대한밤사선의학호|지 1998; 39: 985- 992
색전술에 의한 경막 동정맥루의 치료 효과1
박광보
·서대철
·정애경
·기원우
·김성태 5
•이명준6
•최충곤
·이호규
검창진 2 • 안효숙 . 3 • 김종성 4 • 이명종4목 적 :색전술에 의한경막동정맥루의 치료효과를평가하고자한다.
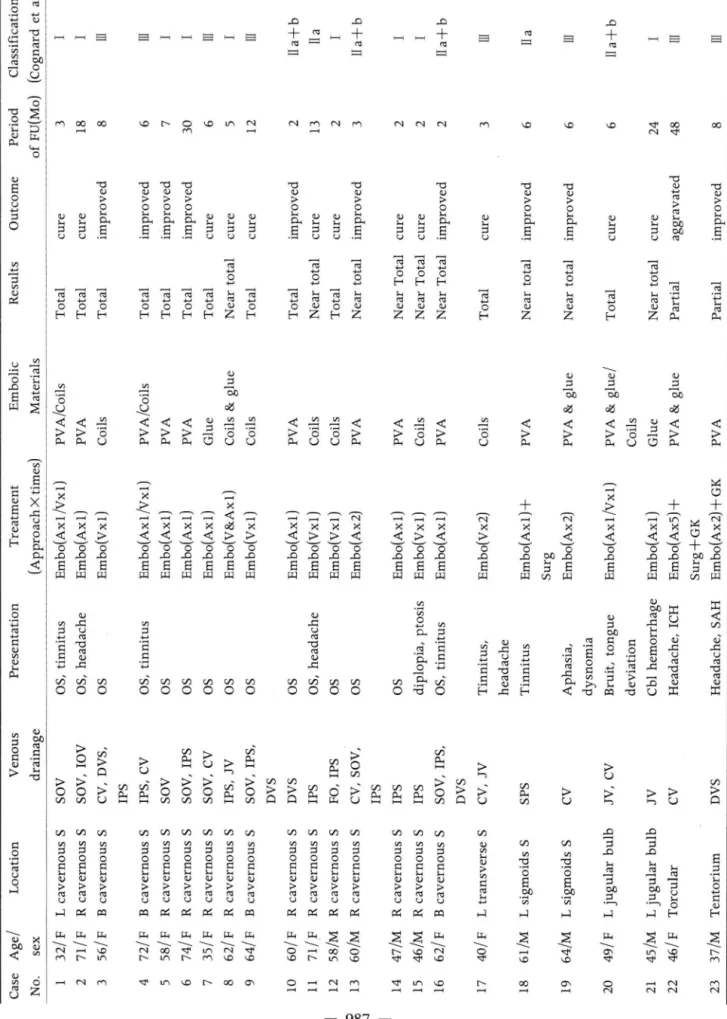
대상 및 방법 : 혈관 조영술상 경막 동정맥루가 확인되어 통,정맥을 통한 색전 치료를 받은 23명을 대상으로 하였다. 혈관 조영술에서 관찰된 경막동정맥루의 위치는 해면정맥동 16명, 경막정맥동 4명, 경정맥 팽대부 2명, 헤로펼루스동 1명, 소뇌천막부 1명이였다. 유출 정맥의 위치와 혈류 형태에 따르는 경막 동정맥의 분류는 Cognard 등의 분류를 적용하였다.
전체 23명 중 13명은 동맥 경로만을 통하여, 6명은 정맥 경로만을 통하여, 그리고 4명은 동맥과 정맥을 통하여 색전 치료하였다. 그 중 1명은 수술, 1명은 감마 방사선 치료, 그리고 l명은 수술과 감마방사선 치료를 병행하였다. 동맥을 통해 사용된 색전 물질은 polyvinyl alcohol 업자나 아교였고, 정맥을 통해 사용된 색전 물질은 tungsten코일, platinum코일이 나 Guglielmi분리 코일이었다. 치료 전과 후의 혈관조영상을 비교하여 경막동정맥루의 잔 여 병변 유무를 확인하였으며 치료후 임상 증상의 호전 유무를 2개월에서 48개월까지 추적 조사하였다. 치료결과의 판정은 완치, 호전, 무변화 및 악화로 나누었다.
결 과 : Cognard 분류법에 의한 유형에서 I 형 9명, II a형 2명, II a+b형 4명,I!I형 8명이 였다. 색전 치료후 추적검사에서 전체 23명 중 12명은 완치되었고 10명은 호전되었으며 1명 은 악화 되었다. 동맥 경로만을 통해 치료한 13명 중 4명은 완치, 8명은 호전, 1명은 악화되 였다. 정맥경로만을 통해 색전치료를 시행한 6명중 5명은 완치되고 1명은 호전되었다. 동맥 과 정맥을 통해 치료한 4명 중 3명은완치, 1 명은호전되었다. 임상증상과 경막동정맥루의 위치를 연관시켜 볼 때 헤로필루스동에서 발생한 1명의 환자는 색전 치료, 수술 및 감마 방 사선치료에도불구하고악화되었다.
결 론· 경막동정맥루는중재적 시술에 의한적절한치료시 완치나호전을기대할수있 으며, 동맥을 통한 치료보다 정맥을 통한 치료에서 더 좋은 결과를 얻었다. 헤로필루스동에 발생한 경우는 그 치료 효과가 좋지 않으므로 좀더 적극적 인 치료를 필요로 한다.
경막 동정맥루는 전체 두개강내 혈관기형의 약 10-15%를 차지하는 혈관 기형으로 알려져 있으며(1 ), 발병의 원인은 혈 전을 통반하는 정맥의 폐색 후 경막에서 잠재적 순환경로가 열 리는 데 있다고 보고있다. 경막 동정맥루는 대부분 횡행 정맥통 과 S상 정맥동에서 생기며 해면정맥통과 소뇌천막부, 시상정맥 동, 그리고 드물게는 하추체 정맥동, 대후두공에도 생긴다
(2-4). 경막 동정맥루의 임상적 발현은 병변의 위치와 유출정 맥의 형태에 따라매우다양하게 나타나묘로두통,신경학적 결 손, 출혈, 치애 등의 증상이나 증후를 나타 낼 수 있으며, 두개
l 울산대학교 의과대학 서울중앙병원 진단방사선과 2 울산대학교 의과대학 서울중앙병원 신경외과 3 울산대학교 의과대학 서울중앙병원 안과 4 울산대학교 의과대학 서울중앙병원 신경과 5언하대학교 의과대학 진단방사선과 6 국럽의료원 진단방사선과
이 논문은 1997년 12월 4일 접수하여 1998년 4월 24일에 채택되었음.
강내 출혈이나 점차 진행하는 신경학적 결손이 있는 경우 반드 시 치료를 요한다 (5). 치료방법의 결정을 위해서는 먼저 경막 동정맥루의 혈류역학적인 상태를정확히 분석하는것이 중요하 며 유업동액과 유출정맥, 두개강내 정액동의 폐색및 피질정맥 의 충만 여부 등을 파악하여야 한다. 경막 동정맥루는 Mir onov (6) 분류에서와 같이 위치에 따른 분류를 할 수도 있으나 본 연구에서는 유출정맥과 피질정맥 및 경막 정맥동과의 상호 관계를 적용한 Cognard 등 (7) 의 분류를 사용하여 경막 동정맥 루의 혈관 조영소견을 분석하였으며 그에따라 시행한 치료방법 들의 효괴플추적관찰하고혈관내 치료의 유용성을평가하고자 하였다.
짜
대상및방법
1991년부터 1997년까지 6년간 혈관조영술에 주로 사용된 기 기는 Philips Intregis BN 3000(Netherland) 이였다. 디지탈 감산 혈관조영술에서 경막 동정액루가 확인되어 방사선과에서 통,정맥을 통한 색전 치료를 받은 23명의 환자를 대상으로 하였 q(Table 1). 대상환자들의 연령은 32세 부터 74세까지 평균 55세였으며, 남자 8명, 여자 15명이었다. 발병 당시의 임상증상 은 병록지를 통해 확인하였다. 혈관조영술에서 경막동정맥루의 위치와 유출정액 그리고 피질정맥의 충만 유무를 관찰한 후 Cognard 등 (7) 의 분류법에 따라 분석하였다.
경막 동정맥루의 위치는 해변정맥동이 16명으로 가장 많았 고, 경막 정맥동 3명, 경정맥팽대부 2명, 소뇌 천막부 l명, 헤로 필루스동 1명이었다. 동맥 경로만을 통한 색전술은 13명에서 시행하였고 정맥 경로만을 통한 색전술은 6명이었으며, 동맥과 정맥 경로를 모두 이용하여 색전숭을 같이 시행한 경우는 4명 이였다. 색전술 후 감마 방사선치료를 병행한 경우가 l명, 수술
r 1
A 8
· ‘
c D
박굉보 오1: 색전술에 의한 경막 동정맥루의 치료
한 경우가 1명, 그리고 수술과 감마 방사선 치료를 모두한 경우 가 1명이었다. 동맥을 통한 색전술에는 polyvinyl alcohol 업자 (Ivalon 혹은 Contour emboli) 빛 아교 (n-butyl 2-<:yanoac- rylate : Histoacryl Blue-B. Brown, Melsungen, Germany) 를 주로 사용하였고, 정맥을 통한 색전술에는 tungsten 코일 (Balt Extrusion, Montmorency, France) 이나 platinum 코 일 (Cook, Bloomington, USA)을 주로 사용하였으며 Gugliel- ml 분리 코일 (Boston Scientific Corporation, Boston, USA) 도 1예에서 사용하였다. 아교는 Lipiodol(Laboratoire Guer- bet, Cedex, France) 과 tungsten 가루 (Balt Extrusion, Mon- tmorency, France 혹은 N ycomed S.A.Paris) 를 흔합하여 사 용하였다. 모든 환자는 색전술 후 2-48개월간 추적 관찰하였 으며, 추적 혈관조영술을 시행하여 경막 동정맥루의 혈류역학 적 상태를 관찰하였고, 치료전 혈관조영 소견과 비교하였다. 치 료 결과의 평가는 경막 동정맥루가 완전히 소실되고 주요 임상 증상이 없는 경우를 완치, 동정맥루가 일부 남아 있으나 주요 엄상 증상이 없는 경우를 호전, 임상 증상이 지속되는 경우는 무변화, 그리고 악화의 4가지로 나누였다.
Fig. 1. Transarterial glue emboliza- tion in patient 7 with dural arteriov- enous fistula involving the right cavernous sinus(Cognard type m).
A. Right external carotid arteriog- ram shows dural arteriovenous fis- tula in right cavernous sinus drain-
’ ing into superior ophthalmic and cerebellar cortical veins.
B. A selective accessory meningeal arteriogram shows that the most of the fistular flow is coming from the accessory meningeal artery
c.
Effective filling of glue cast into the lesion was performed through accessory meningeal artery.D. The external carotid arteriogram after glue embolization shows no
~;빠ur야t야he뼈le
e
밍nous fistula. This patient had tran- sient trigeminal pain in the right face after embolization.
- 986 -
모떼 mC〉}aE패떼-U〔二m@∞”ω∞”∞∞m·|@@N
Classification (Cognard et al)
Period of FU(Mo)
Outcome Results Embolic Materials I I
3 18
cure cure improved
Total Total Total
PVA/Coils PVA
Treatment (Approach X times) Embo(Axl/Vxl) Embo(Axl) Embo(Vxl)
Presentation Venous drainage
Table 1. Summary of the Results Location Age/ Case OS, tinnitus OS, headache OS
SOV SOV, IOV CV, DVS,
L cavernous S R cavernous S
sex 32/F 71/F 56/F
No. 2 m 띠 m 山
8 6 improved improved improved
Total
Coils PVA/Coils I 7 Total PVA I m 띠 I
30 6 5
cure cure
Total Near total
Total
PVA
l &
야
oe。‘ p3 p3 ιι 이U 이U
1j o o
pb [L [L
Embo(Axl!vxl) Embo(Axl) Embo(Axl) Embo(Axl) Embo(V&Axl) Embo(Vxl)
OS, tinnitus
IPS IPS, CV
B cavernous S B cavernous S OS SOV R cavernous S OS OS OS
SOV,IPS SOV,CV IPS, JV
R cavernous S R cavernous S R cavernous S
72/F 58/F 74/F 35/F 62/F 64/F
3 4 5 6 7 8 m ω
lla+b lla
12 cure
빼
mTotal Total Near total Total
2 PVA Coils 13 2 cure Coils
Embo(Axl) Embo(Vxl) Embo(Vxl) Embo(Ax2)
OS OS OS, headache OS
SOV, IPS, DVS DVS
B cavernous S R cavernous S IPS FO,IPS CV, SOV, IPS
R cavernous S R cavernous S
F
M 빼 뼈
9 10 11 12 lla+b 3 improved Near total PVA OS R cavernous S 13 I 2 2
cure cure
Near Total Near Total
PVA Coils
Embo(Axl) Embo(Vxl) Embo(Axl)
OS ·3
따
m/ ·α
뼈 m
l p
때
@IPS IPS
R cavernous S R cavernous S
세째 씨빼 샤 M
14 15 lla+b 2 improved Near Total PVA SOV, IPS, DVS
B cavernous S 16 m 띠
3 cure Total Coils Embo(Vx2) Tinnitus’ headache
CV, JV L transverse S 4O
/ F
17 lla 6 improved Near total PVA Embo(Axl)+ Surg Embo(Ax2) Tinnitus SPS L sigmoids S 61/M 18 m ω6 improved Near total PVA & glue
m싸
a m
뺑
mμ 뼈
m m ·때
P F n 안
A d E 1α
CV L sigmoids S 64/M 19 lla+b I
6 24
cure cure
Total Near total Partial
PVA & glue/ Coils Glue
Embo(Axl!vxl) Embo(Axl) Embo(Ax5)+ Surg+GK Embo(Ax2)+GK
Cbl hemorrhage Headache, ICH
JV, CV JV
L jugular bulb L jugular bulb Torcular
49/F 45/M 46/F
20 21 m 띠 m ω
48 8
aggravated improved Partial
PVA & glue PVA Headache, SAH
CV DVS Tentorium 37/M
22 23
결 과
경막 동정맥루의 공급동액은해면정맥동의 경우주로외경동맥 분지들인 중경막동맥, 천측두동맥, 내상악동맥과 내경동맥의 해면정맥동내 분지들이였고, 후두와 및 횡행 정맥동의 병변들
박광보 오1: 색전술에 의한 경막 동정맥루의 치료
에서는 후두통맥 및 상행인두동맥, 후이개동맥들이었다. Cog- nard등의 분류 (Table 2) 에 따라 분석한 결과 I 형이 9명으로 가장 많았고, II a형이 2명, II a+b형이 4명, 그리고 m형이 8명 이었다 (Table 1). 해면 정맥동에 위치한 경막 동정맥루는 16명 중 15명에서 안구의 통증이나 충혈등 안과적인 증상이 있었으 며, 1명은 충혈이나 안구돌출이 없이 복시와 안검 히수증만 있 Table 2. Two Different Classifications of Dural Arteriovenous Fistula
A
~
DClassifÏcation Djindjian et a1.
type 1 D into sinus
type I! D into sinus with ref1ux into other sinus or CV I!a
I!a+b
type III D into CV
type N D into CV with giant venous pouch type V
D = drainage, CV = cortical vein
1
i
B
E
、3
%
Cognard et a1.
D into sinus with antegrade f10w D into sinus with retrograde D retrograde D into sinus retrograde D into sinus & CV D into CV
D into CV with ectasia
D into spinal perimedullary vein
1
Fig 2 c Transvenous coil embolization in patient 9 with dural arteriovenous fistula involving both cavernous Silll페Cognard type IIl).A. Right internal carotid (posterio-an- terior view) arteriogram shows dural arteriovenous fistula draining into both carvernous sinuses.
B. Right external carotid arteriogram shows dural arteriovenous fistula also draining into deep venous system through the basal vein of Rosenthal (arrows).
C. Coil embolization was done in both cavernous sinuses through the inferior petrosal sinus
D. Right internal and E external ca- rotid arteriograms obtained after coil embolization show nearly complete obliteration of the fistula.
988
대한방사선의학회지 1998; 38: 985-992
었다 지주막하출혈이나 뇌실질내출혈 등의 두개강내 출혈이 있었던 경우는 3병으로 Cognard 분류 I 형에서 1명과 m 행에 서 2명 있였다. 그 중 환자 21( 1 행)은 경막 정맥의 폐쇄로 인 한소뇌 출혈로수술을받은깐건후에 경막동정맥루가발생한 경우였고, 환자 22( m 형)에서는 헤루필리동에 병변이 있었던 경우로 색전술 후 일시적인 증상의 호전은 있었으나 이 후 다시 악화되는 과정을 반복하다가 정 맥 압 상승에 의한 뇌출혈이 발 생하여 결국 사망하였다. 환자 23( m 형)은 지주막하 출혈이 있 었으며 동맥 경로를 통해 2번의 색전술을 시도하여 증상의 호 전은 있었으나 치료가 불완전하여 잔유 병변에 대하여 감마 방 사선 치료를 하였던 경우이다.
동맥 경로만을 통한 색전술은 13명에서 시행하였는데 이 중 다른 치료를 받지 않고 색전술만 시행한 10명 중 4명이 완치, 6 명이 호전되었다 (Fig. 1). 호전된 4명 중 3명은 약간의 증상이 남아 있었으나 일상적인 생활을 하는데 지장은 없는 정도였다.
정맥 경로만을 통해 시술한 6명 중 5명은 완치, 1명은 호전되었 으며 동맥과 정맥을 통하여 치료한 4명 중 3명은 완치, 1명은
v
AD
/ ‘-
B
E
호전되었다 (Fig. 2, 3). 악화된 1명은 경막정맥동의 Torcula 부 위에서 완전 폐색되고 피질 정맥의 충만을 보인 경우였으며 동 맥을통한색전숭을시행한후호전이 있었으나다시 수개월 후 악화되어 수술과 감나나이프를 같이 시행하였지만 결국 출혈과 뇌압상승으로 사망한 경우였다. 수솔한 l명과 감마 방사선 치 료를 시행한 1명은 호전되었으며, 수숭과 감마 방사선 치료를 병행한 l명은 악화되었다. 시술과 관련하여 24시간 이내에 유 발된 후유증이나 주요 신경학적 손상은 없었으며, 동맥 경로를 통해 색전술을 시행한 2명에서는 안변에 3차 신경통이 일시적 으로 발생하였으나 이 후 호전되어 증상은 소실되었다. 대개의 환자에서 다양한 정도의 두통을 호소하였으며 1-2주에 걸쳐 서서히 호전되면서 증상은소실되었다.
고 찰
경막 동경맥루는 임상 경과가 다양하고 치료가 어려운 병으 로 알려져 있는데, 본 연구에서는 경막 동정맥루를 색전술로 치
꺼
c
~~때i패g. 3. Tr뎌때때a값뻐nsv
in pa와t디ient 17 with du따lπra메1 arteriovenous fistula invo이lving the left transverse sinus(Cognard type rn).
A. Left external carotid arteriogram (lateral view) shows occluded trans-
?
~erse sinus at the pro~imal en? of the dural arteriovenous fistula (a large arrow) and filIing of the cortical veins in the temporal lobe(smaIl arrows).B. The left vertebral arteriogram (pos- terio-anterior view) shows muItiple feeders from the vertebral artery.
c.
Coil embolization was done through the venous approach.D. The left vertebral and E the external carotid arteriograms show complete disappearance of the fistula.
료하여 52%(1 2/23) 에서 완치되었고, 43%(1 0/23) 에서 호전 을 보이는 좋은 치료성적을 얻었으며 색전술 치료와 관련하여 사망이나 영구적인 후유증을 동반한 합병증은 없었다. 색전술 에 의한 치료는 동맥 혹은 정맥을 치료경로로 선택 할 수 있으 며 색전물질로는 Polyvinyl Alcohol 업자 (PVA) , 아교(n-bu
tyl cyano-acrylate) 및 여러 가지 코일들이 있다. 업자형 색전 물질만을 사용하여 색전치료를 시행한 경우 재개통율이 약 30
% 정도로 보고되고 있어 (8), 아교 혹은 코일 등을 병행하여 쓰 는 경우가 많다 (9 -12). 본 연구에서는 동맥경로만을 통하여 치료한 경우는 완치율이 40%(4/1이인데 비하여 정맥 경로만 을 통해 코일로 치료한 경우는 83%(5/6) 이었다. 동맥을 통한 색전술이 불완전하여 정맥을 통한 치료를 같이한 4명의 경우와 함치면 80%(8/1이의 완치율을나타내어 정맥 경로를통한치 료가 더 효과적임을 알수 있었다. Pierot 등(13) 은 해면정맥동 과 횡행정맥동 및 S상정맥동 그리고 하추체정맥동에 위치하는 경막 동정맥루는 정맥경로를 통한 색전치료가 효과적이지만 소 뇌 천막부나 대후두공에 있는 경막 동정맥루에서는 이 방법이 적절하지 못하다고 하였다. 그러나 어떠한 형태든지 간에 정맥 경로를 확보할 수만 있다면 정맥경로를 이용한 치료를 할 수는 있을것이다.
경막동정맥루는동맥과경막정맥동및 수막정맥 사이에 다 발성 교통이 생기는 질환으로 일부에서는 선천성 병변이라는 주장이 있으나 많은 경우에서 경막 정액동의 부분적 혹은 완전 한 혈전성 폐쇄로 인해 생기는 후천성 병변으로 알려져 있다
(14). Nishijima 등(15, 16) 의 보고에 의하면 경박 정맥동이 폐쇄되면 정맥성 고혈압이 뒤따르며 조직학적으로는 침범된 경 막 정액동의 벽에 경막 동정맥루가 위치하고 경막 정맥동의 벽 을 공급하는 동맥이 굵어진다고 한다. 또한 경막 정맥동의 벽에 정상적으로 존재동}는 현미경적 동정맥루가 근육성 자동조절의 일차적인 병변이 생겨 직경이 굵어지면서 병적언 발달을 보인 다는 가정도 있다(1 7). 일부 외상이나 수술의 과거력,혈관성 질 환,경구 피임약의 복용등 경막 정맥동의 혈전 발생의 전구인자 를가지는경우는있으나경막정맥동의 혈전성 폐쇄와경막동 정액루의 발생 사이의 정확한 인과관계는 불분명하다 (18) .
발생 원인에 대한 추정이 불분명한 만큼 분류도 여러 가지 방 법이 있다. 1972년 Houser 등 (14) 이 동정맥루에서 정맥 유출 의 중요성을 기술하였고, 1976년 Castaigne 등(19) 이 피질정 맥에 큰 정맥냥(large venous lake)을 동반하는 형태가 출혈 빈도가 높다는 것을 기술한 후, 1978년 Djindjian과 Merland
등 (2이은 정맥 유출 형태를 중심으로 분류하였고 정맥동으로 유업되는 경우는 증상이 양성이며 피질정맥으로 유입되는 경우 는 신경학적 증상과 출혈이 잘 일어난다고 하였 q(Table 2).
1995년 Cognard 등(7)은 Djindjian (2이의 분류를 확대시켜 정맥동으로의 역류와 피질정맥으로의 역류가 있는 형태를 세분 화하였고 척수주위정맥으로 유출되는 형태를 추가하였다.
Cognard 등 (7) 의 분류볍이 예후와 관련이 있으며 일반적으로 잘 받아들여지는 형태로 생각하여 본 연구에서 적용하였으나 본 연구에서는 해면 정액동 병변이 많아 그러한 분류가 해면 동 정맥에서 발생한 경막 동정맥루의 예후 평가에도 같이 적용될
박광보 오1: 색전술에 의한 경막 동정맥루의 치료
수 있을 지는 의문이다. 경막 동정맥루에 관해서 1985년에 기술 된 Barrow 등 (21) 의 분류가 많이 인용되고 있는데, Barrow
등 (2 1)은 14명의 환자에서 해면 정맥동루에서 경동맥과 해면정 맥동과의 사이에 고혈류의 단락이 있는 경우를 Type A, 내경 동맥의 경막 분지와 해연정맥동 사이의 경막 단락이 있는 경우 를 type B, 외경동맥의 경막 분지와 해변정맥동 사이의 경막 단락이 있는 경우를 type C, 내, 외경통맥의 경막 분지와 해면 정맥동 사이의 경막 단락이 있는 경우를 type D로분류하였다.
그러나 Type A는 경막 동정맥루와는 다른 형태의 질환이며,
그 외의 Type에서 공급 혈관의 형태를 분류한 것도 대상 환자 의 수가 적어 일반적인 분류법으로 적용하기는 어려울 것이다.
1995년 Borden 등 (22)은 경막 정맥동이나 수막 정맥 (menin- geal vein) 으로 직접 유업되는 경우, 지주막하 정맥 (subarac- hnoid vein) 으로 역류가 있는 경우, 지주막하 정맥으로만 유출 되는 경우 등으로 분류하였으나 큰 차이를 부여하지는 못하였 고, 1995년 Mironov 등 (23) 은 위치에 따라 정맥동, 해면정액 동, Galen계, 뇌기저부 및 정맥동 주위 피질정맥 등의 5형태로 나누였으며 혈전의 확인은 부위에 따라 차이가 있어서 정맥동 인 경우 72%까지 나타나지만 기저부 형태에서는 나타나지 않 는다고 하였다. 또한 1986년 Lasjaunias 등 (24) 은 191예를 분 석하여 중추신경계의 증상은정맥압상승과관련이 있으며 말초 신경증상은 동액의 허혈현상 (steal phenomenon) 에 의한다고 하였다.
동정맥루의 발생 부위별 빈도는 서양의 보고에서는 대개 횡 행 S상 정맥동에 많아 그 부위의 정맥 혈류 유출 형태에 따라 분류하고 있으나 (7) , 국내 환자를 대상으로한 본 연구에서는 해연 정맥동에서의 발생율이 70%(16/23) 로 높았다. 해면정맥 동의 동정맥루는 대개 예후가 좋은 임상 경과를 보인다고 알려 져 있으므로 국내 환자들에서는 예후가 좋은 형태가 많다고 할 수 있을 것이다. 해면 정맥동 병변이 예후가 좋은 까닭은 해면 정맥동이 피질정맥과 후두개와나 상하추체 정액및 뇌기저부를 통하여 많은정맥 혈류의 교통이 이루어지는콧이므로정맥 혈 전이나 정맥압 상승에 의한 뇌실질로의 영향이 상대적으로 적 게 나타나기 때문일 것이다. 하지만 해면정맥동의 동정맥루에 대한 충분한 엄상 경과가 밝혀져 있지 않으으로 다른 분류가 적 용되어야하지 않을까생각된다.
피질정맥의 충만은 나쁜 예후인자로 알려져 있으며 출혈의 위험도 역시 증가되며 피질 정맥을 통한 유출이 있을 경우 출혈 의 빈도는 42%에서 50%까지 보고되고 있다 (25, 26). 본 연구 에서 두개강내 출혈은 대뇌실질부 출혈, 지주막하출혈, 소뇌반 구출혈이 각각 l명씩 있었으며, 형태학적 분류로는 m 형 2명과 I 형이 1명이었다. 환자 21( 1 형)은 소뇌 혈종 제거술을 받은 후 수술 당시의 혈관조영상에서는 보이지 않았던 경막 동정맥 루가 깐건 후에 발생하였다. 환자는 적혈구 증가증 (polycytem
ia) 이 있었으며 출혈은 혈전에 의한 정맥동의 폐색에서 비롯되 었던 것으로 간주하였다.
혈관을 통한 치료의 합병증으로는 색전물질이 경막 동정맥루 의 구멍보다 원위부로 흘러갈 경우 정맥성 경색이 생길 수 있고 공급 통맥의 근위부 폐색 혹은 불완전하거나 비효과적인 공급
- 990 -
[H 한밤사선의학회지 1998; 38: 985- 992
동액의 폐색등에서는 풍부한 측부순환을 통한 공급정맥의 재집 결이 생겨 다음시술을어렵게 만들수도있으며 경막동정맥루 의 폐색에 이어 급작스런 피질정액의 충만이 오는 수가 있다.
이러한 합병증은 때로 심한 신경학적 결손을 통반할 수 있으므 로 동정맥루의 비침습적인 치료의 하나로 경동맥 압박 치료가 있다. Halbach 등 (27) 의 보고에 의하면 후두동맥의 수동적 압 박은 22% 에서 완치되고 33%에서는 호전을 보였다. 본 연구에 서 동맥 경로를 통한 치료 후 병변이 남은 일부 환자에서는 압 박 치료를 병행하였으나 그 자체의 치료효과를 정확히 평가하 기는어려웠다.
수술적 치료는 공급동액의 결찰이나 유출정맥의 결찰 그리고 경막 동정맥루의 완전 절제 및 수술 중 아교삽입 등의 기법을 쓰며 공급동맥의 결찰은 대개 수술후 측부순환 공급동맥들의 재집결이 일어나 실패동}는 수가 많으며 특히 후두와에 위치하 는 경막 동정맥루는 해부학척인 위치에 따라 결찰 자체가 어려 울 수 있다 (28-31). 유출정맥의 결찰은 경막 동정맥루를 완치 하게 iï}는 경우도 있으나 정맥압의 상승으로 인해 출혈의 위험 이 높아지는 단점이 있다. 본 연구에서 수술을 같이 시행한 1명 은 경막 동정맥루가 S자 정맥동을 침범하여 수술적 제거를 하 였으나 정맥을 통한 폐색술로도 치강} 가능한 경우라고 보여 진다. 감마 나이프로 방사선 치료를 시행한 2명중 1명(환자 22) 이 악화되었는데 경막동정맥루에 대한방사선치료는앞으로좀 더 많은 연구가 필요할 것으로 여겨진다. 환자 22의 경우 동맥 경로를 통한 반복적인 색전술을 시도하였을 때는 증상의 호전 이 있었으나 이 후 계속 악화되어 수술과 감마 나이프 치료를 하였으나 뇌압상승과 뇌출혈로 인해 사망하였다. 돌이켜보면 환자 22에서는 정맥 경로를 통하여 폐색술을 시행동}든지 막힌 정맥 경로를복원하여 뇌압상승을완화시키는치료를적극적으 로 했어야 했던 경우로 생각된다.
결론적으로경막동정맥루는중재적 시술로비교적 안전하게 치료하여 좋은 치료 효과를 얻을 수 있었으며, 중재적 시술시의 치료 경로는 동맥을 통한 치료보다 정맥을 통한 치료에서 더 좋 은 결과를 얻었다. 헤로펼루스동에서 발생한 병변과 같이 출혈 의 위험도가 높거나 신경학적 결손이 예상될 경우는 보다 적극 적 인 치료가 필요할 것이다.
참 고 문 헌
l ‘ Newton TH, Cronqvist S. lnvolvement of the dural arteries in intracranial arteriovenous malformations Radiology 1969; 93 : 1071-1078
2. Barnwell S, Halbach V, Dowd C, Higashida R, Hieshima G Dural arteriovenous fistulas in vol ving the inferior petrosal sinus: angiographic findings in six patients. AJN R 1990; 11 : 511-516
3. Kuwayama N, Akai T, Horie Y, et al. Dural arteriovenous fistulae involving the transverse sigmoid sinus and foramen magnum. Surg Neurol 1994; 41: 389-395
4. Kothbauer K, Huber P. Dural arteriovenous fistula in the falx cerebri. Neuroradiology 1994; 36: 616-618
5. Lownie SP. lntracranial dural arteriovenous fistula: endovascul- ar therapy. Neurosurg Clin N Am 1994; 5 ‘ 449-458
6. Mironov A. Classification of spontaneous dural arteriovenous fistulas with regard to their pathogenesis. Acta Radiol 1995; 36 : 582-592
7. Cognard C, Yves P, Laurent P, Anne-Laure B, et al. Cerebral dural arteriovenous fistulas: Clinical and angigraphic corre- lation with a revised c1assification of venous drainage. Radi- ology 1995; 194: 671-680
8. Nakstad P, Bakke S, Hald J. Embolization of intracranial arteriovenous malformations and fistulas with polyvinyl alcohol particles and platinum fiber coils. Neuroradiology 1992; 34 ’
348-351
9. Gobin y, Houdart E, Rogopoulos A, et al. Percutaneous
σansvenous embolization through the thrombosed sinus in transverse sinus dural fistula. AJNR 1993; 14: 1102-1105 10. Guglielmi G, Vinuela F, Duckwiler G, et al. High flow,small
hole arteriovenous fistulas: treatment with electrodetachable coils. AJNR 1995; 16: 325-328
11. Yoshimura S,Hashimoto N,Kazekawa K, et al. Embolization of dural arteriovenous fistulas with interlocking detachable coils AJNR 1995; 16 ‘ 322-324
12. Roy D, Raymond J. The role of transvenous embolization in the treatment of intracranial dural arteriovenous fistulas Neurosurgery 1997; 40: 1133-1144
13. Pierot L, Chiras J, Duykaeryts C, Jason M, Martin N. Fist띠 es
arterioveineuses durales intracraniennes et thrombophlebites intracraniennes. J Neuroradiol 1993; 20: 9-18
14. Houser 0, CampbelI J, CampbelI R, Sundt T. Arteriovenous malformation affecting the Lransverse dural venous sinus: an acquired lesion. Mayo Clinic Proc 1979; 54: 651-661
15. Nishijima M, Takaku A, Endo S, et el. Etiological evaluation of dural arteriovenous malformations of the lateral and sigmoid sin uses based on histopathological examinations. J Neurosurg 1992;76 ’ 600-606
16. Seth M, Lee H, Oneida A. et al. Reversibility of white matter changes and dementia after treatment of dural fistulas AJNR 1995; 16: 1080-1083
17. Kerber CW, Newton TH. The macro and microvasculature of the dura mater. Neuroradiology 1973; 6: 175-179
18. Urtasun F, Biondi A. Casasco A, et al. Cerebral arteriovenous fistulas: percutaneous transvenous embolization. Radiology 1996
’ 199: 209-217
19. Castaigne P, Bories J, Brunet P, et al. Les fistules arterio-veineuses meningees pures a drainage veineux cortical Rev Neurol 1976; 132: 169-181
20. Djindjian R, Merland JJ. Super-selective arteriography of the external carotid artery. Berlin; Springer-Verlag, 1978
21. Barrow DL, Spector RH. Braun IF, et al. Classification and treatment of spontaneous cavernous sinus fistulas. J Neurosurg 1985; 62: 248-256
22. Borden J, Wu J, Shucart W. Proposed c1assification for spinal and cranial dural arteriovenous fistulous maIformations and im- plication for treatment. J Neurosurg 1995; 82: 166-179
23. Mironov A. Dural arteriovenous fistula of the inferior petrosal sinus producing contralateral exophthalmus. Neuroradiolo밍 1994; 36: 619-621
24. Lasjaunias P, Chiu M, Brugge KT, Tolia A, Hurth M, Berenstein M. Neurological manifestations of intracranial dural arteriov- enous malformations. J Neurosurg 1986; 64: 724-730
25. Gaston A, Chiras J, Bourbotte G, Leger J, Et al. Meningeal arteriovenous fistulae draining into the cortical veins. J Neuro radiol 1984; ll: 161-177
26. Pierot L, Chiras J, Meder J, Rose M, et al. Dural arteriovenous
박광보 오1: 색전술에 의한 경막 동정맥루의 치료
fistulas of the posterior fossa draining into the subarachnoid 29. Sundt T, Piepgras D. The surgical approach to arteriovenous veins. AJNR 1992; 13: 315-323 malformations of the lateral and sigmoid dural sinuses J 27. Halbach V, Higashida R, Hieshima G, et al. Dural fistulas in- Neurosurg 1983; 59: 32-39
volving the transverse and sigmoid sinuses: results of treatment 30. Grisoli F, Vincetelli F, Fuchs S, et al. Surgical treatment of ten- in 28 patients. Radiology 1987; 163: 443-447 torial arteriovenous malformations draining into the subarac- 28. Halbach V, Higashida R, Hieshima G,et al. Transvenous hnoid space. J Neurosurg 1984; 60: 1059-1066
embolization of dural fistulas involving the transverse and sig- 31. Kosnik EJ, Hunt WE, Miller CA. Dural arteriovenous malforma- moid sinuses. AJN R 1989; !o : 385-392 tions. J Neurosurg 1974; 40: 322-329
J Korean Radiol Soc 1998; 39 : 985- 992
The Results of Embolization of Dural Arteriovenous Fistula
1Kwang Bo Park, M.D., Dae Chul Suh, M.D., Ae Kyeong Jeong, M.D.
Won Woo Ki, M.D., Sung Tae Kim5, Myung Joon Lee, M.D.6 Choong Gon Choi, M.D., Ho Kyu Lee, M.D., Chang Jin Kim, M.D.2 Hyosook Ahn, M.D.3, Jong Sung Kim, M.D.4, Myoung Jong Lee, M.D.4
1 Department of Diagnostic Radiology, Asan Medical Center University of Ulsan College of Medicine 2Department of Neurological Surgeηι Asan Medical Center University of Ulsan College of Medicine
3Department of Ophthalmology, Asan Medical Center University of Ulsan College of Medicine 4Departmeηt of Neurology, Asan Medical Center University of Ulsan College of Medicine
5 Department of Radiology, College of Medicine, Inha University 6 Department of Radiology, National Medical Center
Purpose: To assess the embolization effect of dural arteriovenous fistula(DA VF).
Materials and Methods: We evaluated 23 patients with DAVF who were diagnosed using digital subtraction angiography and treated by transarterial and/or transvenous emobolization. The locations of DAVFs, as seen on angiograpl).y were as follows: 16 in the cavernous sinus, four in the major dural sinuses, two in the jugular bulb, one in the torcula Herophili, and one in the tentorium cerebelli. On the basis of venous drainage patterns, Cognard’s classification of DA VF was used.
Among our 23 patients, 13 underwent transarterial embolization, six underwent transvenous embolization, and four underwent both. After embolization, three patients underwent other treat- ment: surgery, one; gamma irradiation, one; and both in one. Polyvinyl alcohol particles or glue was used in transarterial embolization, and tungsten, platinum, or Guglielmi detachable coils in transvenous embolization. To analyse the residual lesion in DAF, we compared pre- and post-treat- ment angiograms; patients were followed up for 2 to 48 months, and their condition was assessed as cured, improved, not changed, or aggravated.
Resu Its : Nine patients were found to be Cognard type 1, two were II a, four were II a
+
b, and eight were type IIl. Of our 23 patients, 12 were cured, ten improved, and one was aggravated; of the 13 who underwent transarterial embolization, four were cured, eight improved, and one was aggravated ; of the six who underwent transvenous embolization, five were cured and one improved. The condition of a patient with a lesion in the torcular herophili was aggravated despite surgery and gamma irradiation after embolization.Conclusion: DAVF can be managed successfully with endovascular treatment. The outcome of the transvenous approach appears to be better than that of the transarterial approach alone. In a case involving a lesion in the torcular herophili, the outcome was poor and more aggressive treat- ment was required.
Index words: Arteries, therapeutic blockade Fistula, arteriovenous
Fistula, carotid -ca vernous
Address reprint requests to: Dae Chul Suh, M.D., Department of Radiology Asan Þ.‘edical Center, University of U1san College of Medicine # 388-1 Poongnap-Dong, Songpa-Gu, Seoul 138-736, Korea
Tel. 82-2-224-4400 Fax. 82-2-476-4719
- 992 -