J Korean Soc Surg Hand 2011;16(3):134-141.
THE HAND
서론
전위된 원위 요골의 불안정한 골절에서 해부학적 정복과 단 단한 고정은 치료의 원칙으로 알려져 있다1. 정복 및 금속 강 선 고정술과 필요에 따라 외고정기를 이용하는 방법은 불안정 원위 요골 골절의 수술적 치료의 한 방법으로 오래 전부터 가 장 흔히 사용되었다2-7. 최근에는 관혈적 정복 및 내고정술이 다시 각광을 받고 있으며, 특히 수장부에 사용하는 잠김 압박 금속판의 등장 이후 가속화 되었다8. 관혈적 내고정술이 선호 되는 이유는 수술 후 손목 관절의 조기 재활 운동이 가능하므
로 기능적으로 빠른 회복을 가져올 수 있다는 점이다9-11. 본 연 구에서는 AO C1, 2형 원위 요골 골절에서 도수 정복 및 K-강 선 고정술을 시행한 군과 수장부에 잠김 압박 금속판 내고정 술을 이용하여 치료한 군의 임상적 그리고 방사선학적 결과를 비교하고자 하였다.
대상 및 방법
11.. 연연구구 대대상상 및및 방방법법
2006년 03월부터 2010년 01월까지 본원에서 AO C1, 2형
경피적 핀 또는 전방 잠김 금속판으로 치료한 AO C1, 2형 원위 요골 골절의 임상 및 방사선학적 결과
Clinical and Radiologic Outcomes of AO Type C1, 2 Distal Radius Fractures Treated with Percutaneous Pinning or Volar Locking Plating
현윤석∙송경원∙박현진∙박현태
한림대학교 의과대학 강동성심병원 정형외과
접수일2011년 2월 28일 수정일2011년 8월 22일 게재확정일2011년 8월 24일 교신저자송경원
서울시 강동구 길동 445
한림대학교 강동성심병원 정형외과 TEL02-2224-2230 FAX02-489-4391 [email protected]
* 본 논문의 요지는 대한정형외과학회 2010년 추계학 술대회에서 발표되었음.
목적:AO C1, 2형 원위 요골 골절의 수술적 치료에서 도수 정복 및 K-강선 고정술 과 수장부 잠김 압박 금속판 내골정술 간의 임상적, 방사선학적 결과를 비교하고자 하였다.
대상 및 방법:2006년 03월부터 2010년 01월 까지 AO C1, 2형 원위 요골 골절로 치 료 받고 12개월 이상 추시가 가능했던 61명을 대상으로 하였다. 임상적 결과는 마지 막 추시 때 disabilities of arm, shoulder and hand score (DASH)와 patient- rated wrist evaluation questionnaires 점수 파악력과 관절의 운동 범위를 조사하 였고 방사선학적 결과는 골유합 여부, 요골의 배측 경사, 요골의 경사각 그리고 요골 의 단축 정도를 측정 비교하였다.
결과:임상적 결과에서는 양 치료군 간의 유의한 차이를 보이지 않았으나 방사선학적 결과에서는 도수 정복 및 K-강선 고정술을 받은 환자에서 잠김 압박 금속판 내고정 술을 받은 환자보다 요골 단축 정도가 유의하게 심한 소견을 보였다.
결론:경피적 핀 고정술 또는 수장부 잠김 금속판 고정술로 치료한 AO C1, 2형 원위 요골 골절 환자에서 임상적으로 유사한 결과를 보이나 잠김 금속판 고정술이 요골의 단축을 방지하는 효과가 더 크다.
색인단어:원위 요골, 불안정 골절, 잠김 압박 금속판, 금속 강선
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non- Commercial License (http://creativecommons.org/
licenses/by-nc/3.0/) which permits unrestricted non- commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
원위 요골 골절로 진단받은 환자 중 수상 2주간의 추시 과정에 서 정복의 소실, 즉 원위 요골의 배측 경사(dorsal tilt)가 20�
이상, 요골 단축이 3 mm 이상, 또는 관절면의 step-off가 2 mm 이상인 불안정 골절과 도수 정복 후 시행한 전산화단층촬 영에서 2 mm 이상의 전위를 보인 환자 군 중 수술을 받고 12 개월 이상 추시가 가능했던 61명을 대상으로 하였다. 수술 방 법의 선택은 기간에 따라 2006년 3월부터 2008년 5월까지는 도수 정복 및 K-강선 고정술을 시행하였으며, 2008년 6월부 터 2010년 1월까지는 잠김 압박 금속판 내고정술을 시행하였 다. 도수 정복 및 K-강선 고정술을 받은 환자가 33명, 잠김 압박 금속판 내고정술을 수장부에 고정한 환자가 28명이었고 환자의 평균 연령은 45.3세(범위: 19-68세)였다.
임상적 결과는 마지막 추시 때 disabilities of arm, shoul- der and hand score (DASH)와 patient-rated wrist eval- uation questionnaires (PRWE) 점수 그리고 관절의 운동 범 위 및 파악력을 근거로 하였다. 방사선학적 결과는 수술 전, 후 그리고 마지막 추시 때의 골유합 여부, 요골의 배측 경사, 요골의 경사각, 척골에 대한 상대적인 요골의 단축 정도 (radial shortening)를 측정 비교하였다. 통계 처리는 Mann- Whitney U 검정법을 이용하였고 SPSS ver. 11.0 (SPSS Inc., Chicago, IL, USA)를 사용하였으며, 통계적 유의 수준 은 p<0.05로 하였다.
2
2.. 수수술술 방방법법
도수 정복 및 금속 강선 고정술의 경우 전신 마취나 상완 신 경총 마취, 또는 환자의 전신 상태가 좋지 않을 경우 국소 마 취 하에 영상 증폭 장치를 보면서 도수 정복을 시행하여 관절 내 골절 간격이 정복되는 것을 확인한 후 1.6-2.4 mm의 K- 강선을 삽입하였다. 강선 삽입 시에는 요골의 경상 돌기 위에 11번 수술 칼로 5 mm 정도 절개를 가한 뒤 끝이 둔한 기구로 골막까지 보이게 하여 신전 건이나 표재성 요골 신경에 손상 이 가지 않도록 하였다. 요골의 경상 돌기에서 약 2-3 mm 근 위부에 강선을 삽입하였고 추가적으로는 원위 요척 관절에 인 접한 요골의 배측면에서 피부에 5 mm 절개 후 신전 건을 보 호하면서 요골의 수장부와 근위부를 향해 강선을 삽입하여 두 강선이 골절의 근위부에서 서로 교차하는 방식으로 고정하도 록 하였다. 2개의 강선으로 고정이 부족하다고 판단된 경우 추 가적을 1-2개를 더 삽입하였다. 수술 후 장상지 부목 고정을 한 뒤 3-4일 후 부종이 감소하면 장상지 석고 고정술을 시행 하였다. 6주 후 외래에서 석고 붕대와 강선을 제거한 후 물리 치료와 재활 치료를 시행하였다. 추시는 수술 후 2주, 4주, 3 개월, 6개월에서 12개월 사이에 추시하였다.
관혈적 정복의 경우 전신 마취나 상완 신경총 마취 후 지혈 대를 장착한 상태에서 요수근 굴곡근(flexor carpi radialis)과 요골 동맥 사이에서 요수근 관절에 해당하는 지점에서부터 근 위부로 약 5-8 cm 정도 절개를 가하였다. 요수근 굴곡근의 건초를 절개한 뒤 건을 척측으로 견인하고 건초의 바닥에 수 직 절개을 가하여 사각 회내근(pronator quadratus)을 노출 하였다. 사각 회내근을 종 절개하여 골절 부위를 노출한 후, 필요한 경우 관절낭을 일부 수직 절개하여 관절내 골절이 정 복되는 것을 육안으로 확인하고 금속 강선으로 임시고정을 하 였다. 영상 증폭 장치로 정복을 확인한 후 잠김 압박 금속판으 로 고정하였다. 금속판은 Synthes 2.4-mm LCP volar col- umn distal radius plate (Synthes, Paoli, PA, USA)를 사용 하였다. 수술 후 3일간 단 상지 부목으로 보호한 뒤 통증이 허 락하는 범위에서 점직적인 물리치료와 재활치료를 시행하였 다. 추시 기간은 도수 정복 및 금속 강선술의 경우와 동일하게 하였다.
결과
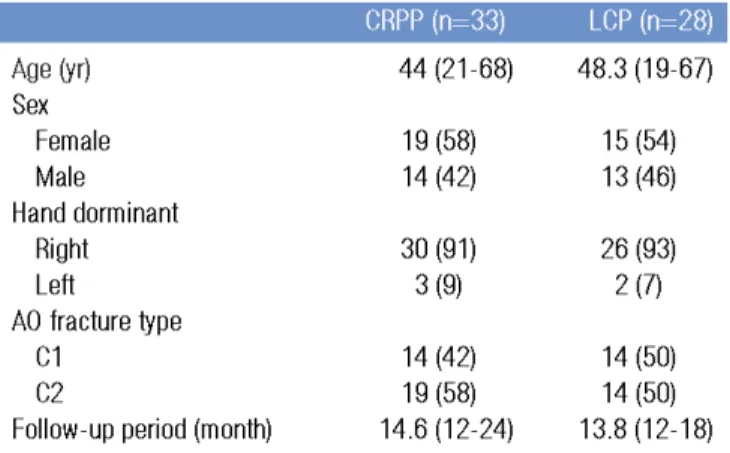
양측 환자 군에서의 성별 분포와 AO type의 분포, 평균 추 시 기간은 유의한 차이를 보이지 않았다(Table 1). 관절의 운 동 범위와 파악력, DASH, PRWE 점수는 도수 정복 및 K-강 선 고정술을 받은 환자에서 각각 15.9±6.1, 11.1±4.6, 잠김 압박 금속판 내고정술을 받은 환자에서 18.1±5.8, 12.3±3.6 였으며 p값은 0.199, 0.249로 양 군 간에 유의한 차이를 보이 지 않았다(Table 2).
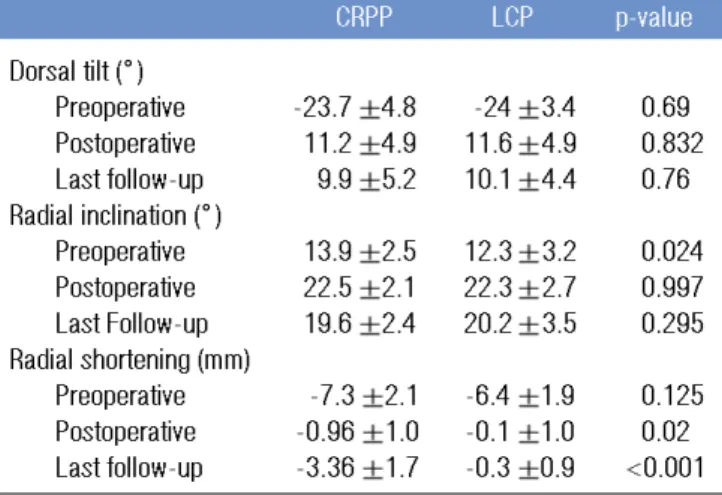
방사선학적 결과에서는 도수 정복 및 K-강선 고정술을 받 은 환자에서 요골 단축 정도가 -3.4±1.7 mm로 측정되어 잠
Table 1.
Dermographic characteristics
Age (yr) 00 44 (21-68) 48.3 (19-67)
Sex Female 19 (58) 15 (54)0
Male 14 (42) 13 (46)0
Hand dorminant
Right 30 (91) 26 (93)0
Left 3 (9) 2 (7)0
AO fracture type
C1 14 (42) 14 (50)0
C2 19 (58) 14 (50)0
Follow-up period (month) 014.6 (12-24) 13.8 (12-18) Values are presented as number (%).
CRPP: closed reduction and percutaneous pin fixation, LCP: open reduction and locking compression plate fixation.
CRPP (n=33) LCP (n=28)
김 압박 금속판 내고정술을 받은 환자에서의 -0.3±0.9 mm 에 비해 유의하게 심한 소견을 보였다(p<0.001). 그러나 마지 막 추시에서 관찰한 결과 척수근 충돌에 의한 후유증을 의심 할 만한 척측 부위의 통증이나 압통은 관찰되지 않았으며 방 사선학적으로 척골과 월상골의 경화나 미란 소견도 관찰되지 않았다(Table 3, Figs. 1, 2).
AO C1형과 C2형간의 요골의 단축 정도를 비교해 본 결과 도수 정복 및 K-강선 고정술을 받은 환자에서 수술 직후 결과 와 마지막 추시 때의 차이가 C1형에 비해 C2형에서 유의하게
저조한 결과를 보였다(Tables 4, 5).
심각한 합병증은 발생하지 않았으며 불유합도 없었다. 도수 정복 및 금속 강선 고정술을 시행한 환자군에서 핀 삽입부 주 위의 감염이 4예, 핀 고정 동안 엄지 손가락의 신전 시 통증을 호소한 경우가 8예 있었으나 핀 제거 후 증상은 없어졌다. 관 혈적 정복술의 경우 일시적으로 수술 후 손가락 굴곡의 어려 움이 있는 경우가 10예 있었으나 4주 내에 모두 호전되었으며 굴곡 건이나 신전 건 자극 증상 및 신경 자극 증상도 관찰되지 않았다.
Table 2.
Functional outcomes at final follow-up for both groups
DASH score 15.9
±6.1 18.1
±5.8 0.199
PRWE score 11.1
±4.6 12.3
±3.6 0.249
Range of motion (
。)
Extension 0046
±5.7 47.5
±5.9 0.359
Flexion 53.5
±6.9 56.5
±8.6 0.095
Supination 74.5
±9.5 73.6
±9.1 0.647 Pronation 076.9
±12.4 079.5
±10.1 0.444 Radial deviation 18.3
±4.8 17.9
±5.3 0.634 Ulnar deviation 24.5
±6.9 25.2
±6.1 0.767 Grip strength (kp) 19.4
±5.6 20.9
±3.9 0.202 Values are presented as mean
±standard deviation.
CRPP: closed reduction and percutaneous pin fixation, LCP: open reduction and locking compression plate fixation, DASH: disabilities of arm, shoulder and hand score, PRWE: patient-rated wrist evalua- tion questionnaires.
CRPP LCP p-value
Table 3.Radiologic mearsurements for both groups Dorsal tilt (
。)
Preoperative -23.7 4.8- --24 3.4 00.690
Postoperative 11.2 4.9 11.6 4.9 00.832
Last follow-up 09.9 5.2 10.1 4.4 00.760 Radial inclination (
。)
Preoperative 13.9 2.5 12.3 3.2 00.024
Postoperative 22.5 2.1 22.3 2.7 00.997
Last Follow-up 19.6 2.4 20.2 3.5 00.295 Radial shortening (mm)
Preoperative --7.3 2.1 -6.4 1.9 00.125
Postoperative --0.96 1.00 -0.1 1.0 00.020 Last follow-up --3.36 1.70 -0.3 0.9 <0.001 Values are presented as mean standard deviation.
CRPP: closed reduction and percutaneous pin fixation, LCP: open reduction and locking compression plate fixation.
CRPP LCP p-value
FFFFiiiigggg.... 1111.... ((((AAAA)))) Preoperative radiographs show radial shortening
of 4.5 mm and metaphyseal comminution. ((((BBBB)))) After open
reduction and locking compression plate fixation, radiologi-
cal indices are within acceptable range. ((((CCCC)))) At last follow-
up, no evidence of reduction loss including radial shorten-
ing is observed.
고찰
원위 요골 골절에서 관절의 침범 여부는 예후와 치료 방법 이 다르기 때문에 구분되어야 한다12,13. 전위된 요골 골절의 치 료에서 해부학적 복원이 좋은 결과를 가져온다는 것은 많은 연구에서 보고되고 있다14-17. 2 mm 이상의 관절면의 전위나 불일치는 추후 퇴행성 관절염을 초래할 가능성이 높은 것으로 알려져 있다18,19. 요골 단축이 6 mm 이상이 되면 척수근 충돌 (ulnocarpal impingement), 원위 요척 관절의 통증, 회내전 과 회외전의 감소 등이 발생할 수 있다20-22. Kazuki 등23은 배 측 경사 정도에 따른 관절의 운동 범위와 수근 관절의 정렬 (carpal alignment) 변화를 연구하여, 10�이하의 배측 경사 에서는 관절의 운동 범위와 수근 관절의 정렬에 미치는 영향 이 적은 것으로 보고하였다. 또한 요골의 경사각이 변할 경우 에도 수부의 파악력과 주상-월상 관절의 부하에 좋지 않은 영 향을 미치는 것으로 보고되었다24,25. 일반적으로 2 mm 이상의 관절면의 부조화, 20�이상의 배측 경사, 그리고 5 mm 이상 의 요골 단축은 정복하는 것이 바람직하다14,26,27. 본 연구에서 는 관절면의 부조화에 대한 비교 분석은 하지 않았으며 방사
선학적 결과에서는 요골의 단축에서만 의미 있는 차이를 보였 다. 경피적 핀 고정술만 시행한 환자군 내에서 요골 단축이 C1 (-2±0.9)보다 C2 (-4.2±1.5)에서 의미 있게 증가함을 알 수 있었다. 그러나 추시 기간 내에 방사선 사진에서 척수근 충돌 에 의한 방사선학적 변화를 발견할 수 없었고 척수근 충돌을 시사하는 증상은 비특이적이어서 객관적인 비교는 어려웠다.
기존의 보고를 근거로 할 때 척수근 충돌의 발생 가능성을 배 제할 수 없기에 장기적인 추시 관찰을 통한 추가적인 연구가 필요할 것으로 생각된다.
AO C1, 2형도 도수 정복으로 안정된 정복을 얻지 못하면 흔 히 볼 수 있는 불안정 원위 요골 골절에 포함된다. AO C1, 2형 에 국한된 연구가 많지 않은 관계로 본 연구의 이론적 배경은 불안정 원위 요골 골절을 대상으로 한 연구를 참고하였다. 불 안정하면서 관절을 침범한 원위 요골 골절에서의 수술적 치료 법으로는 비관혈적 방법으로 도수 정복 후 경피적 금속 강선 고정술 또는 외고정기 고정술이나 두 가지 방법의 병용, 그리 고 관혈적 방법으로 고식적인 금속판과 잠김 압박 금속판을 이용한 방법 등이 이용되고 있다. 본 연구에서는 금속 강선을
TTTTaaaabbbblllleeee 4444.... Comparison of Radial shortening between AO type C1 and
C2 at last follow-up (unit:mm)
CRPP 00--2 0.9 -4.2 1.50 <0.001
LCP -0.18 1.1 -0.4 0.78 <0.538
CRPP: closed reduction and percutaneous pin fixation, LCP: open reduction and locking compression plate fixation.
C1 C2 p -value
TTTTaaaabbbblllleeee 5555.... Comparison of radial shortening changes from postoperation to last follow-up between AO type C1 and C2 (unit:mm) : (value = last follow-up value - postoperative value)
CRPP 1.007 0.732 3.247 1.242 <0.001
LCP 0.479 0.487 0.357 0.457 <0.428
CRPP: closed reduction and percutaneous pin fixation, LCP: open reduction and locking compression plate fixation.
C1 C2 p -value
FFFFiiiigggg 2222.... ((((AAAA)))) Preoperative radiographs show radial shortening of 4
mm and metaphyseal comminution. ((((BBBB)))) After closed reduction
and percutaneous pin fixation, radiological indices are within
acceptable range. ((((CCCC)))) At last follow-up, reduction loss, especial-
ly radial shortening is observed.
이용한 비관혈적인 방법과 잠김 압박 금속판을 이용한 관혈적 방법을 비교 대상으로 하였다. 각각의 치료법에 대한 기존의 연구를 참고해보면 잠김 압박 금속판은 상대적으로 튼튼하게 고정되므로 수술 후 빨리 관절 운동이 가능하여 수지와 손목 관절의 강직을 최소화하면서 정복의 소실이 적다는 점 때문에 많은 인기를 얻고 있으며 좋은 결과들이 보고되고 있다28-32. 도 수 정복 및 금속 강선 고정술은 상대적으로 비침습적이고 시 술 시간이 짧으며 비용적인 측면에서도 장점이 있으나 상대적 으로 고정력에서 떨어지고 골유합이 이루어지는 동안 정복의 소실과 그에 따른 기능 감소가 단점으로 지적되고 있다33. Glickel 등34은 도수 정복 후 경피적 금속 강선 고정술의 장기 추시 연구에서 우수한 방사선학적 및 임상적 결과를 보고하였 다. 기존의 경피적 금속 강선 고정술이 가지는 우려를 줄이기 위해 요골의 경상 돌기 근처에 핀을 삽입할 때 관혈적 방법을 사용하여 건이나 신경의 손상을 최소화하였고 술 후 설탕 집 게 부목을 사용하여 전완부의 회전을 막아 핀 주위 감염의 위 험을 줄였다. 본 연구에서도 핀을 삽입할 때마다 0.5 cm 절개 후 골막까지 육안으로 확인하였고 장상지 석고 붕대 고정을 4-6주 시행하였다. 금속 강선 삽입 후 일시적인 핀 삽입 주변 의 피부 감염이 7예에서 발생하였으나 신전 건이나 표재 요골 신경의 자극 증상은 발생하지 않았다.
관혈적 정복 및 금속판을 이용한 수술적 치료 후 요수근 굴 곡 건, 장무지 굴곡 건이 돌출된 나사못의 머리에 의해 기계적 자극을 받을 수 있으며 심할 경우 파열이 될 위험이 있는 것으 로 알려져 있다34. 그러나 잠김 압박 금속판은 나사 머리의 돌 출이 최소화되게 고안되어 있고 영상 증폭 장치로 확인하면서 요골의 배측 피질골을 관통하지 않도록 나사못 길이를 적절하 게 선택하면 충분히 예방할 수 있으며 본 연구 대상 환자에서 는 발생하지 않았다.
Knox 등10은 사체를 이용한 생역학적 연구에서 금속 강선을 이용한 고정술이 잠김 압박 금속판을 이용한 고정술 보다 고 정력이 약하다고 하였으나 실제로 금속 강선 고정술만 시행하 는 것이 아니라 석고 붕대 고정술을 병용한다는 사실을 간과 하였다. 즉 잠김 압박 금속판과 금속 강선 경피적 고정술에 석 고붕대 고정술이 추가된 생역학적 비교 연구는 아직 없다. 현 재까지 두 가지 수술법에 대한 임상적 결과나 방사선적 결과 에 대한 비교 연구는 많지 않으며 둘 중 어떤 방법이 우수한 지는 아직 결론이 나지 않은 상태이다. Rozental 등35은 45명 의 불안정 원위 요골 골절 환자를 대상으로 시행한 전향적 연 구에서 수장부 잠김 압박 금속판 내고정술과 도수 정복 후 금 속 강선 고정술 간의 임상적 결과를 비교한 결과 수술 후 6주 까지는 임상적 결과가 금속판 내고정술 환자에서 우수하나 그
후 서서히 차이가 줄어들어 1년 추시에서는 의미 있는 차이를 보이지 않았다고 보고하면서, 술 후 초기의 임상 결과를 바탕 으로 빠른 기능적 복귀가 필요한 환자에서 관혈적 방법을 추 천하였다. 이와는 다소 상이한 연구로서 Kreder 등36은 179명 의 관절을 침범한 전위된 원위 요골 골절 환자를 대상으로 고 식적 금속판 내고정술 과 도수 정복 후 금속 강선 및 외고정기 고정술을 비교한 무작위 연구에서 수술 후 첫 2년 동안은 비관 혈적인 치료를 받은 환자에서 관혈적 치료를 받은 경우보다 일상 생활로의 복귀나 기능적 측면에서 더 우수한 결과를 보 였고 수술 후 1년 이후에는 기능적 결과의 변화가 없으므로 1 년 이상의 추시는 필요 없다고 하였다. 본 연구에서도 마지막 추시의 임상적 결과 비교에서 양측 환자 군에서 의미 있는 차 이를 보이지 않았다. 1년 이상 추시는 요골 단축에 의해 발생 할 수 있는 합병증의 발생 여부와 이것이 임상 결과에 미치는 영향을 관찰하기 위해 필요할 것으로 생각된다.
Kim 등37은 후방 불안정 원위 요골 골절에서 Kapandji 술 식과 전방 잠김 압박 금속판과의 임상적 및 방사선적 결과를 비교한 연구에서 DASH 점수와 동통 점수에서 잠김 압박 금속 판이 더 우수하다고 하였고 방사선적 결과에서는 요골 단축에 서 잠김 압박 금속판이 더 좋은 결과를 보였다고 하였다. 본 연구에서는 AO C1, 2형을 대상으로 임상적 평가를 하여 비교 한 결과 양측에서 차이를 보이지 않았으나 방사선적 결과에서 잠김 압박 금속판이 요골 단축을 방지하는 효과가 큰 것으로 조사되었다. 본 연구의 한계는 추시 기간이 12-24개월로 장기 적으로 외상 후 관절염 등에 대한 연구가 필요할 것이다.
결론
AO C1, 2형 요골 골절의 수술적 치료 결과 비교에서 임상적 결과에서는 도수 정복 후 금속 강선 고정술과 잠김압박 금속 판 내고정술 간에 유의한 차이를 보이지 않았으나 방사선학적 으로 잠김 압박 금속판 내고정술을 받은 환자에서 요골 단축 의 정도가 적은 결과를 보였다.
참고문헌
1. Fernandez DL, Wolfe SW. Distal radius fractures. In:
Geen DP, Hotchkiss RN, Pederson WC, Wolfe SW, edi- tors. Green’s operative hand surgery. 5th ed. Philade- phia: Elsevier Churchill livingstone; 2005. p645-710.
2. Horne G. A prospective randomized trial of external fix- ation and plaster cast immobilization in the treatment
of distal radius fractures. J Orthop Trauma. 1991;5:246.
3. Kapoor H, Agarwal A, Dhaon BK. Displaced intra-artic- ular fractures of distal radius: a comparative evaluation of results following closed reduction, external fixation and open reduction with internal fixation. Injury.
2000;31:75-9.
4. Cooney WP 3rd, Linscheid RL, Dobyns JH. External pin fixation for unstable Colles’ fractures. J Bone Joint Surg Am. 1979;61:840-5.
5. Fitoussi F, Ip WY, Chow SP. Treatment of displaced intra-articular fractures of the distal end of the radius with plates. J Bone Joint Surg Am. 1997;79:1303-12.
6. Azzopardi T, Ehrendorfer S, Coulton T, Abela M.
Unstable extra-articular fractures of the distal radius: a prospective, randomised study of immobilisation in a cast versus supplementary percutaneous pinning. J Bone Joint Surg Br. 2005;87:837-40.
7. Handoll HH, Madhok R. Surgical interventions for treating distal radial fractures in adults. Cochrane Database Syst Rev. 2003;(3):CD003209.
8. Orbay JL, Fernandez DL. Volar fixed-angle plate fixa- tion for unstable distal radius fractures in the elderly patient. J Hand Surg Am. 2004;29:96-102.
9. Drobetz H, Kutscha-Lissberg E. Osteosynthesis of distal radial fractures with a volar locking screw plate system.
Int Orthop. 2003;27:1-6.
10. Knox J, Ambrose H, McCallister W, Trumble T.
Percutaneous pins versus volar plates for unstable dis- tal radius fractures: a biomechanic study using a cadav- er model. J Hand Surg Am. 2007;32:813-7.
11. Orbay JL, Fernandez DL. Volar fixation for dorsally dis- placed fractures of the distal radius: a preliminary report. J Hand Surg Am. 2002;27:205-15.
12. Schneeberger AG, Ip WY, Poon TL, Chow SP. Open reduction and plate fixation of displaced AO type C3 fractures of the distal radius: restoration of articular congruity in eighteen cases. J Orthop Trauma. 2001;15:
350-7.
13. Kreder HJ, Hanel DP, McKee M, Jupiter J, McGillivary G, Swiontkowski MF. Consistency of AO fracture classifi- cation for the distal radius. J Bone Joint Surg Br. 1996;
78:726-31.
14. Ark J, Jupiter JB. The rationale for precise management of distal radius fractures. Orthop Clin North Am.
1993;24:205-10.
15. Howard PW, Stewart HD, Hind RE, Burke FD. External
fixation or plaster for severely displaced comminuted Colles’ fractures? A prospective study of anatomical and functional results. J Bone Joint Surg Br. 1989;71:68-73.
16. McQueen M, Caspers J. Colles fracture: does the anatomical result affect the final function? J Bone Joint Surg Br. 1988;70:649-51.
17. Jenkins NH, Jones DG, Johnson SR, Mintowt-Czyz WJ.
External fixation of Colles’ fractures. An anatomical study. J Bone Joint Surg Br. 1987;69:207-11.
18. Bradway JK, Amadio PC, Cooney WP. Open reduction and internal fixation of displaced, comminuted intra- articular fractures of the distal end of the radius. J Bone Joint Surg Am. 1989;71:839-47.
19. Knirk JL, Jupiter JB. Intra-articular fractures of the distal end of the radius in young adults. J Bone Joint Surg Am.
1986;68:647-59.
20. Fernandez DL. Radial osteotomy and Bowers arthro- plasty for malunited fractures of the distal end of the radius. J Bone Joint Surg Am. 1988;70:1538-51.
21. Fernandez DL. Correction of post-traumatic wrist deformity in adults by osteotomy, bone-grafting, and internal fixation. J Bone Joint Surg Am. 1982;64:1164-78.
22. Jupiter JB, Masem M. Reconstruction of post-traumatic deformity of the distal radius and ulna. Hand Clin.
1988;4:377-90.
23. Kazuki K, Kusunoki M, Yamada J, Yasuda M, Shimazu A. Cineradiographic study of wrist motion after fracture of the distal radius. J Hand Surg Am. 1993;18:41-6.
24. Jenkins NH, Mintowt-Czyz WJ. Mal-union and dysfunc- tion in Colles’ fracture. J Hand Surg Br. 1988;13:291-3.
25. Palmer AK, Werner FW. Biomechanics of the distal radioulnar joint. Clin Orthop Relat Res. 1984:26-35.
26. Hastings H 2nd, Leibovic SJ. Indications and tech- niques of open reduction. Internal fixation of distal radius fractures. Orthop Clin North Am. 1993;24:309-26.
27. Altissimi M, Antenucci R, Fiacca C, Mancini GB. Long- term results of conservative treatment of fractures of the distal radius. Clin Orthop Relat Res. 1986;(206):202- 10.
28. Willis AA, Kutsumi K, Zobitz ME, Cooney WP 3rd.
Internal fixation of dorsally displaced fractures of the distal part of the radius. A biomechanical analysis of volar plate fracture stability. J Bone Joint Surg Am.
2006;88:2411-7.
29. Leung F, Zhu L, Ho H, Lu WW, Chow SP. Palmar plate fixation of AO type C2 fracture of distal radius using a
locking compression plate: a biomechanical study in a cadaveric model. J Hand Surg Br. 2003;28:263-6.
30. Chung KC, Watt AJ, Kotsis SV, Margaliot Z, Haase SC, Kim HM. Treatment of unstable distal radial fractures with the volar locking plating system. J Bone Joint Surg Am. 2006;88:2687-94.
31. Rozental TD, Blazar PE. Functional outcome and com- plications after volar plating for dorsally displaced, unstable fractures of the distal radius. J Hand Surg Am.
2006;31:359-65.
32. Wright TW, Horodyski M, Smith DW. Functional out- come of unstable distal radius fractures: ORIF with a volar fixed-angle tine plate versus external fixation. J Hand Surg Am. 2005;30:289-99.
33. Mah ET, Atkinson RN. Percutaneous Kirschner wire sta- bilisation following closed reduction of Colles' frac- tures. J Hand Surg Br. 1992;17:55-62.
34. Glickel SZ, Catalano LW, Raia FJ, Barron OA, Grabow R, Chia B. Long-term outcomes of closed reduction and
percutaneous pinning for the treatment of distal radius fractures. J Hand Surg Am. 2008;33:1700-5.
35. Rozental TD, Blazar PE, Franko OI, Chacko AT, Earp BE, Day CS. Functional outcomes for unstable distal radial fractures treated with open reduction and internal fixa- tion or closed reduction and percutaneous fixation. A prospective randomized trial. J Bone Joint Surg Am.
2009;91:1837-46.
36. Kreder HJ, Hanel DP, Agel J, McKee M, Schemitsch EH, Trumble TE, et al. Indirect reduction and percutaneous fixation versus open reduction and internal fixation for displaced intra-articular fractures of the distal radius: a randomised, controlled trial. J Bone Joint Surg Br.
2005;87:829-36.
37. Kim JK, Park HS, Jeong BJ. Comparative analysis of the results of dorsally unstable distal radius fractures between kapandji technique and volar locking plate fix- ation. J Korean Soc Surg Hand. 2008;13:217-22.
Clinical and Radiologic Outcomes of AO Type C1, 2 Distal Radius Fractures Treated with
Percutaneous Pinning or Volar Locking Plating
Yoon-Suk Hyun, MD, Kyung-Won Song, MD, Hyun-Jin Park, MD, Hyun-Tai Park, MD
Department of Orthopedic Surgery, Kangdong Sacred Heart Hospital, Hallym University School of Medicine, Seoul, Korea
Purpose:To compare clinical and radiological results between closed reduction followed by percutaneous K-wire fix- ation and volar locking compression plate fixation in the treatment of AO type-C1, 2 fractures of the distal radius.
Materials and Methods:The subjects of this study were 61 patients who had a AO type-C1,2 fracture of the distal radius treated from March 2006 to January 2010, and were followed up for over 12 months. Clinical evaluations included disabilities of arm, shoulder and hand score (DASH) score, patient-rated wrist evaluation questionnaires (PRWE) score, the Grip strength, and the range of joint motion at the last follow-up, and radiological assessment included the presence of bony union, the dorsal tilt angle of the radius, the inclination of the radius, and the radial shortening.
Results:The range of joint motion, the grip strength, DASH and PRWE demonstrated no significant difference between the two groups. Radiological results revealed that the patients treated with percutaneous K-wire fixation showed greater radial shortening than those treated with locking compression plate fixation.
Conclusion:Although clinical results are similar between volar locking plating and percutaneous pinning in the treatment of AO C1, 2 distal radius fractures, volar locking plating is more effective in preventing radial shortening during fracture healing.
Keywords:Distal radius, Unstable fracture, Locking compression plate, K-wire
Received:February 28, 2011 Revised:August 22, 2011 Accepted:August 24, 2011
Correspondence to:Kyung-Won Song, MD
Department of Orthopedic Surgery, Kangdong Sacred Heart Hospital, Hallym University School of Medicine, Kangdong Sacred Heart Hospital, 445 Gil-dong, Kangdong-gu, Seoul 134-701, Korea
TEL:+82-2-2224-2230 FAX:+82-2-489-4391 E-mail:[email protected]