Analysis of Outcomes and Prognostic Factors
Associated with Surgical Treatment Plus Postoperative Radiation Therapy for Stage II/III Pancreatic Cancer
Purpose: To evaluate treatment outcomes for patients with stage II/III pancreatic cancer who are treated with radiation therapy (RT) with or without chemotherapy (CTx) following surgery.
Methods: We retrospectively analyzed data from 17 patients who underwent surgery and post-operative RT with or without CTx between January 2000 and December 2008. Seven patients (41%) had stage II cancer and 10 (59%) had stage III cancer. Most were male (13 of 17; 76.5%). Age at diagnosis ranged from 42 to 82 (median 69) years. Whipple’s operation was done in 9 patients (53%), distal pancreatectomy in 7 (41%), and subtotal pancreatectomy in 1 (6%). All patients received RT using a three-dimensional RT technique to spare critical normal structures. Median radiation dose was 54 Gy (range, 50.4∼55.8 Gy). Variable CTx regimens were combined in 10 patients (58.8%); 5-FU in 4, UFTE-G in 4, gemcitabine in 1, and xeloda in 1. Acute toxicity was evaluated according to RTOG toxicity criteria. Survival analysis was done using the Kaplan-Meyer method. Univariate and multivariate prognostic factor analysis were done, respectively, using a log-rank test and Cox’s proportional hazards model.
Results: The median follow-up period was 12.6 months. Locoregional and distant failures occurred in 8 (47.1%) and 8 patients (47.1%), respectively. Five patients (29.4%) developed both loco-regional recurrence and distant metastasis. The metastatic sites were liver in 4 patients, lung in 3, peritoneum in 1, and kidney in 1. Median overall survival (OS) was 12.6 months.
The 1- and 2-year OS rates were, respectively, 58.8% and 24.5%. Median disease-free survival (DFS) was 8.3 months and the 1- and 2-year DFS rates were 46.3% and 30.9%, respectively.
The 2-year OS was not different between RT and RT with CTx : survival rates were 28.6%
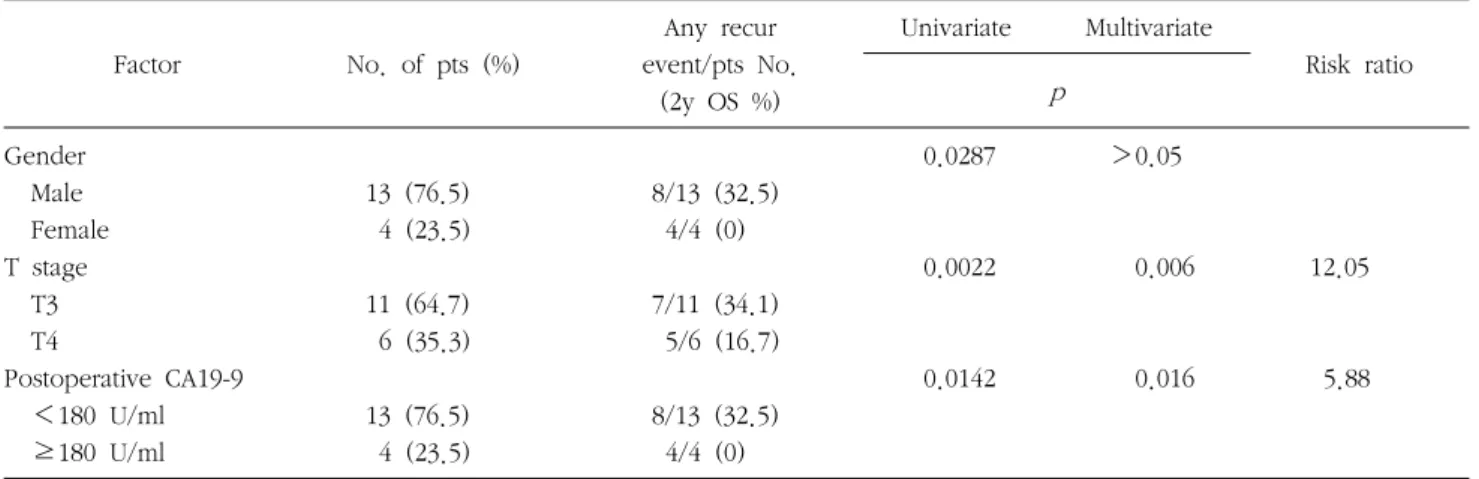
and 17.5%, respectively (p=0.764). T stage and a postoperative CA 19-9 level of ≥180 U/ml were significant prognostic factors for OS in both univariate and multivariate analysis: the 2-year OS for T3 and T4 were 34.1% and 16.7%, respectively (p=0.0022), the 2-year OS for <180 and ≥180 U/ml were 32.5% and 0%, respectively (p=0.0142) Acute toxicities were RTOG grade 1 (G1) nausea in 1 patient (5.9%), G1 vomiting in 2 (11.8%), and G1-2 enteritis in 5 (29.4%).
The hematologic toxicities were G1 leukopenia in 5 patients (29.4%), G2 leukopenia 1 (5.9%), G1 thrombocytopenia in 1 (5.9%), and G1∼2 anemia in 6 (35.3%).
Conclusion: Survival results of the present study are comparable to those in other reports with acceptable toxicity. Significant prognostic factors for overall survival in pancreatic cancer are tumor stage and postoperative CA 19-9 level.
Seok Ho Lee, M.D.1, Seung Heon Lee, M.D.1, Kyu Chan Lee, M.D.1, Yeon Ho Park, M.D.2, Gun Kook Kim, M.D.2, Jeong Nam Lee, M.D.2, Yang Seo Goo, M.D.3, Yeon Seok Kim, M.D.3, Sun Jin Shim, M.D.3, Dong Bok Shin, M.D.3, Jung Ho Kim, M.D.4, Dong Hae Chung, M.D.5
Departments of 1Radiation Oncology,
2Surgery, 3Internal Medicine, 4Radiology,
5Pathology, Gacheon University Gil Hospital
Corresponding Author Seok Ho Lee
Department of Radiation Oncology, Gacheon University Gil Hospital, 1198, Guwol-dong, Namdong-gu, Incheon 405-760, Korea
Tel: +82-32-460-3030 Fax: +82-32-460-3029
E-mail: [email protected]
*The Best Poster Awards at the 2010 Spring Conference.
Key Words : Pancreatic cancer, Radiation therapy, Chemotherapy
Received: 2010. 6. 7 Accepted: 2010. 7. 1
Table 1. Patients characteristics
Characteristics No. of pts (%) Age (years)
Median Range
69 42∼82 Gender
Male Female Surgery
Whipple's operation Distal pancreatectomy Subtotal pancreatectomy Tumor location
Head and neck Body and tail Stage
II III T stage 3 4
ECOG performance status 1
2 3 Weight loss Negative Positive
Postoperative CA 19-9 <180 U/ml ≥180 U/ml RT dose ≤50.4 Gy >50.4 Gy
13 4 9 7 1 11 6 7 10 11 6 8 7 2 12 5 13 4 2 15
76.5 23.5 53 41 6 64.7 35.3 41 59 64.7 35.3 47 41 12 70.6 29.4 76.5 23.5 11.8 88.2
Introduction
The prognosis for pancreatic cancer remains very poor.1 The reported 5-year overall survival rate of these patients was approximately 20%.2 In Korea, pancreatic cancer constituted 2.4% of all cancers diagnosed in males and females in 2007.3 The crude incidence rates have increased in parallel for both genders between 1999 and 2007. The surgery remains the primary therapy, but only 10∼15% of patients are possibly resectable. The local failure was reported in 50∼86% of patients who did not receiving the postoperative adjuvant therapy.4 Therefore, surgery alone is considered as an inadequate procedure for long-term disease control, and these poor outcomes of patient with pancreatic cancer would suggest a role for adjuvant therapy to improve the survival. The first randomized controlled trial on adjuvant radiation therapy (RT) for pancreatic cancer was performed by Gastrointestinal Tumor Study Group (GITSG).5 They reported that the median overall survival was 21 months with concurrent chemoradiation therapy (CCRT) compared with 11 months with surgery alone. However, the role of RT on overall survival still remains questionable. Although systemic relapse is a predominant feature for pancreatic cancer, radiation dose escalation could decrease the local and regional failures in selected patients,6 respectively. In the present study, we reported our experience of post-operative RT using rela- tively high radiation dose with or without chemotherapy (CTx) was retrospectively analyzed for patients with stage II, III pancreatic cancer.
Methods
1. Patients
Between January 2000 and December 2008, 17 patients at Gachon University Gil Hospital underwent surgery for pancreatic cancer followed by RT with or without CTx. In patients suspected pancreatic cancer, computed tomogra-
phy (CT) scanning was used to determine resectability. All patients had a histologic diagnosis of carcinoma before RT.
Histologically, 94% had adenocarcinoma, and 6% had papillary-mucinous carcinoma. Patient’s age ranged from 42 to 82 year with a median age of 69 years. Thirteen patients were male and 4 were female (male/female ratio, 3.25:1).
Patient characteristics are shown in Table 1. No patients were found to have metastatic disease. All pancreatic cancer cases were staged according to the 6th edition of the American Joint Committee on Cancer staging system.7 The
pathologist reviewed all tumors to assess the tumor size, presence or absence of lymph node metastasis, surgical margin status, perineural and lymphatic invasion.
Follow-up period ranged from 3.1 to 79.8 months. Six to 12 weeks after treatment completion, the patients under- went CT scan or MRI of abdomen and tumor marker study (CA19-9 and carcinoembryonic antigen) for a routine follow-up. First recurrences were defined as local, regional, or distant. A local failure was defined as any tumor recurrent disease at the primary sites (following RT).
Locoregional failure was defined as failure in either local or regional sites. The median follow-up period was 12.6 months. Toxicity experienced during adjuvant therapy was evaluated using the RTOG/EORTC toxicity criteria.
2. Surgery
Seventeen patients underwent a curative resection for pancreatic carcinoma. Whipple’s operation was performed in 9 patients (53%), distal pancreatectomy in 7 (41%), and subtotal pancreatectomy in 1 (6%). The margin status and the closest distance of tumor cells to any surgical resection margin were determined by at least one pathologist. Five patients underwent a curative resection with negative margins. Twelve patients (70.6%) had lymph node meta- stasis, and 5 patients had none.
3. Radiation Therapy and Chemotherapy All patients received external beam RT with megavoltage equipment (10 MV X-ray). All the patients received RT using a three-dimensional RT technique (3D-CRT) to spare critical normal structures (kidney, liver etc). Doses were limited to less than 50% of liver volume receiving more than 45 Gy. At least two thirds of one kidney was spared from RT fields and the spinal cord was limited to less than 45 Gy. The tumor bed (including the involved pancreatic resection margin) and regional lymphatics (celiac axis, distal portal vein, and superior mesenteric vein) received 45 Gy in 1.8 G per fraction, and then the tumor bed was boosted to a total 50.4∼55.8 Gy (median 54 Gy). Most
patients were treated with four-fields based on 3D-CRT.
Concomitant CTx were administered in 10 patients (58.8%) with variable CTx regimens: 4 patients received 5-FU monthly (500 mg/m2/day for 5 days), 4 patients received UFTE-G (350 mg/m2/day), 1 patient received 3 cycles of gemcitabine (1,250 mg/m2/day), and 1 patient received xeloda (1,250 mg/m2/twice daily) during RT.
4. Statistics
The primary endpoint of the study was the 2-year overall survival rate. Secondary endpoints were the 2-year disease- free survival (the patterns of locoregional and distant failu- re) rate and toxicity. By use of the Kaplan-Meier method, the overall survival (OS) and disease free survival (DFS) were calculated from the date of RT until last follow-up or death. Patients were censored from time of last follow-up or death. The univariate and multivariate prognostic factor analysis were performed using Log-rank test and cox’s proportional hazards model, respectively. The analysis of prognostic factors for OS included age, gender, ECOG performance status, T stage, pathologic stage, tumor location, tumor marker (CA 19-9), surgery type, use of CTx, and RT dose (<54 vs. ≥54 Gy).
Results
1. Toxicity
The acute gastrointestinal toxicities were RTOG grade 1 (G1) nausea in 1 patient (5.9%), G1 vomiting in 2 (11.8%), and G1∼2 enteritis in 5 (29.4%). The hematologic toxicities were G1 leukopenia in 5 patients (29.4%), G2 leukopenia 1 (5.9%), G1 thrombocytopenia in 1 (5.9%), G1 anemia 5, and G2 anemia 1 (35.3%). These acute toxicities are summarized in Table 2.
2. Overall Survival
The 1- and 2- year DFS rates were 46.3% and 30.9%, respectively. The DFS curve using the Kaplan-Meir method is shown in Fig. 1. The 1- and 2-year OS rates were 58.8%
Table 2. Acute toxicities according to RTOG/EORTC toxicity criteria
Grade 1 Grade 2 Grade 3 Grade 4
Gastrointestinal toxicities Nausea
Vomiting Enteritis
Hematologic toxicities Anemia
Leukopenia Thrombocytopenia
1/17 (5.9%) 2/17 (11.8%) 3/17 (17.6%) 5/17 (29.4%) 5/17 (29.4%) 1/17 (5.9%)
0 0 2/17 (11.8%) 1/17 (5.9%) 1/17 (5.9%)
0
0 0 0 0 0 0
0 0 0 0 0 0
Fig. 1. Overall and disease-free survival of adjuvant RT for pancreatic cancer.
Fig. 2. Univariate and multivariate analysis of survival by T-stage.
Fig. 3. Univariate and multivariate analysis of survival by postoperative CA19-9 level.
and 24.5%, respectively. The OS curve is also shown in Fig.
2. The median OS and DFS times were 12.6 (95%
confidence interval (CI), 1.1∼24.1) and 8.3 months (95%
CI, 0∼17.5) months.
3. Patterns of Failure
Of the 17 patients, locoregional failure was observed in 8 patients (47.1%). Eight patients (47.1%) had distant failure, and 5 patients (29.4%) had both locoregional and distant failure. The median time to failure was 4.9 months in locoregional disease and 3.9 months in distant failure.
Sites of distant failure were as follows: Liver 4, Lung 3, peritoneum 1, Kidney 1. Most failure (locoregional 7/8;
88%, distant 6/8; 75%) was seen in stage III patients.
4. Prognostic Factor Analysis for Survival
Using univariate analysis, T stage (
p
=0.0022), gender (p
=0.0287) and postoperative CA 19-9 level of ≥180 U/mlTable 3. Risk factors for overall survival in univariate analysis and multivariate
Factor No. of pts (%)
Any recur event/pts No.
(2y OS %)
Univariate Multivariate
Risk ratio p
Gender Male Female T stage T3 T4
Postoperative CA19-9 <180 U/ml ≥180 U/ml
13 (76.5) 4 (23.5) 11 (64.7) 6 (35.3) 13 (76.5) 4 (23.5)
8/13 (32.5) 4/4 (0) 7/11 (34.1) 5/6 (16.7) 8/13 (32.5) 4/4 (0)
0.0287
0.0022
0.0142
>0.05
0.006
0.016
12.05
5.88
For univariate analysis, log-rank test was used, and multivariate model using cox regression was used for multivariate analysis
(
p
=0.0142) were found to be significantly associated with overall survival. RT dose did not show any significant correlation with regard to OS (p
=0.1362). Variables associa- ted with OS on multivariate analysis included T stage (ha- zard ratio[HR](95% CI) 12.05 (2.02∼71.98),p
=0.006) and postoperative CA 19-9 level of ≥180 U/ml (HR (95%CI) 5.88 (1.40∼24.73),
p
=0.016). Fig. 2 and 3 shows the univariate and multivariate analysis of overall survival by T-stage and CA 19-9 level, respectively. Table 3 presents the univariate and multivariate associations.Discussion
The prognosis of patients with pancreatic cancer remains very poor. This poor prognosis is due to 2 reasons.8 The first is that most patients present at an advanced stage, with about 80% of pancreatic cancers being either metastatic or loco-regionally unresectable.9 The second is that most patients who receive surgery will not be cured by their surgery alone even though the surgery was done with curative intent. The rationale of adjuvant therapy for pancreatic cancer relies on the above-mentioned considera- tions. RT combined with 5-FU based CTx has a significant role for the adjuvant treatment for resected pancreatic cancer. The GITSG5 conducted a randomized, prospective
trial that compared adjuvant 5-FU based CCRT with no adjuvant treatment, and since then several studies have been done on the adjuvant treatment for resected pan- creatic cancer. Among them, the European Organization for Research into the Treatment of Cancer (EORTC) completed a phase III trial (EORTC Protocol 40891) that compared split courses of CCRT, which were similar to those used in the GITSG trial.10 They randomized 114 patients into the 2 treatment arms (54 in the observation arm and 60 in the CCRT arm). In the observation arm, the 2-year survival (median survival: 12.6 months) was 26% and the 2-year survival of the CCRT arm was 34% (median survival: 17.1 months) However, this survival difference was not significant (
p
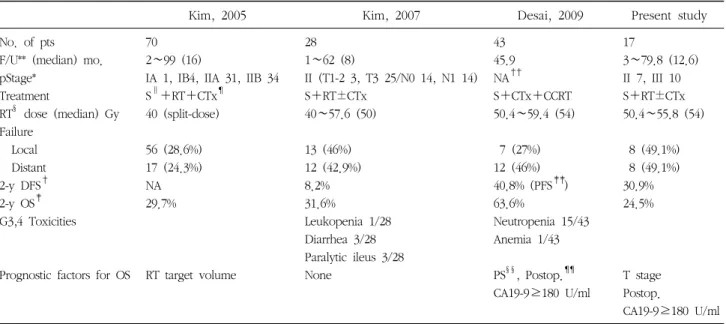
=0.099). The European Study Group for Pancreatic Cancer (ESPAC-1) trial randomized 541 pancreatic cancer patients into a two-by-two factorial design of observation and concurrent CCRT (20 Gy/10 fractions/2 weeks with 500 mg/m2 5FU IV on days 1∼3, and this was repeated after 2 weeks), CTx alone and concurrent CCRT followed by CTx. The median follow-up for the interim results was 10 months. This study showed no survival benefit for adjuvant CCRT, but it revealed a potential benefit for adjuvant CTx.11 This study was criticized for several reasons. Sixty-eight patients were assigned separately and randomized to either CCRT orTable 4. Studies evaluating adjuvant radiation therapy with or without chemotherapy in pancreatic cancer
Kim, 2005 Kim, 2007 Desai, 2009 Present study
No. of pts F/U** (median) mo.
pStage*
Treatment
RT§ dose (median) Gy Failure
Local Distant 2-y DFS† 2-y OS‡ G3,4 Toxicities
Prognostic factors for OS 70 2∼99 (16)
IA 1, IB4, IIA 31, IIB 34 S∥+RT+CTx¶
40 (split-dose)
56 (28.6%) 17 (24.3%) NA 29.7%
RT target volume
28 1∼62 (8)
II (T1-2 3, T3 25/N0 14, N1 14) S+RT±CTx
40∼57.6 (50)
13 (46%) 12 (42.9%) 8.2%
31.6%
Leukopenia 1/28 Diarrhea 3/28 Paralytic ileus 3/28 None
43 45.9 NA††
S+CTx+CCRT 50.4∼59.4 (54)
7 (27%) 12 (46%) 40.8% (PFS‡‡) 63.6%
Neutropenia 15/43 Anemia 1/43
PS§§, Postop.¶¶
CA19-9≥180 U/ml 17
3∼79.8 (12.6) II 7, III 10 S+RT±CTx 50.4∼55.8 (54)
8 (49.1%) 8 (49.1%) 30.9%
24.5%
T stage Postop.
CA19-9≥180 U/ml
*pStage=pathologic stage; †DFS=disease free survival; ‡OS=overall survival; §RT=radiation therapy; ∥S=surgery; ¶CTx=chemo- therapy; **F/U=follow up period; ††NA=not available; ‡‡PFS=progression free survival; §§PS=performance status; ¶¶Postop.=
postoperative.
observation to increase the number of patients, and 188 patients were separately assigned to either CTx alone or observation. Because the median total RT dose was only 40 Gy in that study, it was difficult to reach the conclusion that RT has a limited adjuvant role. Because of the high local failure,12 more studies13-15 have been conducted to evaluate postoperative adjuvant RT for treating resected pancreatic cancer. The results of the previous studies13-15 and the corresponding results of the present study are summarized in Table 4. Although there was no agreement on adjuvant RT for pancreatic cancer in the phase III study, the survival results and failure patterns of the present study are comparable, with acceptable toxicity, with the results of these previous studies. However, making direct com- parisons and interpretations between different studies is somewhat difficult. First, different treatment regimens were used for adjuvant therapy. We used RT as a main adjuvant therapy, whereas the majority of the studies predominantly used CCRT as adjuvant therapy or CTx as a neoadjuvant therapy. Second, the RT doses and fractionation schemes that were used slightly varied between the studies. In the
present study, the dose and fractionation scheme we used involved the delivery of 50.4∼55.8 Gy in 1.8 Gy fractions to the tumor bed using 3D-CRT, which was relatively consistent except for one study13 that used RT by a split-course technique. Third, the pathologic stages of the patients between the studies were somewhat different. In present study, 59% of the patients were pathologically staged as III, whereas most of the patients in the other studies13,14 were pathologic stage II. Fourth, all the studies were a nonrandomization, single-institution experience, with a limited number of patients and a retrospective analy- sis. We reported a median overall survival of 12.6 months and the 2-year OS was 24.5%, which are comparable13,14 to or somewhat lower15 than the results of the recent reports.
There are several possible reasons for this discrepancy between our results and the recent reports. First, the stages of the patients enrolled in the present study were more advanced than those of the recent studies.13,14 Secondly, the patients enrolled in the recent good report15 used the gemcitabine-based CCRT, which showed excellent long- term survival for patients with pancreatic cancer. The recent
RTOG 97-04 concluded that the addition of gemcitabine to adjuvant fluouracil-based CCRT was associated with a survival benefit for patients with resected pancreatic cancer, although this improvement was not statistically significant.16 Third, most of the patients in our study were not given CTx because of their poor general condition and their age (median age: 69 years), and furthermore, CTx was deli- vered with various regimens.
Our study revealed that the postoperative CA 19-9 level and the tumor size are significant prognostic factors by multivariate analysis and the postoperative CA 19-9 level was also a significant prognostic factor for OS in the other study,15 which is the first prospective, phase 3 trial that has evaluated the correlation of the postoperative CA 19-9 values with the outcome. The results of this trial will help determine whether a postoperative CA 19-9 value higher than 180 U/ml should be used as a stratification variable.
Our results suggests that complete resection is the minimal need for cure, although further studies are needed because of the retrospective nature of the currently reported studies.
In other report, the CA 19-9 level could be utilized as indicating factors of the operability of the tumor.17 They reported that the mean CA 19-9 level was higher in unresectable group (5,166.2 U/ml), compared to resectable group (964.7 U/ml) (
p
=0.039).Using 3D-CRT, we treated the patients with a relatively high RT dose for local control. Although, no relationships was apparent between the RT dose level and overall survival, there was no occurrence of unacceptable acute toxicity (RTOG grade III∼IV). Dosimetric studies have shown the benefits of IMRT (intensity modulated radiation therapy) over 3D-CRT for achieving dose escalation with the recent advances in RT planning and delivery.18 This suggests that it will be necessary to conduct a randomized trial to determine the role of a higher RT dose for local control with using advanced RT techniques.
Conclusion
Although these interim results did not show significant correlation between the higher radiation dose and local control, the survival results of the present study are comparable to those of the previous studies and the patients generally well tolerated the treatment in regard to the normal acute toxicities induced by relatively high radiation dose. The significant prognostic factors for OS of patients with pancreatic cancer were the tumor stage and the postoperative CA 19-9 level of ≥180 U/ml. We report here on our clinical experience with 17 pancreatic cancer patients who treated with RT after their surgery.
References
1. Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin 2007;57:43-66.
2. Wade TP, Halaby IA, Stapleton DR, Virgo KS, Johnson FE.
Population-based analysis of treatment of pancreatic cancer and Whipple resection: department of defense hospitals, 1989-1994. Surgery 1996;120:680-685.
3. Korea National Statistical Office. 2007 annual report on the cause of death statistics. Daejeon: The Office; 2008.
4. Calvo FA, Viere JC, Gunderson LL, Willett CG. Cancer of the pancreas. In: Chao KSC, Perez CA, Brady LW, eds. Principles and practice of radiation oncology. 4th ed. Philadelphia:
Lippincott Williams & Wilkins; 2004.1574-1588.
5. Kalser MH, Ellenberg SS. Pancreatic cancer. Adjuvant combined radiation and chemotherapy following curative resection. Arch Surg 1985;120:899-903.
6. Willett CG, Del Castillo CF, Shih HA, et al. Long-term results of intraoperative electron beam irradiation (IOERT) for pa- tients with unresectable pancreatic cancer. Ann Surg 2005;
241:295-299.
7. Greene FL, Page DL, Fleming ID, et al, eds. AJCC cancer staging manual. 6th ed. Chicago, IL: Springer; 2002.
8. Dickler A, Abrams RA. Radiochemotherapy in the manage- ment of pancreatic cancer--part II: use in adjuvant and locally unresectable settings. Semin Radiat Oncol 2005;15:235-244.
9. Sohn TA, Yeo CJ, Cameron JL, et al. Resected adenocar- cinoma of the pancreas-616 patients: results, outcomes, and prognostic indicators. J Gastrointest Surg 2000;4:567-579.
10. Klinkenbijl JH, Jeekel J, Sahmoud T, et al. Adjuvant radiotherapy and 5-fluorouracil after curative resection of
cancer of the pancreas and periampullary region: phase III trial of the EORTC gastrointestinal tract cancer cooperative group. Ann Surg 1999;230:776-782.
11. Neoptolemos JP, Dunn JA, Stocken DD, et al. European Study Group for Pancreatic Cancer. Adjuvant chemoradio- therapy and chemotherapy in resectable pancreatic cancer: a randomised controlled trial. Lancet 2001;358:1576-1585.
12. Griffin JF, Smalley SR, Jewell W, et al. Patterns of failure after curative resection of pancreatic carcinoma. Cancer 1990;66:
56-61.
13. Kim K, Kim S, Chie EK, Kim SW, Bang YJ, Ha SW. Posto- perative chemoradiotherapy of pancreatic cancer: what is the appropriate target volume of radiation therapy? Tumori 2005;91:493-497.
14. Kim SW, Chun M, Kim MW, et al. The outcome of posto- perative radiation therapy for patients with stage II pancreatic cancer (T3 or N1 disease). J Korean Soc Ther Radiol Oncol
2007;25:213-218.
15. Desai S, Ben-Josef E, Griffith KA, et al. Gemcitabine-based combination chemotherapy followed by radiation with ca- pecitabine as adjuvant therapy for resected pancreas cancer.
Int J Radiat Oncol Biol Phys 2009;75:1450-1455.
16. Regine WF, Winter KA, Abrams RA, et al. Fluorouracil vs gemcitabine chemotherapy before and after fluorouracil- based chemoradiation following resection of pancreatic adenocarcinoma: a randomized controlled trial. JAMA 2008;299:1019-1026.
17. Kil WH, Kim DK, Noh SI, et al. Adenocarcinoma of the body and tail of the pancreas;treatment and prognosis. Korean J Hepatobiliary Pancreat Surg 2000;4:161-168.
18. Brown MW, Ning H, Arora B, et al. A dosimetric analysis of dose escalation using two intensity-modulated radiation therapy techniques in locally advanced pancreatic carcinoma.
Int J Radiat Oncol Biol Phys 2006;65:274-283.