Paint gun is used for painting ships or automobiles. It ejects paint through a nozzle at pressures as high as 1,500-3,000 lb/
inch2. When highly pressured paint invades a worker’s skin, even though the entry point is small, the paint spreads along muscle fascia, tendon sheaths, and sometimes along neurovascular bun- dles. This invasion subsequently causes an acute inflammatory reaction. At first the patient does not feel any recognizable symp- toms, however after several hours severe swelling and pain devel- op. If treatment is delayed or if the paint has spread along the neurovascular bundle of the finger, necrosis of the injured finger develops. The authors analysed the results of treatment in 30 cases of paint gun injury.
MATERIALS AND METHODS
From March 1990 to September 2000, 30 patients were treat- ed for paint gun injury of the hand. All 30 patients were male with a mean age of 36 years (ranging from 23 to 52 years). Ten patients were injured while cleaning the blocked nozzle, 5 patients were injured by an explosion of the line connecting the compres- sor and the paint gun, and 15 patients were injured by a careless co-worker. Four patients were injured in the thumb, 14 patients in the index finger, 2 patients in the middle finger, 6 patients in the ring finger and 4 patients in the metacarpal area. Twenty-four
patients were treated within one day of injury, 3 patients were treated between one and two days, one patient was treated between three to five days, and two patients were treated between five to seven days. When the injury was confined within the finger it was defined as a localized injury (Fig. 1), and when multiple metacarpal bones were invaded, it was defined as an extensive injury (Fig. 2). There were 26 cases of localized injury and 4 cases of extensive injury. We treated the patients on an emergency basis.
We extended the original wound and removed the paint as much as possible, left the wound open without any closure and repeat- ed the debridement to remove the newly developed necrotic tis- sue or the remaining paint even several days. When we were able to confirm that the necrosis was not progressing, we closed the wound. If there was a need for flap surgery, we performed the pro- cedure according to the situation (Fig. 4). Clinical outcomes were evaluated using the Strickland6)evaluation method (Table 1).
Follow-up ranged from 1 year 7 months to 12 years 7months, averaging 4 years 8 months. Outcomes were analysed according to the extent of injury, the time between injury and surgery, and the cause of amputation.
RESULTS
When a result was graded as excellent or good by the Strick- land evaluation method, it was considered to be satisfactory, and when it was graded as fair or poor it was considered unsatisfac- tory. Results in 19 patients (63%) were satisfactory and in 11 patients unsatisfactory. Nineteen among 26 patients who sustained localized paint gun injury had satisfactory results, and all four
514 514 514 514 Address reprint requests to
Sogu Lew, M.D.
Department of Orthopedic Surgery, Ulsan University Hospital 290-3 Chunha-dong, Dong-gu, Ulsan 682-714, Korea Tel: +82.52-250-7129, Fax: +82.52-235-2823 E-mail: sogulew@hanmail.net
Purpose:To evaluate the serious effects of a paint gun injury and to determine the proper treatment.
Materials and Methods:The authors reviewed 30 cases of paint gun injuries of the hand that were treated from March, 1990 to Septem- ber, 2000. We extended the original wound and removed the paint as soon as possible. The wound was left open, and debridement repeated and delayed wound closure performed. The authors evaluated the results according to the Strickland evaluation method, and anal- ysed the results with respect to treatment delay and extent of injury.
Results: Delayed treatment, invasion of the paint along the neurovascular bundle and extensive injury resulted in a poor outcome. Ampu- tation was inevitable in 4 cases in which treatment had been delayed or when blood vessels had been invaded by the paint.
Conclusion:Paint gun injury should be considered an emergency requiring immediate debridement. The surgeon should warn the patient that even after proper treatment, poor outcome can result.
Key Words: Hand, Paint Gun Injury
Bum-Soo Kim, M.D., Sang Hun Ko, M.D., Sung-Do Cho, M.D., Sogu Lew, M.D., Ju-Yong Lee, M.D., Moon Soo Park, M.D.
Department of Orthopedic Surgery, Ulsan University Hospital, Ulsan, Korea
patients who sustained extensive paint gun injury had unsatis- factory results. Results according to the time between injury and
surgery are summarized in Table 2. Two patients who had under- gone surgery more than 5 days after injury experienced an unsat-
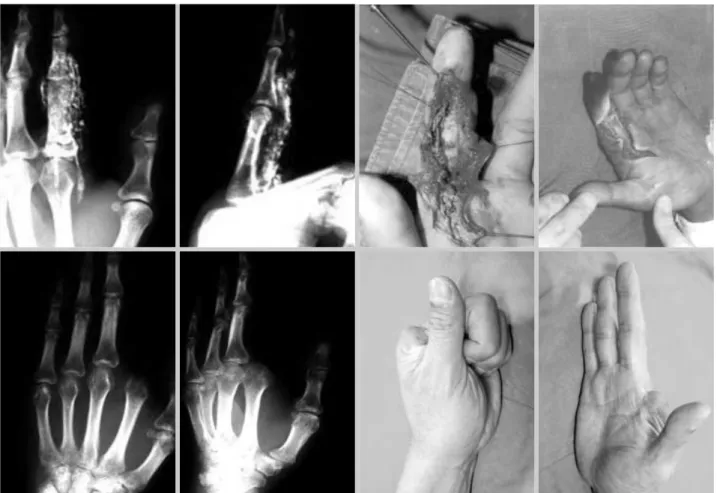
Fig. 2. Fourty-five-year old man injured by a paint gun in the left hand. Paint invaded the hand extensively. It was removed immediately but after the treatment the hand function was poor.
Fig. 1. Radiograph of a 45 year old man whose right 4th finger was injured by a paint gun. The paint was removed immediately.
isfactory outcome; one patient underwent amputation of the in- jured digit. Amputation was performed in 4 patients, two of which were treated two and five days after the injury, respectively, the other two patients received amputation due to paint invasion along the neurovascular bundle (Fig. 3).
DISCUSSION
High pressure injection injury of the hand occurs in certain industries such as in shipyards. Most doctors are unfamiliar with this kind of injury. Therefore doctors tend not to realize the seri- ousness of the injury and patients treatment, and the complica-
Fig. 3. Fourty-seven year old man injured by a paint gun. Paint invaded along the neurovascular bundle of the finger. Amputation was inevitable due to necrosis of the digit.
Fig. 4. Thirty-six year old man injured by a paint gun. Paint invaded the distal phalanx of the left index finger. After removal of the paint, necrosis developed, and a cross finger flap was performed.
tion may be amplified. Paint gun injuries mainly involve the hand.
When workers are injured by a paint gun, they often do not com- plain of specific symptoms except minor discomfort. The injury appears as a tiny laceration of the hand, which is the entry point of the paint. Doctors without experience of paint gun injuries, treat the patient symptomatically, and concentrate only on the laceration. However, paint that has invaded the skin at high pres- sure travels along muscle fascia, tendon sheaths and sometimes along neurovascular bundles. A few hours after the injury, acute inflammatory reaction occurs and swelling and pain develop. If proper treatment is delayed, necrosis of the injured digit can occur.
According to previous reports, the amputation rate due to paint gun injury ranges from 16%4)to 48%5). Kaufman1)recommend- ed that because the prevalence of amputation after high pressure injury is so high, that the primary treatment should be amputa- tion. Lewis2)reported that the factors affecting treatment results are; the amount of paint invasion, the existence of infection, and the time between injury and operation. In this study, all patients who suffered from an extensive paint gun injury had unsatisfac- tory outcomes, and delayed treatment showed a tendency to be associated with poor outcome. However, when the amount of paint invasion was small, we were able to obtain a good outcome even if the treatment was delayed. We amputated the affected digit in 4 patients, a 13% amputation rate. Two of these patients came late to the hospital, 2 and 5 days after the injury, respectively. The other two came to the hospital immediately after injury, but paint had invaded along the neurovascular bundle and this led to necro- sis of the digit.
Pinto et al.3)explained the injury mechanism as a compartment syndrome due an acute inflammatory reaction and the localized toxic effect of the paint. Vente and Bolhuis7)reported that if a
foreign material invades a restricted space, it compresses the neu- rovascular bundle causing thrombosis of the digits. They also sug- gested that sometimes the paint directly destroys blood vessel walls.
Our patients had no initial complaint except for the small entry.
After a few hours they complained of swelling, pallor and paras- thesia of the digits. The authors believe that necrosis of a digit can be due either to compartment syndrome, which causes swelling, or directly due to vessel injury caused by paint invasion along the neurovsacular bundle.
Pinto et al.3)advocated that the proper treatment of paint gun injury should be extensive debridement and drainage. The wound should be left open and observed carefully with repeated debride- ment and delayed wound closure. They treated 25 cases of paint gun injury using this method, and achieved an 84% survival rate of the digit and normal digit function in 64% of cases. This is an excellent result compared to those reported by others. The authors of this paper treated patients using the same methods and achieved an amputation rate of 13% with satisfactory hand function in 63% of cases. Our experience indicates that the initial wound should be opened widely, this minimizing the possibility of com- partment syndrome due to swelling. The paint should be removed thoroughly and the wound left open, the process of necrosis should then be carefully observed. The wound should be debrided repeat- edly. When the wound becomes stable it should be closed. How- ever this treatment will not yield uniformly satisfactory results, because of the penetration of an enormous amount of paint and its movement along the neurovascular bundles, the results are very poor regardless of treatment. In consequence, patients should be warned about the possibility of poor outcomes from paint gun injuries, even after proper treatment.
CONCLUSION
Paint gun injuries should be considered emergency cases, and require the prompt removal of paint and debridement of the wound. The wound should be left open for days under careful observation and repeatedly debrided. The wound should be closed after the necrotic process stops. It is important to warn the patient that even with proper treatment, results are not uniformly sat- isfactory due to the severe inflammatory reaction caused by the paint.
REFERENCES
1. Kaufman HD: The clinicopathological correlation of high pressure injec- tion injuries. Br J Surg, 55: 214-218, 1968.
2. Lewis RC Jr: High-compression injection injuries to hand. Emerg Med Clin North Am, 3: 373-381, 1985.
Active (PIP+DIP) flexion-Extension lag 175°
% of normal active DIP and PIP motion
×100
85-100% (greater than 150°) : Excellent
70- 84% (125-149°) : Good
50- 69% (90-124°) : Fair
Less than 50% (less than 90°) : Poor Table 1.Outcome Analysis using the Strickland Method
Time between
Injury and Operation (day) 0-1 1-2 3-5 5-7
Satisfactory Result (cases) 17 1 1 0 Unsatisfactory Result (cases) 7 2 0 2 Table 2.Treatment results according to the time between injury and surgery
130, 1993.
4. Ramos HR, Posch JL and Lie KK: High-pressure injection injuries of the hand. Plast Reconstr Surg, 45: 221-226, 1970.
5. Schoo MJ, Scott FA and Boswick JA Jr: High pressure injuries of the
don repair in zone II: A comparison of immobilization and controlled passive techniques. J Hand Surg, 5: 537-543, 1980.
7. Vente JP and Bolhuis RJ: Airless paint gun injuries of the hand: a report of three cases. Injury, 16: 91-93, 1984.
목 적 :페인트 총 손상의 심각성과 적절한 치료방법에 대해 알아보고자 하였다.
대상 및 방법 : 1988년 3월부터 2000년 9월까지 페인트 총 손상으로 치료받은 30예를 대상으로 하였다. 저자들은 환자가 내원하면 가능한 신 속히 피부를 확장 절개하여 페인트를 제거하였고 상처를 개방시켜 추가적인 페인트제거 및 세척을 시행한 뒤 지연 봉합하여 치료하였다.
Strickland의 결과 평가법에 따라 결과를 평가하였는데 수상후 페인트제거까지의 소요시간 및 손상범위에 따라 환자를 구분하여 치료결과에 미치는 영향을 분석하였다.
결 과 : 수상후 수일이 경과된 뒤 제거수술을 받거나 혈관초를 타고 페인트가 퍼진 경우 그리고 광범위하게 페인트가 침투한 경우 그 결과는 불
량하였다. 4예에서 수지 절단을 시행하였는데 이는 수상후 내원시까지 시간이 지연된 경우와 수상시 혈관 손상이 심한 경우였다.
결 론 :페인트 총 손상은 응급치료를 요하는 손상으로 분류되어야 하며 그 치료는 신속한 페인트의 제거 및 변연절제술이며 수술상처는 수일간
개방시킨 상태로 지켜보다가 지연봉합을 하는 것이 권장된다. 또한 환자에게는 적절한 치료를 시행함에도 불구하고 침투한 페인트의 염증유발작 용으로 인해 그 결과가 좋지 않을 수 있음에 대하여 충분한 경고를 하여야 할것으로 판단된다.
색인 단어 : 수부, 페인트총 손상
수부 고압 주입 손상의 치료
김범수∙고상훈∙조성도∙류석우∙이주용∙박문수
울산대학교 병원 정형외과