Introduction
Worldwide, lower back pain is associated with high economic costs, disability, and decreased productivity.
Although there are various guidelines on the management of lower back pain, its overall management, including diagnosis and treatment, still remains controversial [1-2].
Various conservative treatments are used to improve and recover from neurological symptoms of degenerative
disc disease [3]. Of such treatment methods, traction treatment maintains the intervertebral height in degenerative disc disease patients, slows down the degenerative changes of discs [4], decreases lower back pain, and reduces the compression of discs within the vertebrae [5-6]. However, other studies have reported that the effects of traction are unclear [7], and the effects remain controversial[8-9].
Flexion-distraction spinal manipulation, which is a type of low-velocity variable amplitude spinal https://doi.org/10.14474/ptrs.2021.10.2.235
eISSN 2287-7584 pISSN 2287-7576
Phys Ther Rehabil Sci 2021, 10(2), 235-242
www.jptrs.org
Immediate Effect of Flexion-Distraction Spinal Manipulation on Intervertebral Height, Pain, and Spine Mobility in Patients with Lumbar Degenerative Disc Disease
Taejin Pi
a, Yijung Chung
ba
Department of Physical Therapy, The Graduate School, Sahmyook University, Seoul, Republic of Korea
b
Department of Physical Therapy, College of Health and Welfare, Sahmyook University, Seoul, Republic of Korea
Objective: This study aimed to investigate the short-term effects of flexion-distraction spinal manipulation on intervertebral height, pain, spine mobility in patients with lumbar degenerative disc disease.
Design: Randomized controlled trial with a pretest-posttest control group design
Methods: A total of 96 participants with degenerative disc disease participated in the study and were randomly divided into two groups. Both groups received intervention for 3-5 minutes a day. The experimental group (n=48) underwent flexion-distraction spinal manipulation for 3-5 minutes, and the control group (n=48) was maintained in the same position as the experimental group for 5 minutes without any intervention. The intervertebral height was measured by computed tomography, pain was assessed using visual analog scale, and the spine in flexion mobility was measured using the finger-to-floor distance test and passive straight leg raise test. Pre-test and post-test measurements were obtained.
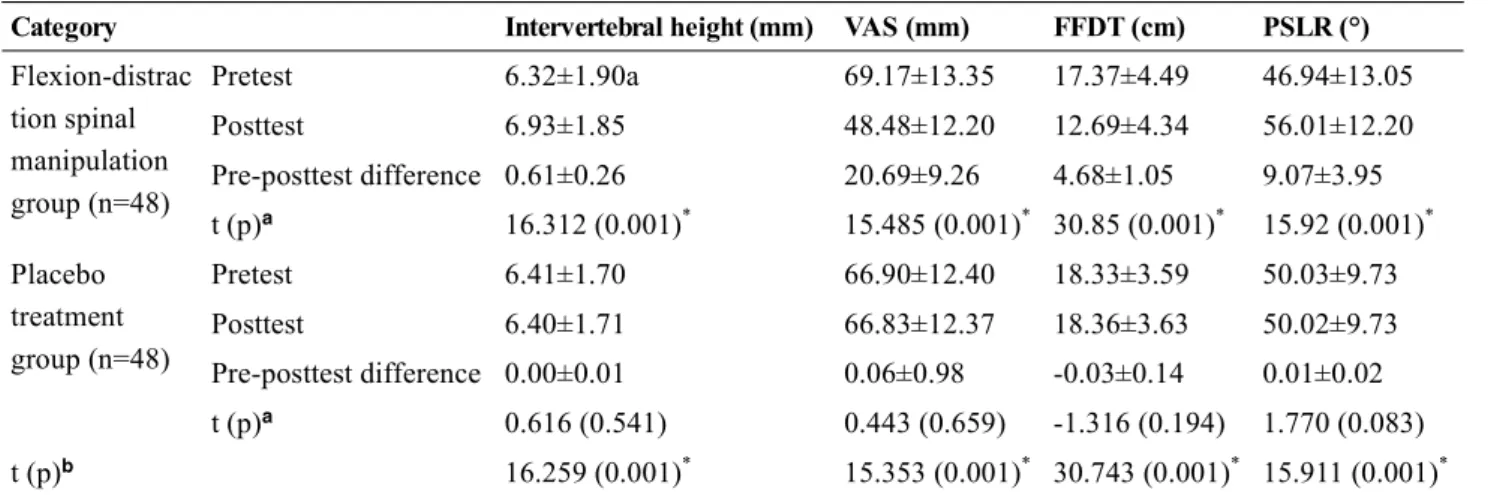
Results: The experimental group showed significant improvement in intervertebral height, degree of pain, and spinal mobility (p<0.05). The intervertebral height increased from 6.32±1.90 to 6.93±1.85 mm (p<0.05), lower back pain decreased from 69.17±13.35 mm to 48.48±12.20 mm (p<0.05), lumbar spine mobility changed from 17.37±4.49 to 12.69±4.34 cm (p<0.05), and passive straight leg raise test range increased from 46.94±13.05° to 56.01±12.20° (p<0.05).
Conclusions: This study suggests that flexion-distraction spinal manipulation could be an effective treatment for decreasing pain and improving function in patients with degenerative disc disease.
Key Words: Intervertebral disc degeneration, Range of motion, Articular
Received: Jun 13, 2021 Revised: Jun 22, 2021 Accepted: Jun 22, 2021
Corresponding author: Yijung Chung (ORCID https://orcid.org/0000-0002-2431-8895) Department of Physical Therapy, College of Health and Welfare, Sahmyook University 815 Hwarang-ro, Nowon-gu, Seoul, Republic of Korea [01795]
Tel: +82-2-3399-1637 Fax: +82-2-3399-1639 E-mail: [email protected]
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2021 Korean Academy of Physical Therapy Rehabilitation Science
manipulation method conducted to cause traction, provides slow traction and mobility through clinician’s manual manipulation and special manipulation treatment equipment[10].
Flexion-distraction spinal manipulation maintains the intervertebral height, thereby preventing degeneration of the peripheral annulus fibrosus, which is sensitive to pain. Through this, the disc pressure is reduced, and the resulting centripetal force repositions the laterally displaced nucleus pulposus to the center [11]. Moreover, the manipulation recovers the subluxation of the spinal facet joint to maintain posterior spinal mobility, and it decreases pain while improving physical function through improved mobility and posture [11-12].
Decreases in the intervertebral height result from the compression created by fluid leaking from discs and spinal endplates and changes in elasticity [13].
Repeated compression of spinal endplates gradually causes degeneration of the nucleus pulposus, delivers greater loads to the annulus fibrosus around the nucleus pulposus, and destroys the structure of the nucleus pulposus, ultimately leading to decreased intervertebral height [14].
Spinal manipulation decreases pain and leads to functional improvement in patients with symptoms of lumbar degenerative disc disease by influencing how the body processes pain [15-16]. However, other previous studies have reported that flexion-distraction spinal manipulation does not improve pain [17-18].
In particular, structural changes observed in degenerative disc disease decrease the intervertebral height as well as spinal mobility [19]. It would also be significant to verify the effects of flexion-distraction spinal manipulation on lumbar joints of patients with degenerative disc disease since decreased hip flexion mobility influences the load on the lumbar vertebrae [19-20]. In addition, a study applied flexion-distraction spinal manipulation to patients with herniated discs in straight leg raise range [21]. However, research on the influence of flexion-distraction spinal manipulation on intervertebral height, pain, and lumbar spinal mobility has been lacking. In other words, there is a need to investigate how flexion-distraction spinal manipulation influences pain and lumbar spinal mobility of degenerative disc disease patients. Therefore, this study aimed to investigate the short-term effect of flexion-distraction
spinal manipulation on intervertebral height, pain, spine mobility in this population through computed tomography (CT).
Methods
Participants
The study was conducted on 96 patients who met the selection criteria among a total of 132 patients.
Study participants were 96 patients with lower back pain who presented to S Hospital in Seoul. The inclusion criteria for the study were as follows: patients diagnosed with degenerative disc disease of L5-S1 on magnetic resonance imaging, those aged between 20 and 60 years, those who have had more than 3 months of continued lower back pain,1 those who have not had flexion-distraction spinal manipulation for 3 months prior to this study, those whose Korean Oswestry Disability Index score was 21 or above [22], those whose pain was rated as 45 mm or above on visual analog scale,10 and those whose straight leg raise test was positive at angles smaller than 70° [23].
Of these patients, those taking analgesics, with cauda equina syndrome, with spondylolisthesis or spondylolysis, who had previous spinal surgeries, with symptoms of radiculopathy, with central nervous system injuries, and contraindicated for spinal manipulation were excluded from the study.
Study methods and experiments
The purpose, methods, and other pertinent information were explained in detail to all participants, and they were also informed that they may withdraw from the study whenever they desire. They all signed written consent forms. The present study was approved by the institutional review board (approval number:
2-1040781-AB-N-01-2016107HR). To minimize bias through single blinding, one physical therapist with 7 years of clinical experience made measurements and another physical therapist with more than 10 years of clinical experience provided the interventions.
Participants with similar general characteristics were
paired and numerically coded. The numbers were
placed in an envelope and drawn randomly to assign
48 participants to the experimental group and the
remaining 48 to the placebo group. There was no dropout of participants, and the data collected from 48 experimental group participants and 48 placebo group participants were used for statistical analysis.
A Zenith Cox flexion table (Zenith Cox flexion table, Standex company, USA), which comprises three pieces (head, thoracic/lumbar spine, and lower extremities) that can move spine joints, was used for flexion-distraction spinal manipulation. The participants were lying in a prone position so that their anterior superior iliac spine was positioned at the end of the thoracic/lumbar spine piece of the table. The spinous process of the participants’ L5 was positioned in between the thenar and hypothenar eminence of one hand of the therapist, and the therapist’s other hand was placed on the end handle of the table used to cause distraction with flexion, lateroflexion, and rotation. Both ankles of the participants’ were fixed with a belt.
The therapist pushed their hand on the patient’s L5 spinous process superio-anteriorly to fix the spinous process and manipulated the table inferio-anteriorly to create a distraction with flexion, lateroflexion, and rotation.
The manipulation was repeated according to the patient’s responses. When the patient did not have any abnormal symptoms, one set (2-3 seconds of distraction with flexion and lateroflexion *5 and 4 seconds of distraction with rotation *5) was applied. Three sets comprised the intervention, which took 3-5 minutes.
The distraction was created in a direction that allowed for flexion and all other physiological mobility [24].
The participants in the placebo treatment group were lying down in a prone position on the Cox flexion table in the same environment as for those receiving flexion-distraction spinal manipulation. The therapist only maintained light touch to the site of the lesion without any mechanical manipulation, and the treatment was maintained for 3-5 minutes.
Measurement tools and data collection
CT (Alexion 16, Toshiba Co., Japan) was used to measure intervertebral height, and the CT scanner had an error range of 2% (±0.2 mm) when tested in 2016.
Cross-section images obtained from the scanner were
reconstructed into sagittal images to obtain mid-sagittal images, which were then sent to PACS (ViewRex, TechHeim, Republic of Korea). The images were zoomed in twice to measure the intervertebral height between L5 and S1 (Figure 1).
For measurement of the intervertebral height, anterior and posterior heights were measured at the anterior and posterior ends of the vertebral bodies, and the mid-intervertebral height was measured by connecting the center of the upper and lower ends of the disc [25].
The anterior intervertebral height (A), mid-intervertebral height (B), and posterior intervertebral height (C) were summed and divided into 3 (A+B+C/3) to obtain the intervertebral height used for analysis [26].
Visual analog scale was used to measure lower back pain. The visual analog scale included an ungraduated horizontal 100-mm line. Zero defined no pain and 100 defined the most severe pain, and the participants were asked to mark the current level of their subjective pain within the range between 0 and 100 mm. The visual analog scale is an effective, appropriate method to measure chronic and acute pain, and intra-rater reliability is r=0.87 in the test-retest measurement [27].
Finger-to-floor distance test was used to measure lumbar mobility. This test measures the maximal possible spinal flexion range, and the participants bent their body forward until there was a functional limitation. (The test is easy to administer and has a high inter-rater reliability of r =0.96-0.98 [28].
Passive straight leg raise test was used to measure
the range of motion of lower extremities. A smartphone
application (Clinometer-level and Slope Finder, Plaincode
Software Solutions, Germany) was used to measure the
Figure 1. Measurement of intervertebral height
angle, and a smartphone was placed on the center of lateral thighs of the participants to measure the angle.
The application has high reliability: intra-rater reliability of r=0.78 and inter-rater reliability of r=0.90 [29].
Passive straight leg raise is easy to administer and is highly reliable with r=0.87 [30].
Analysis
All statistical analyses were conducted on SPSS 19.0 (ver. 19.0, IBM Co., USA). Descriptive statistics were used for the general characteristics of the participants, and socio-demographic variables were analyzed in real numbers. Medical characteristics were analyzed as mean and standard deviation. Paired-sample t-tests were conducted to assess the differences in the dependent variables within groups according to intervention, and independent samples t-tests were conducted to assess between-group differences according to intervention. The level of statistical significance (α) of all data was set as 0.05.
Results
In this present study, 132 patients were initially recruited, and 36 patients who did not satisfy the selection criteria were excluded. As a result, there
were a total of 96 participants.
When the homogeneity of the two groups was assessed in terms of general characteristics and dependent variables, the groups did not differ significantly (Table 1).
In the flexion-distraction spinal manipulation group, the intervertebral height increased from 6.32±1.90 mm to 6.93±1.85 mm, with a significant difference of 0.61±0.26 mm (p<0.05) (Figure 2) and lower back pain decreased from 69.17±13.35 mm to 48.48±12.20 mm, with a significant difference of 20.69±9.26 mm (p<0.05) (Table 2, Figure 3). The treatment group also had a significant decrease in lumbar spine mobility of 4.68±1.05 cm, from 17.37±4.49 cm to 12.69±4.34 cm (p<0.05) (Figure 4), and a significant increase in passive straight leg raise test range of 9.07±3.95° from 46.94±13.05° to 56.01±12.20° (p<0.05) (Table 2, Figure 5).
Discussion
Maintenance of intervertebral height decreases burdens on spinal facet joints and recovers spinal mobility, whereas recovery of intervertebral height widens respective intervertebral foramina, distracts the posterior annulus fibrosus, and increases the diameter Category Flexion-distraction spinal manipulation
(n=48)
Placebo treatment group (n=48)
t (p)
Sex (male/female) 22/26 23/25 0.202 (0.840)
Age (years) 43.31±11.25ba 42.27±13.27 0.456 (0.649)
Height (cm) 165.85±7.94 166.44±10.345 -0.310 (0.757)
Weight (kg) 64.96 ±9.26 66.25±14.93 -0.509 (0.612)
K-ODI (score) 24.42±2.99 24.15±2.81 0.457 (0.649)
Intervertebral height (mm) 6.32±1.90 6.41±1.70 -0.217 (0.828)
VAS (mm) 69.17±13.35 66.90±12.40 0.863 (0.390)
FFDT (cm) 17.37±4.49 18.33±3.59 -1.155 (0.251)
PSLR (°) 46.94±13.35 50.02±9.73 -1.312 (0.193)
Values are presented as mean±standard deviation or number
FFDT: finger-to-floor distance test, K-ODI: Korean Oswestry disability index, PSLR: passive straight leg raise, VAS:
visual analog scale.
Table 1. Test of homogeneity of the participants in terms of general characteristics, medical characteristics, and dependent
variables (n=96)
Figure2. Pre-posttest changes in intervertebral height after intervention
FDSM: flexion-distraction spinal manipulation, IVS: intervertebral space.
Figure 3. Pre-posttest changes in lower back pain after intervention
FDSM: flexion-distraction spinal manipulation, VAS: visual analog scale.
Figure 4. Pre-posttest changes in lumbar spinal mobility after intervention
FDSM: flexion-distraction spinal manipulation, FFDT: finger-to-floor distance test.
Figure 5. Pre-posttest changes in passive straight leg raise test range after intervention
FDSM: flexion-distraction spinal manipulation, PSLR, passive straight leg raise.
Category Intervertebral height (mm) VAS (mm) FFDT (cm) PSLR (°)
Flexion-distrac tion spinal manipulation group (n=48)
Pretest 6.32±1.90a 69.17±13.35 17.37±4.49 46.94±13.05
Posttest 6.93±1.85 48.48±12.20 12.69±4.34 56.01±12.20
Pre-posttest difference 0.61±0.26 20.69±9.26 4.68±1.05 9.07±3.95
t (p)
a16.312 (0.001)
*15.485 (0.001)
*30.85 (0.001)
*15.92 (0.001)
*Placebo
treatment group (n=48)
Pretest 6.41±1.70 66.90±12.40 18.33±3.59 50.03±9.73
Posttest 6.40±1.71 66.83±12.37 18.36±3.63 50.02±9.73
Pre-posttest difference 0.00±0.01 0.06±0.98 -0.03±0.14 0.01±0.02
t (p)
a0.616 (0.541) 0.443 (0.659) -1.316 (0.194) 1.770 (0.083)
t (p)
b16.259 (0.001)
*15.353 (0.001)
*30.743 (0.001)
*15.911 (0.001)
*Values are presented as mean±standard deviation or number
FFDT: finger to floor distance test, PSLR: passive straight leg raise, VAS: visual analog scale.
a