ), eat everything ( ), prefer vegetarian diet ( ), prefer seafood ( ) Amount of exercise
a. much ( ), moderate ( ), little ( ) History of taking herbal medicine:
Table 1. Characteristics of the Subjects
Variables Girls (N=158)
Age (yr) Height (cm) Height percentiles Weight (kg)
Weight-for-height percentiles Body mass index (kg/m2) BA advancement (BA-CA) BA advancement: <1 yr BA advancement: 1-2 yr BA advancement: 2-3 yr BA advancement: >3 yr Paternal height (cm)
Maternal height (cm)
8.27±1.3 132.6±8.5 77.7±19.1*
32.3±7.9 54.38±26.7*
18.14±2.8 1.86±0.3 11 (7.0) 80 (50.6) 58 (36.7) 9 (5.7) 172.6±5.3 159.5±4.6 Values are presented as mean±standard deviation or n (%).
BA: bone age, CA: chronological age. *p-value <0.0001.
Because earlier pubertal development affects phys- ical status and mental status, parents have been tak- ing a growing interest in it [4]. The purpose of this study was to analyze the obesity and overweight rates with their clinical characteristics in girls with earlier pubertal development by using physical examina- tions and questionnaires.
MATERIALS AND METHODS
Subjects
A total of 158 girls presenting with earlier pubertal development from July 2008 to June 2010 were in- cluded in the study. Among them, 78 girls whose pu- bertal development had started before age 8 were di- agnosed with precocious puberty and the other 80 girls whose pubertal development had started at 8-9 years of age were diagnosed with early puberty. All of the 78 girls with precocious puberty had no under- lying disease, so the cause was not different from the early puberty group, that is, just an early activation of the hypothalamic-pituitary-ovarian axis. Recently in Korea, insurance has been covering girls diagnosed before age 9 by the luteinizing hormone-releasing hormone (LHRH) stimulation test. Therefore, we grouped those who breast budding started before 9 years of age without underlying disease, that is, the precocious and early pubertal development groups
together, into one earlier pubertal development group and analyzed them (Table 1) [5].
Methods
When new patients presented with earlier pubertal development, we measured their chronological age, bone age, height and weight. Meanwhile, their pa- rents completed questionnaires (Table 2). Height was measured to the closest 0.1 cm by using a Harpenden stadiometer (Holtain, Crymych, UK) and weight was measured with a GL-6000-20 scale (CAS, Seoul, Korea). Bone age was calculated with the Greulich-
Fig. 1. Height percentiles of girls with earlier pubertal develop- ment.
Fig. 2. Weight-for-height percentiles of girls with earlier pubertal development.
Pyle atlas. Based on their answers for the ques- tionnaires, we verified them and rechecked some ad- ditional questions, if necessary. For examples, the height of parents was confirmed by asking again and the mother’s early maturation was also verified by questioning about the menarchal age again by check- ing how much different it was from the mother’s friends. In addition, the father’s early maturation or constitutional growth delay was also verified by ask- ing about their growth spurt again.
Statistical analyses
Every analysis was carried out by using SAS ver- sion 9.1.3 software (SAS Institute, Cary, NC, USA).
Each result was presented by means of descriptive statistics. The statistical analysis of categorical varia- bles was performed with the chi-squared test for ver- ifying a categorical ratio, and a paired t-test was per- formed in order to compare their height percentiles with weight-for-height percentiles. All statistical tests were two-sided, and the level of significance was α=0.05. Therefore, a p-value less than 0.05 was considered statistically significant.
RESULTS
General characteristics
The mean age of the 158 girls was 8.27±1.3 years
and their mean bone age advancement was 1.86±0.3 years. Among the cases, 11 (7.0%), 80 (50.6%), 58 (36.7%), and 9 (5.7%) had a bone age advancement of less than 1 year, 1-2 years, 2-3 years, and more than 3 years, respectively. Meanwhile, the mean height of their fathers and mothers was 172.6±5.3 cm and 159.5±4.6 cm, respectively (Table 1).
Height and weight distributions
Based on weight-for-height percentiles, 9.2% were obese, which was defined as above the 95th percen- tile, 15.8% were overweight which was defined as 85th-95th percentile and therefore the obesity plus overweight rate was 25%. Analyzing the same group regarding body mass index (BMI), 13.2% and 24.3%
were above the 95th and between the 85th to 95th percentiles, respectively, and therefore the obesity plus overweight rate measured by BMI was 37.5%, a bit different from the results according to the weight-for-height percentiles. The height percentiles of the girls were mostly more than 50, as expected (Fig. 1), but a considerable number had weight- for-height percentiles within 25-50 (27%) or 50-75 (26.3%) (Fig. 2). To compare their height percentiles and weight-for-height percentiles, the median of the interval of the percentiles were averaged for each, and the mean of their height percentiles, at 77.7±
19.1, was statistically higher than the mean of their
Fig. 3. Types of milk feeding in infancy.
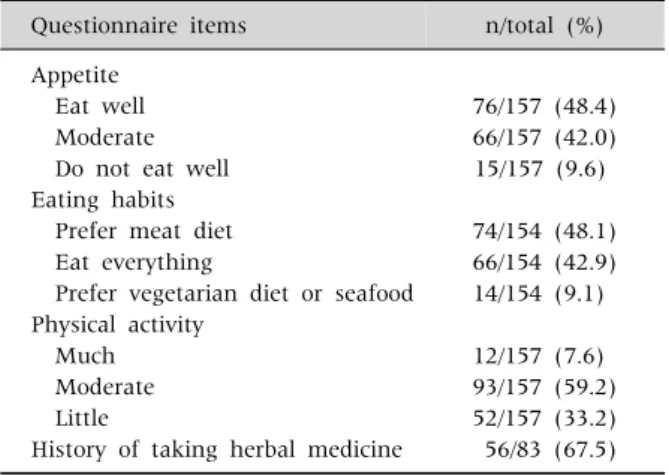
Table 3. Appetite, Eating Habits, Physical Activity, and History of Taking Herbal Medicine
Questionnaire items n/total (%)
Appetite Eat well Moderate Do not eat well Eating habits Prefer meat diet Eat everything
Prefer vegetarian diet or seafood Physical activity
Much Moderate Little
History of taking herbal medicine
76/157 (48.4) 66/157 (42.0) 15/157 (9.6)
74/154 (48.1) 66/154 (42.9) 14/154 (9.1)
12/157 (7.6) 93/157 (59.2) 52/157 (33.2) 56/83 (67.5)
Table 4.Family History of Girls with Earlier Pubertal Develop- ment
Family history of early maturation n/total (%) Mother
Father
Mother and father Aunt
Mother's family Elder sister
Constitutional growth delay of father No family history
39/152 (25.7) 7/152 (4.6) 11/152 (7.2) 1/152 (0.7) 1/152 (0.7) 1/152 (0.7) 2/152 (1.3) 90/152 (59.2)
Table 5. Family Relationships of Girls with Earlier Pubertal Development
Family relationships n/total (%)
The first of one son/one daughter The first of two daughters The first of one daughter
The first of one son/two daughters The first of two son/one daughter The second of one son/one daughter The second of two daughters The second of one son/two daughters The second of three daughters The third of one son/two daughters The third of three daughters
45/149 (30.2) 32/149 (21.5) 22/149 (14.8) 2/149 (1.3) 2/149 (1.3) 20/149 (13.4) 17/149 (11.4) 2/149 (1.3) 2/149 (1.3) 3/149 (2.0) 2/149 (1.3)
weight-for-height percentiles, which was 54.4±26.7 (p-value <0.0001).
Types of milk feeding and eating habits The percentage of girls who had been only breast fed was 13.7%, mainly breast fed was 5.5%, who had a mix of breast feeding and formula was 34.3%, mainly formula fed was 32.9%, and only formula fed was 13.7% (Fig. 3). Most of them ate well or moder- ately, only 10% did not eat well. Meanwhile, 48.1%
preferred meat, 42.9% ate everything well, and only 9% preferred vegetables or seafood (Table 3).
Family history of early maturation
About 40% of the girls had a family history of early maturation. Among them, 25.7% had a maternal his- tory, 4.6% paternal and 7.2% both. However, 60% of them had no family history of early maturation (Table 4).
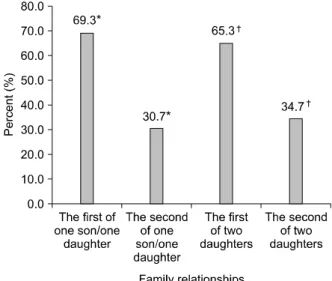
Family relationships of the girls
Among the girls, 30.2%, 21.5%, and 14.8% were the first child in families with one son and one daughter, the first child in families with two daughters, and the only child in families with one daughter, respectively.
Furthermore, 13.4% were the second child in families with one son and one daughter, 11.4% were the sec- ond child in families with two daughters (Table 5). By classifying these girls into families with one son and one daughter and those with two daughters, we ob- tained some interesting results. In one-son/one- daughter families, 69.3% were the first children and
Fig. 4. Family relationships of the girls with earlier pubertal development. *p-value=0.0019, †p-value=0.0321.
30.7 % were the second. In two-daughter families, 65.3% were the first and 34.7% were the second (Fig.
4). In each group, the number of oldest children who had earlier pubertal development was about twice as large as that of second children. The risk for earlier pubertal development was found to be statistically higher for the first children (p-value was 0.0019 in one-son/one-daughter families; p-value was 0.0321 in two-daughter families).
Intake of herbal medicine
Up to 67.5% of the girls had taken herbal medicine (Table 3).
Amount of exercise
Among the girls, 7.6%, 59.2% and 33.1% performed much, moderate and little activity, respectively (Table 3).
DISCUSSION
Recently, public interest in earlier pubertal devel- opment has been increasing due to the increasing number of girls experiencing it; thus, we investigated the phenomenon, focusing especially on obesity and overweight. On the other hand, some recent studies
have been reporting a relatively longer period of pub- erty; that is, the onset of puberty tends to come earlier than in the past but the onset of menarche does not necessarily come earlier [6].
With regard to obesity and nutritional status, it has been reported that obesity and fat accumulation would be major factors determining the onset of me- narche in early adulthood [7]. Physical factors (obesity, nutritional status or exercise) or psychoso- cial factors can affect the onset of puberty [8]. In par- ticular, excessive exercise can delay the onset of pub- erty in girls [9]. Frische and McArthur [10] reported that menarche can begin when the body fat takes up about 17% of body weight and amenorrhea could happen if body fat occupies less than about 22% of the body weight of women aged 16 years and over. In this study, to determine the rates of obesity and over- weight, we adopted both the methods of BMI and weight-for-height percentiles. BMI tended to be cal- culated as higher in this relatively tall group, as shown by the BMI (kg/m2) formula that reflects the weight of tall height [11,12]. Based on BMI, the obe- sity and obesity plus overweight rates were calculated to be 13.2% and 37.5%, respectively. According to some reports and data released from the Korean Centers for Disease Control, the recent prevalence of general elementary school girls' obesity was 5.5-8.0 % and their obesity plus overweight rate was 17.8-18.2% [13-15]. Therefore, we found that, using the BMI method, the obesity plus overweight rate was somewhat higher in girls with earlier pubertal development. Meanwhile, according to the data from the US, the rate of obesity, that is, a BMI above the 95th percentile and the obesity plus overweight rate, that is, a BMI above the 85th percentile was reported to be 15.5% (control 8.1%) and 34.4% (control 23.2%), respectively, in the group of early sexual ma- turation [16]. Those results were almost the same as ours. However, in the present study, the difference was that we also obtained obesity and overweight rates based on the weight-for-height percentiles and found a bit different results according to the method of analysis. Therefore, similar data should be ana- lyzed in light of this difference between the two obe-
sity and overweight rates. There have been some re- ports that BMI is positively correlated with earlier pu- bertal and breast development [7], and that puberty and menarche come earlier when in the groups with a higher percentage of body fat at age 5 [5], in those with a higher BMI at age 3 [17], and in those with higher weight gain during the 9 months after birth [18]. However, Laron et al reported that there was no evidence that weight was a critical factor for pubertal development [19]. Additionally, as shown in the fig- ures from this study, because their height percentiles were statistically higher than their weight-for-height percentiles, we suspected that there might be some other factors besides increased fat causing earlier pu- bertal development. In other words, although it was true that the obesity and overweight rates were high- er in this group, we conjectured that there might be some etiologic factors affecting their higher height percentiles. As we will discuss later, we suspected that some components of herbal medicine might cause weight gain, and also in previous studies, it was shown that phytoestrogen in ginseng and the like seemed able to induce growth hormone secretion for increasing height also [20,21]. Meanwhile, at the same time, because of early maturation of bone age due to phytoestrogen, eventually their final adult heights might be shorter, but during the growth peri- od they seemed to be taller and also heavier than their peers.
With regard to types of milk feeding and eating habits, the percentage of those receiving only breast feeding was 13.7% and mainly breast feeding was 5.5%, so the rates were lower than a report in Korea that the percentage of breast feeding during the first 3 months of age only increased from 28% in 1999 to 50% in 2005 [22,23]. Therefore we suspected that for- mula feeding in infancy might be a starting point for obesity or overweight which in turn could induce ear- lier pubertal development in the future [24,25]. At the same time, the vast majority (91%) of the girls preferred meat or ate everything well, while only 10%
did not eat well, so we observed the importance of nu- tritional status for maturation, but not necessarily being obese. Therefore, these results might be said to
have some connection with the reports that intake of a high protein diet such as one containing great deal of meat in childhood was related to earlier pubertal development [26,27].
In our study, the family history rate of early matu- ration was about 40%, which did not differ much from a longitudinal study showing a heritability of 0.49 [28]. Meanwhile, from another perspective, al- though correlation with some reports that chronic stress in the family might be a cause of earlier pu- bertal development was uncertain [9,29], the num- ber of oldest children with earlier pubertal develop- ment was statistically higher than that of second children in each group (Table 4), when classifying these girls into the families with one-son/one-daugh- ter and those with two daughters. This interesting finding might help inform medical counseling. This result has not been reported in the existing literature, so we conjectured that its correlation was an influ- ence of the environment of being raised as the first child.
With regard to herbal medicine, according to a re- cent article, most responses about herbal medicine intake were as follows: with herbal medicine, oral in- take and weight, but not height, increased; the pa- tients tended to report the feeling of “being a little healthier” and puberty was likely to develop earlier [30]. Meanwhile, although it was just reported in small scale study of 18 people who had taken herbal medicine for growth, there were only 10 cases of a growth rate increase after taking herbal medicine (55.6% of all 18 people, and among them 4 are girls [66.6%], 6 are boys [50.5%]). For all 10 people who had a growth rate increase, their BMI also increased, but there was no case in which the BMI decreased while the growth rate increased [31]. Therefore, ac- cording to that study, in all cases of a growth rate in- crease after taking herbal medicine, their BMI also increased, so these results of a height increase with weight gain were thought to be also followed by pro- gression of bone age inducing earlier pubertal development. On the other hand, there have been some reports that a main ingredient of ginseng, gin- senoside-Rb1, binds to estrogen receptors and acti-
vates them, so it could have estrogenic activity used for decreasing menopausal symptoms [20,21]. In some Korean reports, the experience of girls taking herbal medicine was reported to be about 33.2-62.0%
[32-34]; however, in our study the percentage taking herbal medicine was found to be 67.5%. To sum it all up, herbal medicine was thought likely to be a poten- tially harmful factor inducing earlier pubertal devel- opment in Korea.
With regard to exercise, it has been reported that the menarchal age of 15 ballet players was 15.4±1.9 years, which is later than that of girls in general, and it was also reported that the menarchal age of girls who are passive and like to lie around is younger than that of other girls [35]. Heavy exercise was found to cause pubertal delay for girls, and this was reported to result from a functional change in the hypo- thalamic-pituitary-ovarian axis; that is, a lack of pro- duction of estrogen due to the loss of normal secre- tion of luteinizing hormone [36,37]. The proportion of girls who actively did exercise was small (7.64%) in this study, so this was thought to be consistent with the above reports.
Taking into consideration the findings of the pres- ent study overall, data that agreed with previous re- ports were the similar rates of obesity and overweight as measured by BMI, the types of milk feeding, eating habits, family history of early maturation and the amount of exercise. However, what was different was the somewhat different rates of obesity and over- weight based on the weight-for-height percentiles in the same group, proving that their height percentiles were statistically higher than their weight-for-height percentiles, the finding that the number of oldest children who had earlier pubertal development was larger than that of the second children, and the fact that the girls who had earlier pubertal development had taken herbal medicine in greater quantities.
In conclusion, conventionally understood, we con- firmed higher rates of obesity and overweight in girls of earlier pubertal development. However, we de- termined that the results were somewhat different according to the method of analysis; specifically, the weight-for-height percentile method produced a
weak positive relationship, but the BMI method pro- duced a little stronger positive relationship. On the other hand, we could conclude that herbal medicine seemed to be a potential harmful factor inducing ear- lier pubertal development, but additional studies are needed to confirm this.
In this study, a few items in the questionnaire in- cluding the amount of exercise had some limitations for accurate analysis because they produced sub- jective answers from the perspective of the parents.
However, there was no better option because it is dif- ficult to obtain objective data from children. More specific questions, for example the numbers of times and length of time of performing exercise, would be needed for a more objective study. It would also be better to ask the parents to specify the ingredients of herbal medicine as accurately and specifically as possible. We hope that more scientific studies will ad- dress the potential role of herbal medicine and timing of pubertal development.
REFERENCES
1. Jeong MN, Lee YJ, Kim MS, Lee DY, Yeo CY, Kim CJ, et al. Causes of precocious puberty: multicenter study in Honam Area. J Korean Soc Pediatr Endocrinol 2009;14:30-7.
2. Park MJ. Update in the etiology and treatment of sexual precocity. Korean J Pediatr 2006;49:718-25.
3. Kaplowitz P. Precocious puberty: update on secular trends, definitions, diagnosis, and treatment. Adv Pediatr 2004;51:37-62.
4. Paik KH, Jin DK. Etiology and age incidence of preco- cious puberty. J Korean Soc Pediatr Endocrinol 2002;7:199-205.
5. Davison KK, Susman EJ, Birch LL. Percent body fat at age 5 predicts earlier pubertal development among girls at age 9. Pediatrics 2003;111:815-21.
6. Carlos M, Barbara V. The duration of puberty in girls is related to the timing of its onset. Pediatrics 1997;131:618-21.
7. Kaplowitz PB, Slora EJ, Wasserman RC, Pedlow SE, Herman-Giddens ME. Earlier onset of puberty in girls:
relation to increased body mass index and race.
Pediatrics 2001;108:347-53.
8. Anastasios P, Polyxeni N, Andreas F, George P.
Constitutional advancement of growth, early growth
acceleration, predicts early puberty and childhood obesity. J Clin Endocrinol Metab 2010;95:4535-41.
9. Bruce JE, Judy G. Psychosocial antecedents of varia- tion in girls’ pubertal timing: maternal depression, stepfather presence, and marital and family stress.
Child Development 2000;71:485-501.
10. Frisch RE, McArthur JW. Menstrual cycles: fatness as a determinant of minimum weight for height necessary for their maintenance or onset. Science 1974;185:949-51.
11. Bellizzi MC, Dietz WH. Workshop on childhood obesity:
summary of the discussion. Am J Clin Nutr 1999;70:
173S-5S.
12. Franklin MF. Comparison of weight and height rela- tions in boys from 4 countries. Am J Clin Nutr 1999;70:
157S-62S.
13. Moon KR. Diagnosis and treatment of childhood sbesity. Korean J Pediatr Gastroenterol Nutr 1999;2:
8-20.
14. Rho YI, Kim KH, Yang ES, Park YB, Park SK, Park J, et al. Prevalence of obesity and its relationship to diet on elementary students. Korean J Pediatr Gastroenter- ol Nutr 2000;3:181-7.
15. Oh KW, Jang MJ, Lee NY, Moon JS, Lee CG, Yoo MH, et al. Prevalence and trends in obesity among Korean children and adolescents in 1997 and 2005. Korean J Pediatr 2008;51:950-5.
16. Wang Y. Is obesity associated with early sexual matura- tion? A comparison of the association in American boys versus girls. Pediatrics 2002;110:903-10.
17. Lee JM, Appugliese D, Kaciroti N, Corwyn RF, Bradley RH, Lumeng JC. Weight status in young girls and the onset of puberty. Pediatrics 2007;119:e624-30.
18. Ong KK, Emmett P, Northstone K, Golding J, Rogers I, Ness AR, et al. Infancy weight gain predicts childhood body fat and age at menarche in girls. J Clin Endocrinol Metab 2009;94:1527-32.
19. Laron Z. Is obesity associated with early sexual matura- tion? Pediatrics 2004;113:171-2.
20. Lee YJ, Jin YR, Lim WC, Park WK, Cho JY, Jang S, et al. Ginsenoside-Rb1 acts as a weak phytoestrogen in MCF-7 human breast cancer cells. Arch Pharm 2003;26:58-63.
21. Ji SM, Lee YJ. Estrogen, androgen and retinoic acid hor- mone activity of ginseng total saponin. J Ginseng 2003;27:93-7.
22. Jung JH, Lee K. A survey on mothers' perception of breastfeeding. Korean J Pediatr 1999;42:1050-5.
23. Park EY, Cho SJ, Lee K. Current understanding and practices of breast feeding by mothers. Korean J Pediatr 2005;48:1162-5.
24. Gilka J, Gajduskova V, Malikova M, Masek J, Docekalova H, Hais R, et al. Foreign substances in the meat and organs of bulls and pigs fed with pastes made from household and food industry waste in addition to pastes made from poultry droppings. Vet Med (Praha) 1987;32:721-30.
25. Stoll BA. Western diet, early puberty and breast cancer risk. Breast Cancer Res Treat (England) 1998;49:
187-93.
26. Rogers IS, Northstone K, Dunger DB, Cooper AR, Ness AR, Emmett PM. Diet throughout childhood and age at menarche in a contemporary cohort of British girls.
Public Health Nutr 2010;13:2052-63.
27. Renu G, Suzanne MS. Consumer concerns about hor- mones in food. BCERF Fact Sheet No. 37. New York:
Cornell University Sprecher Institute for Comparative Cancer Research, 2000.
28. Towne B, Czerwinski SA, Demerath EW, Blangero J, Roche AF, Siervogel RM. Heritability of age at me- narche in girls from the Fels longitudinal study. Am J Phys Anthropol 2005;128:210-9.
29. Walvoord EC. The timing of puberty: is it changing?
does it matter. J Ado Health 2010;47:433-9.
30. Huh K, Park MJ. Questionnaire-based analysis of growth-promoting attempts among children visiting a university growth clinic. Korean J Pediatr 2009;52:
576-80.
31. Jeong MJ, Gok SY, Lee SY. Pilot study of effect to the growth after the administration of herbal medicine to the prepuberty children. J Korean Oriental Pediatrics 2008;22:25-34.
32. Ahn YJ. A study of elementary school pupils using tradi- tional herbal medicines. Korean J Pediatr 2007;50:
381-5.
33. Ahn YJ, Kim EY, Moon KR. A study on the utilization of complementary and alternative medicine for elemen- tary children Korean J Pediatr 2009;52:1103-8.
34. Lee MC, Kim MJ, Choi MJ, Cheuh HW, Yoo JH.
Complementary therapies and perceptions of growth in parents and children visiting the growth clinic. J Korean Soc Pediatr Endocrinol 2008;13:73-80.
35. Michelle PW. The effects of exercise on pubertal pro- gression and reproductive function in girls. J Clin Endocrinol Metab 1980;51:1150-7.
36. Theintz GE. Endocrine adaptation to intensive physical training during growth. Clin Endocrinol 1994;41:267-72.
37. Stafford DE. Altered hypothalamic-pituitary-ovarian axis function in young female athletes: implications and recommendations for management. Treat Endocrinol 2005;4:147-54.