관절경적 회전근 개 봉합술 시 시행하는 골 처치
- 견봉 성형술∙원위 쇄골 절제술∙건 부착부 처치∙오구 성형술 -
서울대학교 의과대학 정형외과학교실, 분당서울대학교병원 관절센터 오주한∙박해봉∙이예현
Arthroscopic Bony Procedure During of Rotator Cuff Repair
- Acromioplasty, Distal Clavicle Resection, Footprint Preparation and Coracoplasty -
Joo Han Oh, M.D., Ph.D., Hae Bong Park, M.D., Ye Hyun Lee, M.D.
Department of Orthopaedic Surgery, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Korea
The arthroscopic bony procedures during rotator cuff repair include acromioplasty, distal clavicle resection, foot- print preparation and coracoplasty. The indication of each bony procedure is based on the theoretical reasons, and various types of surgical techniques are available. The purpose of this review article is to review the back- grounds of the indication and surgical techniques in the arthroscopic bony procedures during rotator cuff repair.
Key Words: Arthroscopic bony procedures, Rotator cuff repair, Acromioplasty, Distal clavicle resection, Foot- print preparation, Coracoplasty
Volume 16, Number 2, December, 2013 doi:http://dx.doi.org/10.5397/CiSE.2013.16.2.153
서 론
충돌 증후군(impingement syndrome) 및 회전근 개 파열(rotator cuff tear)을 비롯한 여러 견관절 질환에 대한 관절경적 수술을 시행할 때 견봉 성형술, 원위 쇄 골 절제술, 건 부착부(대결절) 처치, 오구 성형술과 같은 골 처치(bony procedure)를 시행하게 된다. 이처럼 견 관절 질환의 치료에 중요하고 필수적인 골 처치 술기에 대한 문헌들을 검토하여, 골 처치의 이론적 배경 및 적
응증, 수술적 방법에 대해 정리하고 기술하여, 이를 통 해 우수한 임상 결과와 연결시킬 수 있는지에 대하여 논 의해 보고자 한다.
본 론
1. 견봉 성형술(Acromioplasty)
1972년 Neer1)는 만성 견관절 통증의 원인 중 하나로
※통신저자: 이 예 현
경기도 성남시 분당구 구미로 166
서울대학교 의과대학 정형외과학교실, 분당서울대학교병원 관절센터 Tel: 031) 787-7197, Fax: 031) 787-4056, E-mail: segaba1@naver.com 접수일: 2013년 12월 2일, 1차 심사완료일: 2013년 12월 20일, 게재 확정일: 2013일 12월 30일
충돌 증후군을 설명하면서 처음으로 전방 견봉 성형술 을 통한 치료를 언급하였으며, 1987년 Ellman2)에 의해 관절경적 견봉 성형술이 소개되었다.
회전근 개 파열의 병태 생리는 외인적 요인과 내인적 요인이 복합적으로 작용함으로 설명할 수 있다. 외인적 요인으로는 견봉(acromion)의 모양, 견봉 골극(acro- mial spur)의 형성, 오구 견봉 인대(coracoacromial ligament)의 비후 등이 있다. 많은 연구들이3-5) 회전근 개 질환을 야기하는 Neer의 외인적 충돌 증후군 이론을 뒷받침하고 있고, 이에 따라 회전근 개 손상으로 수술 시 전방 견봉 성형술을 같이 시행해 주는 것이 좋다고 주장하고 있다. Bigliani 등4)은 갈고리 모양(hook type) 의 견봉과 전방 골극이 있는 경우 70%에서 회전근 개 전 층 파열이 있었다고 보고하였고, Ogawa 등6)은 5 mm 이상의 견봉 골극이 있는 경우 회전근 개의 점액낭측 파 열 및 전층 파열이 높은 비율로 관찰된다고 하면서 이 골극이 진단적 가치가 있다고 보고하였다. Tucker 등7) 은 용골 골극(keel spur)이 회전근 개의 점액낭측 부분 파열 및 전층 파열과 관련이 있다고 하였고, Balke 등8) 도 외측 견봉 각이 낮은 경우 및 외측으로 견봉이 튀어
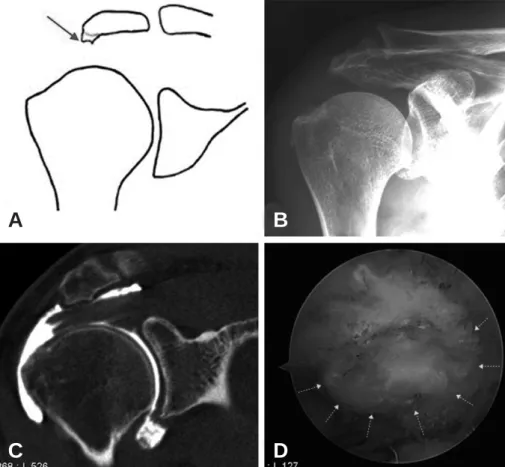
나온 경우에 충돌 증후군 및 회전근 개 파열이 많이 발 생함을 보고하였다. Oh 등9)의 연구 결과에 의하면, 회 전근 개 손상이 있는 그룹에서 견봉 골극이 더 많았으 나, 회전근 개 파열과 견봉의 형태와는 큰 차이는 없음 을 보고하였고, 평균 견봉 두께는 8 mm이었으며 회전 근 개 손상이 있는 그룹에서 더 두껍게 관찰되었고, 구 두굽 모양의 견봉 골극(heel type spur, Fig. 1)이 전층 회전근 개 파열의 위험 인자라고 보고하였다. 이렇게 여 러 논문에서 제시하듯이 견봉 골극과 회전근 개 손상은 연관성이 있음을 알 수 있으며, 이는 회전근 개 봉합술시 관절경적 견봉 성형술을 시행해야 할 근거로 볼 수 있다.
한편, 회전근 개 손상의 원인을 내재적 요인으로 주장 하는 연구자들도 있다. Ozaki 등10)은 회전근 개 손상이 퇴행성 변화로 발생한다고 주장하였고, Ogata 등11)은 회전근 개 손상이 충돌이 아닌 내재적인 퇴행성 건 병변 으로 시작된다고 보고하였다. 이렇게 내재적인 요인이 회전근 개 질환의 원인으로 생각된다면 수술적 치료 시 견봉 성형술이 정말로 필요한 시술인지 고민하지 않을 수 없고 여러 입장에서 볼 때 견봉 성형술의 시행 유무 에도 이견이 있을 수 있다.
Fig. 1. Heel type spur was shown in the (A) schematic diagram (B) plain radiograph (C) MRI and (D) arthroscopy (yellow arrow: margin of heel type spur).
A B
C D
회전근 개 질환에 있어서 견봉 성형술의 결과에 대해서 는 다양한 보고들이 있다. Odenbring 등5)이 보고한 논 문에 의하면 관절경적 견봉 성형술을 시행하고 12~14년 간 추시한 결과 77%에서 좋은 결과를 보였으며, 장기 추시 결과는 관절경적 견봉 성형술이 개방적 견봉 성형 술보다 좋았다고 보고하였다. Magaji 등12)도 수술의 적 응증만 잘 선택한다면 충돌 증후군의 경우, 관절경적 견 봉 성형술이 효과적이라고 보고하였다. 한편, MacDon- ald 등13)은 회전근 개 봉합 시 견봉 성형술 시행 유무와 기능적 결과 및 삶의 질 척도는 큰 차이가 없다고 하였 고, Shin과 Oh 등14)의 연구에서도 견봉 골극이 없는 소 형 및 중간 크기 회전근 개 파열에 대해 봉합술 시 견봉 성형술의 시행은 임상적 결과에 영향을 미치지 않는 것 으로 보고하였다. 그 외에도 일부 논문들3,13-17)에서 충돌 증후군 및 회전근 개 파열의 치료 시 견봉 성형술을 시 행한 그룹과 시행하지 않은 그룹간에는 큰 차이가 없다 고 보고하고 있다(Table 1).
따라서, 회전근 개 질환의 병인적 요인도 다양하며, 견 봉 성형술 자체에 대해서도 다양한 결과들이 보고된다는 것을 고려하면, 일률적으로 견봉 성형술을 시행하기 보다 는 환자 개개인의 상태에 따라 견봉 성형술을 할 것인지 를 결정하는 것이 더 적절한 접근 방법으로 보인다. 이에 는 견봉에 골극이 존재하는지, 골극 모양이 어떠한지(구두 굽 모양인 경우), 견봉의 두께가 충분히 두꺼운 지(MRI의
시상 영상(sagittal view)에서 견봉 쇄골 관절 후방 1 cm의 단면에서 견봉 전방의 두께가 7 mm 이상인 경우) 등을 평 가하여 견봉 성형술을 시행하는 것이 적절할 수 있겠다.
이러한 적응증을 적용했을 때, 전체 회전근 개 봉합 수술 환자의 80% 정도에서 견봉 성형술을 시행하게 된다.
수술 방법으로는 개방적 견봉 성형술 및 관절경적 견 봉 성형술이 있다. 개방적 견봉 성형술은 견봉 연마기 (acrominizer)를 견봉의 앞쪽에서 후-하방으로 삽입하여 견봉의 앞쪽의 전-하방 부분을 제거하는 Neer의 방법과,18) 쇄골보다 앞으로 튀어나온 부분을 뼈 집게(rongeur)로 제 거하고 견봉 연마기를 노출된 해면골을 통해서 후-하방 으로 진행하여 아래 부분을 제거하는 Rockwood 방법 이 있다.19) 관절경을 이용한 견봉 성형술의 원칙은 개방 적 견봉 성형술과 동일하다. Sach 등20)을 비롯한 여러
논문들21,22)에서 두 수술 방법의 임상적 결과의 차이는 없
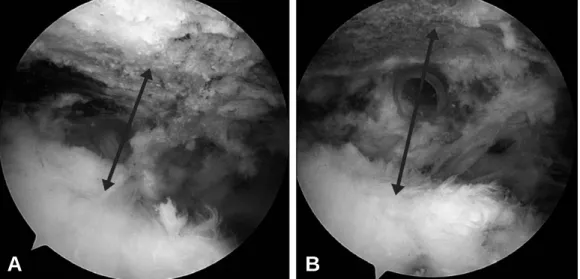
으나, 관절경적 견봉 성형술에서 빠른 회복을 보였다고 보고하였다. 저자는 우선 견봉하 공간의 상태를 관찰하 고 필요한 만큼 점액낭을 제거한 후 견봉 성형술의 적응 증이 되는 경우, 전-측방 삽입구로 견봉 연마기를 삽입 하여 견봉의 전-하방 부위를 감압을 시행한다. 필요 시 전-측방 삽입구와 후방 삽입구를 바꾸어서 전-측방에 관절경을 삽입하여 보면서 후방 삽입구를 통하여 견봉 연마기를 사용하여 견봉 아래쪽으로 돌출된 부분을 제 거하고 있다(Fig. 2).
Table 1. Studies about Acromioplasty
Study Study Design Details of Surgery Follow-Up
No difference 47 (ASRCR c AP)000
Gartsman and O’Connor, 2004, JSES16) Level III vs 15.6 mo
46 (ASRCR only)000.
Milano et 34 (ASRCR c AP)000
al., 2007, Arthroscopy15) Level III vs 24 mo
37 (ASRCR only)000.
26 (Bursectomy only).
Henkus et al., 2009, JBJS Br3) Level III vs 57 mo
30 (Bursectomy c AP) 32 (ASRCR c AP)00 0
MacDonald et al., 2011, JBJS Am13) Level III vs 12 mo
37 (ASRCR only)00.0 60 (ASRCR c AP)000
Shin SJ et al., 2012, Arthroscopy14) Level III vs 35 mo
60 (ASRCR only)000.
Prefer acromioplasty Neer CS 2nd, 1972, JBJS Am1) Level III 46 (Anterior AP)0 00.. 1 yr to 5 yr Odenbring et al., 2008, Arthroscopy5) Level III 31 (Arthroscopic AP). 12-14 yr Magaji et al., 2012, JBJS Br12) Level III 51 (Arthroscopic AP). 3 mo & 1 yr Abbreviations: AP: acromioplasty, ASRCR c AP: arthroscopic rotator cuff repair with acromioplasty, ASRCR only: arthro- scopic rotator cuff repair only
2. 원위 쇄골 절제술(Distal clavicle resection)
원위 쇄골 절제술의 적응증으로는 견봉 쇄골 관절염, 골 융해, 견봉 쇄골 불안정성 등이 있고, 시행 방법으로 는 크게 개방적 절제술 및 관절경적 절제술이 있다.
1941년 Mumford23)와 Gurd24)가 증상이 있는 견봉 쇄골 관절염 환자에서 개방적 원위 쇄골 절제술 시행 후 좋은 결과를 보고한 이후로, 관절경적 원위 쇄골 절제술 또한 좋은 결과에 대한 여러 발표들이 있었다.25-28)Robertson 등29)은 개방적 및 관절경적 원위 쇄골 절제술은 치료하 기 어려운 견봉 쇄골 관절 통증에 효과적인 치료 방법이 며, 두 방법 모두 환자의 만족도와 견관절 기능에는 좋 은 결과를 보였지만, 관절경적 수술 후 잔존하는 통증이 좀 더 적다고 보고하였다.
관절경적 절제술 방법으로는 크게 외측 견봉하(간접적) 접근법 및 상위(직접적) 접근법이 있다. 여러 연구들30-32) 에서 두 접근법에는 임상적 결과에 차이는 없으나, 직접 적 접근법에서 수술 후 회복은 빠르지만 불안정성을 야 기할 수 있는 상위 관절낭 인대 손상을 유발할 위험이 있다고 보고하였다.
Debski 등33)은 원위 쇄골 절제술과 관절경적 견봉 성 형술을 같이 시행한 경우 쇄골의 후방 이동이 의미 있게 증가함을 보고하였고, Blazar 등34)도 원위 쇄골 절제술 후 발생한 원위 쇄골의 과도한 전후방 불안정성은 수술 후 통증 및 좋지 않은 임상 결과를 가져올 수 있는 원인 이라고 하였다. 이처럼 과도한 원위 쇄골 절제술은 불안 정성을 가져올 수 있으므로, 얼마만큼 시행할 지에 대한 고민이 생기는데, Branch 등35)은 5 mm의 원위 쇄골 절 제술로도 견갑 회전 시 골 접촉을 막기에 충분하다고 보고
하였고, Edwards 등36)도 5 mm의 원위 쇄골 절제술 시행 후 골 접촉도 없고 관절 강직도 줄일 수 있다고 하였다.
원위 쇄골 절제술로 발생할 수 있는 전후방 불안정성 등의 부작용을 고려할 때, 증상은 없으나 영상의학적으 로 견봉 쇄골 관절염이 보일 경우 원위 쇄골 절제술의 시행 여부에 대한 서로 다른 주장들이 있다. Kim 등37)은 회전근 개 파열 시 증상 없는 견봉 쇄골 관절염에 대해 회전근 개 봉합 및 원위 쇄골 절제술을 시행한 결과 만 족스러운 통증 감소 및 좋은 임상 결과를 얻었고, 2년 동안 재수술은 없었다고 보고하였다. 하지만, 회전근개 파열과 동반된 견봉 쇄골 관절 병변에서 원위 쇄골 절제 술이 임상 결과에 영향을 미치지 못했다는 보고도 있으 며,38) 저자가 최근 발표한 전향적 무작위 비교 연구39)에 서도 예방적인 원위 쇄골 절제술의 시행이 견봉 쇄골 관 절의 불안정성을 초래하는 위험성이 있는 반면, 임상적 그리고 해부학적 결과는 원위 쇄골 절제술을 시행하지 않은 군과 차이를 보이지 않았기에, 무증상 견봉 쇄골 관절염에 대해서 예방적 원위 쇄골 절제술에 대하여 부 정적인 입장을 견지하였다. 하지만, 장기적인 추시 관찰 시 견봉 쇄골 관절염이 진행하여 증상을 초래할 수도 있 으므로 좀 더 장기적인 추시 관찰이 필요할 것이다.
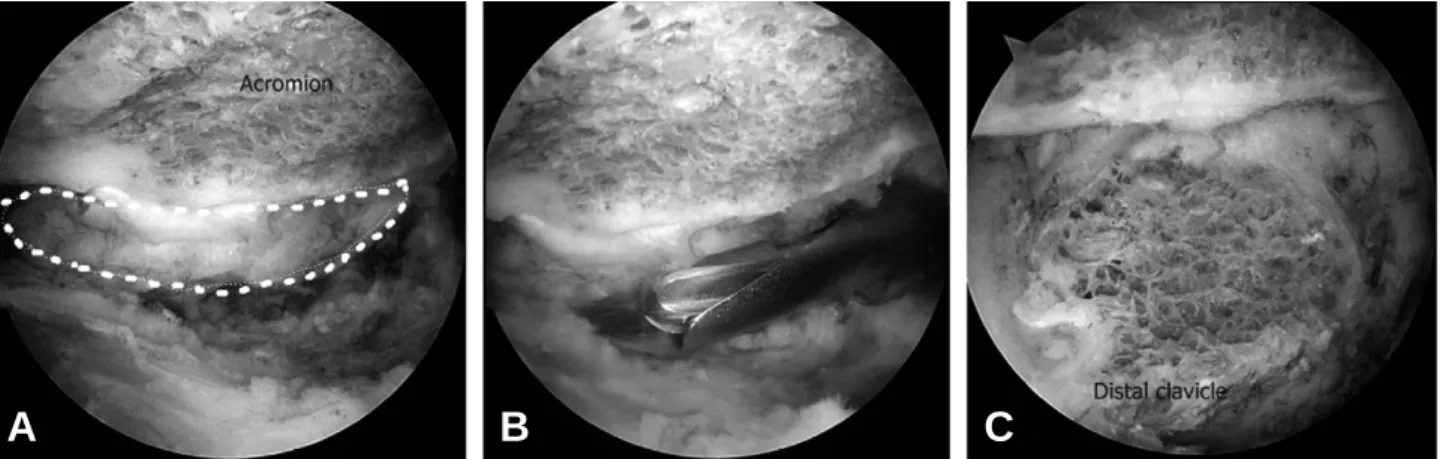
저자는 원위 쇄골 절제술은 증상이 있는, 즉 압통이나 압박 검사 양성, 내전 압박 검사 양성인 원위 쇄골 관절 염에 국한하여 시행하고 있으며, 외측 견봉하(간접적) 접근법을 통하여, 전방 삽입구를 통하여 원위 쇄골과 일 부 견봉을 절제한다(Fig. 3). 보통 연마기의 굵기 보다 조금 더 크게 절제하며, 이는 대개 7~8 mm의 두께가 된 다. 가능하면 상부 그리고 후방 견봉 쇄골 인대(posterior acromioclavicular ligament)는 손상시키지 않도록 주
Fig. 2. (A) Before the acromioplasty, subacromial spur is observed. (B) After acromioplasty, acromiohumeral distance was widen.
A B
의해야 하지만, 그렇다고 특히 후방 골 절제(posterior bone resection)가 부족하지 않도록 해야 하며, 관절 주 변의 활액막에 혈관이 풍부하므로, 시행 전에 충분한 연 부 조직 절제 및 지혈이 선행되어야 한다.
3. 대결절 건 부착부 처치
(Greater tuberosity footprint preparation)
건 부착부 처치를 시행하는 목적은 회전근 개 파열의 봉합 시 건-골간의 유합을 촉진하는데 있다. 최근 들어
회전근 개 봉합 시 생물학적 강화(biologic augmenta- tion)을 위한 여러 연구들이 진행되고 있고, 이에는 간엽 줄기 세포(mesenchymal stem cell),40)세포외 기질 이식 (extracellular matrix),41) 성장 인자(growth hormone) 유도 체계,42)건 이식(tendon transfer)43)등이 있다.
이들 중 건 부착부 처치는 회전근 개 봉합 시 건-골 유착 부분에 간엽 줄기 세포를 많이 분포시키고자 시행 하는 것으로, Ouyang 등40)은 토끼 모델을 통해 골 터널 에서 골에서 유래된 간엽 세포가 건 이식의 치유에 도움 을 줄 수 있다고 보고하였고, Mazzocca 등44)은 관절경 적 회전근 개 수술 시 사용되는 봉합 나사못(anchor) 터 널로부터 결합 조직 기원 세포(connective tissue prog- enitor cells)를 안전하고 효과적으로 채취할 수 있고, 회전근 개 봉합 시 이 세포들은 치료에 중요한 역할을 한다고 보고하였다. 또한 Kida 등45)은 회전근 개 부착 부위에 천공(drilling)을 시행하고, 이에 의해 생긴 구멍 들을 통해 골수에서 유래된 세포들이 봉합된 회전근 개로 침투하여 치유에 기여한다고 보고하였고, Jo 등46)도 회전 근 개 봉합 시 대결절에 다발성 천공(multiple channel- ing)을 시행한 것이 회복에 도움을 준다고 보고하였다 (Fig. 4). Jo 등은 2.1 mm 크기의 천공기를 사용하였으 며, 각각의 천공은 4~5 mm 간격을 이루며 10 mm의 깊이를 가진다고 하였다. 반면에, Gulotta 등47)은 간엽 줄기 세포들이 존재하고 활성화되는 근거들은 존재하 나, 구조적으로나 치유된 건 부착 부위의 강도에는 큰 개선이 없었다고 보고하였으며, Levy 등48)도 쥐 모델에 서 상완골 천공(humeral cannulation)이 건-골 치유 가 의미 있게 개선되지 않았고, 이는 천공 크기가 작아 주위 자가 골수의 충분한 이동이 제한되었기 때문이라 Fig. 3. (A) The acromioclavicular (AC) joint was identified and surrounding synoviums were resected. (B) Then, the acro- minizer (or burr) was inserted from the anterior portal to the AC joint using lateral subacromial (indirect) approach. (C) Distal clavicle resection was performed, and yellow dotted line indicated the margin of undersurface of AC joint.
A B C
Fig. 4. Multiple channeling of the footprint of rotator cuff tendon was shown. The channels are created by the bone punch of diameter 2.1 mm with 4~5 mm apart and 10 mm deep. (Courtesy by CH Jo)
고 보고하였다.
이처럼 아직까지 줄기 세포와 건과 골의 유합 촉진과 의 관계가 명확히 밝혀진 바는 없지만, 저자는 적절한 대결절 건 부착부 처치가 건-골 치유에 도움이 된다는 의견에는 동의하는 바이다. 건 부착 부위 주위에 연부 조직을 깨끗이 제거한 이후에 면도기(shaver), 연마기 (burr), 큐렛(curette)을 이용하여 피질골 박리(decor- tication)를 시행한 다음에 건이 접촉할 부분에 출혈 골 표면(bleeding bony surface)를 만드는 것은 분명히 건-골 유합을 촉진시킬 것이라 생각한다. 하지만, St.
Pierre 등49)의 연구와 같이 피질골(cortical bone)과 해 면골(cancellous bone) 사이의 건 치유에는 큰 차이가 없다고 생각하며, 나사못이 들어갈 부분은 안정성을 위 해 피질골 박리를 최소화하여 시행한다. 회전근 개 수술 환자의 대부분이 고령의 환자이고, 전신적인 골다공증 이 없더라도 회전근 개 부착부의 스트레스 유발 국소 골 다공증(stress-deprived local osteoporosis)이 존재 함을 고려한다면, 지나친 건 부착부 처치나 미세 골절 (micro-fracture)과 같은 수기는 회전근 개 봉합에 필 수적으로 사용되는 봉합 나사못의 기계적 뽑힘 강도 (mechanical pull out strength)를 약화시킬 수 있음 을 주지해야 할 것이다.
4. 오구 성형술(Coracoplasty)
1985년 Gerber 등50)이 만성 충돌 증후군에서 오구 돌 기(coracoid process)의 역할에 대해 처음 기술한 이 후, 견갑하건(subscapularis) 파열의 유병률 증가로 이 와 관련된 임상적 술기의 연구가 최근 많아지고 있다.
Lo 등51)은 오구 돌기하 충돌(subcoracoid impinge- ment)은 지속적 증상을 남기고 봉합된 견갑하건을 약화
시키며, 견갑하건 파열이 있는 환자에서 오구 상완 간격 (coracohumeral distance, CHD)이 의미 있게 감소하 고 있음(파열이 있는 환자에서 5±1.7 mm로, 파열 없 는 환자군 10±1.3 mm 보다 좁아져 있음)을 보고한 바 있다. Lo 등51)과 Richard 등52)은 오구 돌기하 충돌을 오 구 상완 간격이 6 mm 이하인 경우로 정의하고, 이와 견 갑하건 파열이 연관성이 있음을 보고하였다. 그 외에도 여러 저자들53,54)이 CT와 MRI를 이용하여 오구 상완 간 격을 측정하여 견갑하건 파열이 있는 환자에서 그 간격 이 좁아져 있으며, 증상 있는 환자 군에서 오구 상완 간 격의 의미 있는 감소가 있다고 보고하였다. 하지만, Radas 등55)은 사체 실험에서 오구 상완 간격과 견갑하건 의 파열과는 연관성이 없다고 보고하였고, Bergin 등56) 도 측정된 오구 상완 간격과 견갑하건 파열의 정도와는 의미 있는 연관성이 없다고 보고하였다.
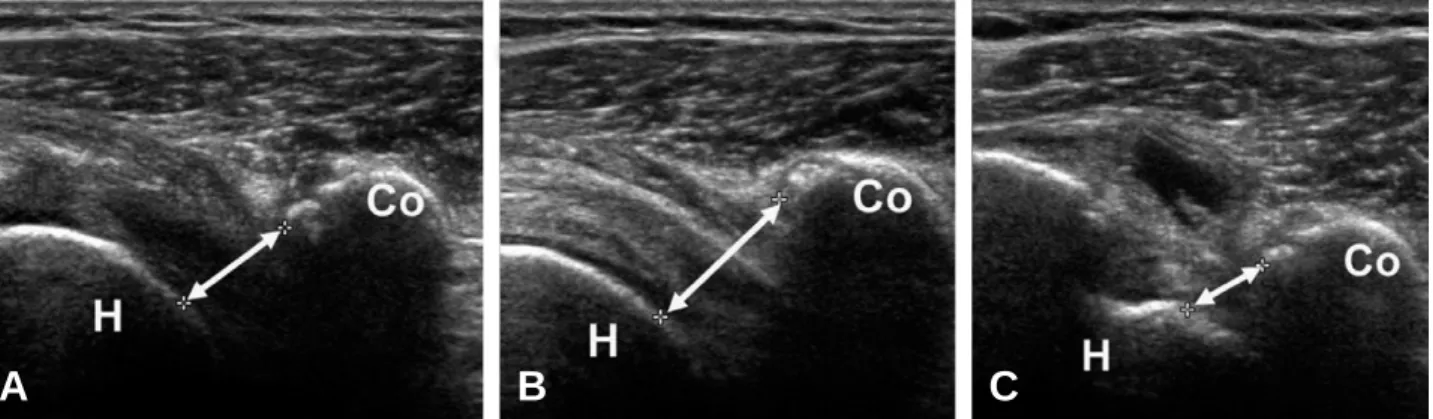
이처럼 서로 반대되는 결과를 보고 하는 것에 대해 MacMahon 등57)은 어깨 회전 시 오구 상완 간격이 변화 하기 때문이라고 하면서, 정적(static)인 CT 및 MRI 검 사를 통해 병적 상태를 진단하는데 제한이 있음을 보고 한 바 있다. 이에 대해 저자는 역동성 초음파(dynamic ultrasonography)를 이용하여 오구 상완 간격을 정확 히 측정하고 이와 견갑하건 파열의 관계를 알아보는 연 구를 시행하였다.58) 역동성 초음파로 중립적 자세와 외 회전, 내회전하여 오구 상완 간격을 측정하여(Fig. 5) 견갑하건 파열과의 연관성을 조사한 저자들의 연구에서 는 견관절의 내회전 시 다른 자세보다 오구 상완 간격이 유의하게 감소되었으며, 전체적으로 오구 상완 간격과 견갑하건 파열이 유의하게 연관되어 있지는 않았으나, 6 mm 이내의 역동성 오구돌기하 협착이 있는 경우에는 견갑하건의 파열이 의미 있게 증가되어 있었다. 이에 따 라 오구 성형술을 역동성 오구돌기하 협착이 있는 경우
Fig. 5. The dynamic coracohumeral distances (CHD) were measured using ultrasonography with the arm in neutral rotation (A), in full external rotation (B) and in full internal rotation (C). (Co: coracoid process, H: humerus, arrow, CHD)
A B C
역동성 초음파에서 내회전 시 CHD가 6 mm 이내인 경우 에만 국한하여 시행하며, 오구 견봉 인대(coracoacro- mial ligament)를 따라 고주파(radiofrequency)를 이용 하여 오구돌기의 후외방 부위를 박리한 후, 견갑하건 방 향과 평행하게 성형술을 시행한다(Fig. 6).
결 론
아직까지 관절경을 이용한 회전근 개 질환 수술 시 흔 히 수행되는 관절경적 골 처치에 대한 명확한 합의 (consensus)는 성립되지 않았다고 할 수 있다. 각 술자 들은 이론적 근거를 통한, 그리고 임상적 경험을 통한 각 시술의 적응증을 설정하고, 적절한 수술적 방법을 개 발할 필요가 있겠다. 추후 많은 임상 연구들을 통하여 각각의 술기에 대한 이론적 정립이 필요하며, 이를 통하 여 더 나은 임상적인 결과를 얻을 수 있도록 노력해야 할 것이다.
REFERENCES
01) Neer CS, 2nd. Anterior acromioplasty for the chron- ic impingement syndrome in the shoulder: A prelimi- nary report. J Bone Joint Surg Am. 1972;54:41-50.
02) Ellman H. Arthroscopic subacromial decompression:
Analysis of one- to three-year results. Arthroscopy.
1987;3:173-81.
03) Henkus HE, de Witte PB, Nelissen RG, Brand R, van Arkel ER. Bursectomy compared with acromio- plasty in the management of subacromial impinge-
ment syndrome: A prospective randomised study. J Bone Joint Surg Br. 2009;91:504-10.
04) Bigliani LU, Ticker JB, Flatow EL, Soslowsky LJ, Mow VC. The relationship of acromial architecture to rotator cuff disease. Clin Sports Med. 1991;
10:823-38.
05) Odenbring S, Wagner P, Atroshi I. Long-term out- comes of arthroscopic acromioplasty for chronic shoulder impingement syndrome: A prospective cohort study with a minimum of 12 years’ follow-up.
Arthroscopy. 2008;24:1092-8.
06) Ogawa K, Yoshida A, Inokuchi W, Naniwa T.
Acromial spur: Relationship to aging and morpho- logic changes in the rotator cuff. J Shoulder Elbow Surg. 2005;14:591-8.
07) Tucker TJ, Snyder SJ. The keeled acromion: An aggressive acromial variant--a series of 20 patients with associated rotator cuff tears. Arthroscopy.
2004;20:744-53.
08) Balke M, Schmidt C, Dedy N, Banerjee M, Bouil- lon B, Liem D. Correlation of acromial morphology with impingement syndrome and rotator cuff tears.
Acta Orthop. 2013;84:178-83.
09) Oh JH, Kim JY, Lee HK, Choi JA. Classification and clinical significance of acromial spur in rotator cuff tear: Heel-type spur and rotator cuff tear. Clin Orthop Relat Res. 2010;468:1542-50.
10) Ozaki J, Fujimoto S, Nakagawa Y, Masuhara K, Tamai S. Tears of the rotator cuff of the shoulder associated with pathological changes in the acromion. A study in cadavera. J Bone Joint Surg Am. 1988;70:1224-30.
11) Ogata S, Uhthoff HK. Acromial enthesopathy and Fig. 6. (A) The coracohumeral distance (CHD) was shown with the arrow before coracoplasty. (B) After coracoplasty, CHD was widened. (LT: lesser tuberosity, yellow line: outlining of coracoid base, yellow dotted line: coracohumeral distance)
A B
rotator cuff tear. A radiologic and histologic post- mortem investigation of the coracoacromial arch.
Clin Orthop Relat Res. 1990:39-48.
12) Magaji SA, Singh HP, Pandey RK. Arthroscopic subacromial decompression is effective in selected patients with shoulder impingement syndrome. J Bone Joint Surg Br. 2012;94:1086-9.
13) MacDonald P, McRae S, Leiter J, Mascarenhas R, Lapner P. Arthroscopic rotator cuff repair with and without acromioplasty in the treatment of full-thick- ness rotator cuff tears: A multicenter, randomized con- trolled trial. J Bone Joint Surg Am. 2011;93:1953-60.
14) Shin SJ, Oh JH, Chung SW, Song MH. The effica- cy of acromioplasty in the arthroscopic repair of small- to medium-sized rotator cuff tears without acromial spur: Prospective comparative study.
Arthroscopy. 2012;28:628-35.
15) Milano G, Grasso A, Salvatore M, Zarelli D, Deriu L, Fabbriciani C. Arthroscopic rotator cuff repair with and without subacromial decompression:
A prospective randomized study. Arthroscopy. 2007;
23:81-8.
16) Gartsman GM, O’Connor D P. Arthroscopic rota- tor cuff repair with and without arthroscopic sub- acromial decompression: A prospective, randomized study of one-year outcomes. J Shoulder Elbow Surg.
2004;13:424-6.
17) Lee KW, Kim KH, Lee HH, Kim BS, Kim HY, Choy WS. Arthroscopically assisted repair of large to massive rotator cuff tears - the role of acromio- plasty-. J. of Korean Shoulder and Elbow Society.
2003;6:143-48.
18) Neer CS, 2nd. Anterior acromioplasty for the chron- ic impingement syndrome in the shoulder. 1972. J Bone Joint Surg Am. 2005;87:1399.
19) Rockwood CA, Lyons FR. Shoulder impingement syndrome: Diagnosis, radiographic evaluation, and treatment with a modified neer acromioplasty. J Bone Joint Surg Am. 1993;75:409-24.
20) Sachs RA, Stone ML, Devine S. Open vs. Arthro- scopic acromioplasty: A prospective, randomized study. Arthroscopy. 1994;10:248-54.
21) Van Holsbeeck E, DeRycke J, Declercq G, Martens M, Verstreken J, Fabry G. Subacromial impingement: Open versus arthroscopic decompres- sion. Arthroscopy. 1992;8:173-8.
22) Lindh M, Norlin R. Arthroscopic subacromial decompression versus open acromioplasty. A two-year follow-up study. Clin Orthop Relat Res. 1993:174-6.
23) Mumford E. Acromioclavicular dislocation a new operative treatment. The Journal of Bone & Joint
Surgery. 1941;23:799-802.
24) Gurd FB. The treatment of complete dislocation of the outer end of the clavicle: An hitherto undescribed operation. Ann Surg. 1941;113:1094-8.
25) Bigliani LU, Nicholson GP, Flatow EL. Arthro- scopic resection of the distal clavicle. Orthop Clin North Am. 1993;24:133-41.
26) Flatow EL, Duralde XA, Nicholson GP, Pollock RG, Bigliani LU. Arthroscopic resection of the dis- tal clavicle with a superior approach. J Shoulder Elbow Surg. 1995;4:41-50.
27) Henry MH, Liu SH, Loffredo AJ. Arthroscopic management of the acromioclavicular joint disorder.
A review. Clin Orthop Relat Res. 1995:276-83.
28) Snyder SJ, Banas MP, Karzel RP. The arthroscop- ic mumford procedure: An analysis of results.
Arthroscopy. 1995;11:157-64.
29) Robertson WJ, Griffith MH, Carroll K, O’Donnell T, Gill TJ. Arthroscopic versus open distal clavicle excision: A comparative assessment at intermediate- term follow-up. Am J Sports Med. 2011;39:2415-20.
30) Miller CA, Ong BC, Jazrawi LM, et al. Assessment of clavicular translation after arthroscopic mumford procedure: Direct versus indirect resection--a cadav- eric study. Arthroscopy. 2005;21:64-8.
31) Levine WN, Soong M, Ahmad CS, Blaine TA, Bigliani LU. Arthroscopic distal clavicle resection:
A comparison of bursal and direct approaches.
Arthroscopy. 2006;22:516-20.
32) Charron KM, Schepsis AA, Voloshin I. Arthro- scopic distal clavicle resection in athletes: A prospective comparison of the direct and indirect approach. Am J Sports Med. 2007;35:53-8.
33) Debski RE, Fenwick JA, Vangura A, Jr., Fu FH, Woo SL, Rodosky MW. Effect of arthroscopic pro- cedures on the acromioclavicular joint. Clin Orthop Relat Res. 2003:89-96.
34) Blazar PE, Iannotti JP, Williams GR. Anteroposte- rior instability of the distal clavicle after distal clav- icle resection. Clin Orthop Relat Res. 1998:114-20.
35) Branch TP, Burdette HL, Shahriari AS, Carter FM, 2nd, Hutton WC. The role of the acromioclav- icular ligaments and the effect of distal clavicle resection. Am J Sports Med. 1996;24:293-7.
36) Edwards SL, Wilson NA, Flores SE, Koh JL, Zhang LQ. Arthroscopic distal clavicle resection: A biomechanical analysis of resection length and joint compliance in a cadaveric model. Arthroscopy.
2007;23:1278-84.
37) Kim J, Chung J, Ok H. Asymptomatic acromioclav- icular joint arthritis in arthroscopic rotator cuff ten-
don repair: A prospective randomized comparison study. Arch Orthop Trauma Surg. 2011;131:363-9.
38) Yoo MJ, Seo JB, Lee DH, Kim SJ. Clinical results after repair of rotator cuff tear in patients with accompanying ac joint pathology: Clinical compari- son of non-operative treatment. J. of Korean Shoul- der and Elbow Society. 2012;15:86-90.
39) Oh JH, Choi JH, Kim JY. Is a distal clavicle resec- tion necessary in patients with radiologic acromioclav- icular joint arthritis with rotator cuff tear?: A prospec- tive randomized comparative study. Paper presented at: The 57th Spring Congress of the Korean Orthopaedic Association. 2013 Apr 19; Daegu, South KOREA.
40) Ouyang HW, Goh JC, Lee EH. Use of bone mar- row stromal cells for tendon graft-to-bone healing:
Histological and immunohistochemical studies in a rabbit model. Am J Sports Med. 2004;32:321-7.
41) Derwin KA, Badylak SF, Steinmann SP, Iannotti JP. Extracellular matrix scaffold devices for rotator cuff repair. J Shoulder Elbow Surg. 2010;19:467-76.
42) Rodeo SA, Potter HG, Kawamura S, Turner AS, Kim HJ, Atkinson BL. Biologic augmentation of rotator cuff tendon-healing with use of a mixture of osteoinductive growth factors. J Bone Joint Surg Am.
2007;89: 2485-97.
43) Warner J. Management of massive irreparable rota- tor cuff tears: The role of tendon transfer. Instruc- tional course lectures. 2001;50:63.
44) Mazzocca AD, McCarthy MB, Chowaniec DM, Cote MP, Arciero RA, Drissi H. Rapid isolation of human stem cells (connective tissue progenitor cells) from the proximal humerus during arthroscopic rota- tor cuff surgery. Am J Sports Med. 2010;38:1438-47.
45) Kida Y, Morihara T, Matsuda K, et al. Bone mar- row-derived cells from the footprint infiltrate into the repaired rotator cuff. J Shoulder Elbow Surg. 2013;
22:197-205.
46) Jo CH, Yoon KS, Lee JH, et al. The effect of multi- ple channeling on the structural integrity of repaired rotator cuff. Knee Surg Sports Traumatol Arthrosc.
2011;19:2098-107.
47) Gulotta LV, Kovacevic D, Ehteshami JR, Dagher E, Packer JD, Rodeo SA. Application of bone mar- row-derived mesenchymal stem cells in a rotator cuff
repair model. Am J Sports Med. 2009;37:2126-33.
48) Levy DM, Saifi C, Perri JL, Zhang R, Gardner TR, Ahmad CS. Rotator cuff repair augmentation with local autogenous bone marrow via humeral can- nulation in a rat model. J Shoulder Elbow Surg. 2013.
49) St Pierre P, Olson EJ, Elliott JJ, O’Hair KC, McKinney LA, Ryan J. Tendon-healing to cortical bone compared with healing to a cancellous trough.
A biomechanical and histological evaluation in goats. J Bone Joint Surg Am. 1995;77:1858-66.
50) Gerber C, Terrier F, Ganz R. The role of the cora- coid process in the chronic impingement syndrome. J Bone Joint Surg Br. 1985;67:703-8.
51) Lo IK, Parten PM, Burkhart SS. Combined subco- racoid and subacromial impingement in association with anterosuperior rotator cuff tears: An arthro- scopic approach. Arthroscopy. 2003;19:1068-78.
52) Richards DP, Burkhart SS, Campbell SE. Relation between narrowed coracohumeral distance and sub- scapularis tears. Arthroscopy. 2005;21:1223-8.
53) Friedman RJ, Bonutti PM, Genez B. Cine magnet- ic resonance imaging of the subcoracoid region.
Orthopedics. 1998;21:545-8.
54) Kleist KD, Freehill MQ, Hamilton L, Buss DD, Fritts H. Computed tomography analysis of the cora- coid process and anatomic structures of the shoulder after arthroscopic coracoid decompression: A cadav- eric study. J Shoulder Elbow Surg. 2007;16:245-50.
55) Radas CB, Pieper HG. The coracoid impingement of the subscapularis tendon: A cadaver study. J Shoulder Elbow Surg. 2004;13:154-9.
56) Bergin D, Parker L, Zoga A, Morrison W. Abnor- malities on MRI of the subscapularis tendon in the presence of a full-thickness supraspinatus tendon tear. AJR Am J Roentgenol. 2006;186:454-9.
57) MacMahon PJ, Taylor DH, Duke D, Brennan DD, O’Brien J, Eustace SJ. Contribution of full-thick- ness supraspinatus tendon tears to acquired subcora- coid impingement. Clin Radiol. 2007;62:556-63.
58) Oh JH, Chung SW, Kim SH, Kim DH, Song BW.
Subscapularis tear: Result of subcoracoid stenosis?:
Measurement of coracohumeral distance using dynam- ic ultrasonography and its correlation with subscapu- laris tear. Poster session presented at: 2013 AAOS annual meeting, 2013 Mar 19; Chicago, IL.
초 록
관절경적 회전근 개 복원술 시에 시행하게 되는 골 처치에는 견봉 성형술, 원위 쇄골 절제술, 건 부착부(대결 절 부위) 처치 및 오구 성형술 등이 있다. 각각의 골 처치는 여러 이론적 근거에 의해 적응증을 가지며, 수술 방법 또한 다양하게 알려져 있다. 이에 관절경적 회전근 개 복원술 시에 사용되는 여러 골 처치의 적응증 및 방법에 대해 기술하고자 하였다.
색인 단어: 관절경적 회전근 개 복원술, 견봉 성형술, 원위 쇄골 절제술, 건 부착부 처치, 오구 성형술