서 론
단독 비복신경 손상은 발생빈도가 그리 높지 않은 병 으로 대부분 비골이나 경골의 원위부의 골절이 있은 후 외측 발목 부위의 통증(pain, burning sensation)이 나 경련(spasm), 이상감각(paresthesia and numb- ness), 감각과민(hypersensitivity) 등의 증상이 발생 할 경우 의심해 볼 수 있는 병이다.1 또한 당뇨병과 같 은 전신 신경병증이 있을 때 비복신경은 다른 신경보다 빨리 손상을 입게 되며, 감각신경만을 가지고 있기 때 문에 진단적 목적으로 조직검사를 시행할 경우 외측 비 복신경 생검을 하게 되며, 이로 인한 손상이 생길 수
있으며, 심장 수술에 있어 비복 정맥을 획득할 때에도 수술을 하는 중에 손상을 받을 수 있는 신경이다.2 그러 나 외상으로 인한 단독 비복신경 손상은 보고된 적이 있지만 특정 이유가 없이 비외상성으로 인한 단독 비복 신경의 보고는 드물다. 이에 비외상성 단독 비복신경 손상 2예를 근전도 소견과 함께 초음파 소견을 보고하 고자 한다.
증례 1
24세 여자 환자가 6개월 전부터 발생된 좌측 발목 외 측 이상감각을 주소로 본원 신경과 외래로 내원하였다.
– 83 –
대한근전도∙전기진단의학회지 13(1):83~86, 2011 J Korean EMG Electrodiagn Med
Address reprint requests to Ha Ra Jeon, MD
Department of Rehabilitation Medication, Yonsei University Medical Center, 134 Sinchon-dong, Seodaemun-gu, Seoul 120-752, Korea
TEL: 82-2-2227-3211, FAX: 82-2-363-2795, E-mail: [email protected] 투고일: 2011년 5월 11일, 수정일: 2011년 6월 29일, 게재 확정일: 2011년 6월 29일
비외상성 단독 비복신경 손상 2예 - 증례 보고 -
국민건강보험공단 일산병원 재활의학과, 연세대학교 의과대학 세브란스병원 재활의학과�
김형섭∙김종문*∙조성래*∙전하라*
– Abstract –
Two Cases of Non-traumatic Sural Mononeuropathy Injury - 2 Case Report -
Hyoung Seop Kim, M.D., Jong Moon Kim, M.D.*, Sung-Rae Cho, M.D.*, Ha Ra Jeon, M.D.*
Department of Rehabilitation Medicine, Ilsan Hospital, National Health Insurance Coporation, Department of Rehabilitation Medication, Yonsei University College of Medicine
�Sural mononeuropathy is an uncommon disease that usually caused by trauma. However we present two cases of non-traumatic sural mononeuropathy injury each in a 24-year old female due to neuroma forma- tion and a 30-year old male patient due to inflammatory reactions. Both cases were diagnosed quantita- tively and qualitatively through electromyographic and ultrasonographic evaluations, respectfully. Both electromyographic and ultrasonographic evaluations should be considered for accurate diagnosis.
Key Words: Sural nerve, Electromyography, Ultrasonography
김형섭∙김종문∙조성래∙전하라
과거력상 특이 소견이 없으며, 내원 전에 종아리를 가 늘게 하기 위해 하지 마사지를 자주 시행하였다고 하지 만, 통증을 느낄 정도의 외상은 없었다고 한다. 이학적 검사에서는 양측 하지 근력은 정상이었으며, 하지 직거 상 검사에서 특이 소견이 관찰되지 않았고, 양측 요부 근육에서도 압통점이 발견되지 않았다. 좌측 하지의 Tinel 징후는 음성이었으나 좌측 하지의 1/3에서부터 명확한 감각이상이 나타났다.
원인 감별을 위하여, 양측 하지 근전도 검사를 시행하 였으며, 검사 결과에서 비복신경근병증으로 진단하였다 (Table 1). 이 때 근전도 검사는 보편적인 검사 방법에 따라 자극전극과 기록전극이 14 cm 떨어진 상태에서 측정되었으며, 방 온도는 34도 이상에서 시행되었다.3
병변의 국소화를 위해 시행한 자기공명영상검사에서 비복신경의 일부 신경막에 두꺼워진 것을 확인할 수 있 었으며, 초음파 검사에서도 주위 신경조직의 국소적 증 식을 확인할 수 있었다(Fig. 1, 2, 3). 말초 신경막종 (Neuroma)이 의심이 되어 조직 검사 시행을 권유하였 으나 환자의 거부로 시행하지는 못하여 조직학적 결과 는 얻지 못하였다.
증례 2
30세 남자가 3개월 전부터 발생한 좌측 발목 외측 감 각이상을 주소로 본원 재활의학과 외래로 내원하였다.
환자의 직업은 일반 직장인이었으며, 과거력상 특이 소
– 84 – Table 1. Sensory Nerve Conduction Study of the First Case
Nerve Onset latency (ms) Amplitude (mV) Lt. supeficial peroneal *3.6 *18.7 Rt. superfical peroneal *3.4 *17.0
Lt. sural *3.4 **2.9
Rt. sural *3.6 *21.1
Lt; left, Rt; right, *; normal, **; abnormal
Table 2. Sensory Nerve Conduction Study of the Second Case
Nerve Onset latency (ms) Amplitude (mV) Lt. supeficial peroneal *2.35 *21.2 Rt. superfical peroneal *2.35 *23.2
Lt. sural *2.65 **4.5
Rt. sural *2.00 *29.4
Lt; left, Rt; right, *; normal, **; abnormal
Fig. 1. (A) T2WI Axial scan shows focal thickening sural nerve (arrow) and lesser saphenous vein (arrow head). (B) T2WI Coronal scan shows focal thickening sural nerve (arrow).
A B
Fig. 2. Longitudinal ultrasound scan of left calf shows focal thickening sural nerve compared with normal right side.
견이 없었으며, 특별한 외상 병력이나 흔적도 없었다.
이학적 검사에서는 양측 하지 근력은 정상이었으며, 하 지 직거상 검사에서 특이 소견이 관찰되지 않았고, 양 측 요부근육에서도 압통점이 발견되지 않았다. 좌측 하 지의 Tinel 징후는 음성이었으나 좌측 외측 상과부터 감각이상이 나타났다.
원인 감별을 위하여 양측 하지 근전도 검사를 시행하 였으며, 검사 결과에서 비복 신경근병증으로 진단하였 다(Table 2).
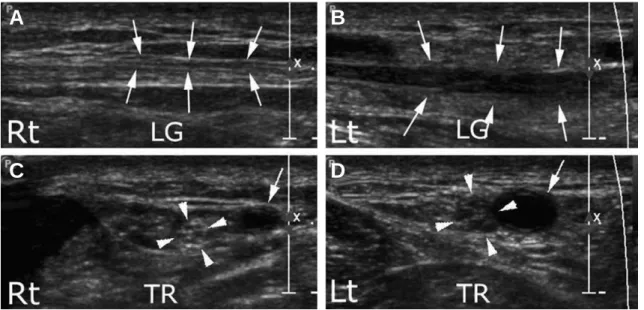
병변의 국소화를 시행한 초음파 검사에서 말초 신경 막이 두꺼워진 것은 확인할 수 없었으나, 병변 부위의 비복신경이 저음영의 부종 소견이 관찰되었으며, 횡단 스캔에서 상대적으로 소복제 정맥이 확장된 소견과 동
시에 비복신경의 직경이 증가된 소견을 확인할 수 있었 다. 그러나 증례 1에서와 같이 비복 신경을 압박하는 해부학적인 구조물은 발견할 수 없었다(Fig. 4).
고 찰
비복신경은 일반적으로 내측 비복감각신경 분지와 외 측 비복감각신경 분지의 결합으로 이루어진다고 알려져 있다. 내측 비복 감각신경은 경골신경의 분지로서 슬와 부근에서 기시하여 비복근의 두 개(medial and later- al gastrocnemius) 머리 사이로 주행하다가 하퇴 부 위에서 근막을 뚫고 피하에 위치하게 되고 외측 비복감 각신경은 총비골신경의 분지로 비복근을 싸고 있는 근
비외상성 단독 비복신경 손상 2예 - 증례 보고 -
– 85 –
Fig. 3. Transverse ultrasound scan of left calf shows focal thickening sural nerve (arrows) and lesser saphenous vein (arrow head).
Fig. 4. Longitudinal and transverse ultrasound scan of left calf compared with right side. (A) Longitudinal ultrasound scan (LG) shows right (Rt) normal lateral sural nerve (arrows). (B) Longituidnal ultrasound scan (LG) shows left (Lt) enlarged hypoechoic pathologic lateral sural nerve (arrows). (C) Transverse ultrasound scan (TR) at the lateral malleolus level shows right (Rt) normal lateral sural nerve (arrow heads), and small saphenous vein (arrow). (D) Transverse ultrasound scan (TR) at the lateral malleolus level shows left (Lt) enlarged hypoehoic pathologic lateral sural nerve (arrow heads) and enlarged small saphenous vein (arrow).
A
C D
B
김형섭∙김종문∙조성래∙전하라
막위로 주행하여 근막을 뚫고 나온 내측 비복감각신경 과 함께 비복신경을 형성하게 된다. 형성된 비복신경은 아킬레스건을 경사지게 가로질러 외측 복사골 뒤쪽으로 주행한다.4,5 따라서 비복신경의 주행상 아킬레스건의 외 측 복사골 부위에 타박상을 입었을 경우에 단독 비복신 경 손상이 일어날 가능성이 많다.6 Refaeian 등은 수 술적인 합병증으로 인한 경우를 제외한 40증례의 비복 신경병증들을 고찰한 결과 외상에 의한 경우가 27증례 로 약 2/3에 해당할 정도로 가장 많은 비중을 차지하였 으며, 혈관 이상에 의한 경우가 6증례, 비복신경 결절 종에 의한 경우가 4증례, 이유를 알 수 없는 경우가 2 증례, 베이커 낭종에 의한 경우가 1증례가 있었다고 보 고하였다.1 이밖에 Stickler 등이 2006년에 발표한 논 문에서도 36명의 환자를 대상으로 시행한 연구에서 단 독 비복손상은 외상이 가장 많았으며, 신경종과 혈관 이상에 의한 경우가 다음으로 많은 경우를 차지하였다.7 비복신경 손상이 의심될 경우, 근전도 검사를 통해 비복신경 손상을 확인할 수 있지만 원인과 위치를 파악 하기가 어려워, 추가적인 검사를 진행하여야 한다. 병 력상 아킬레스 건 부위의 타박상의 과거력이 있는 경우 에는 외상에 의한 비복신경 손상의 가능성이 가장 크겠 으나 그렇지 않은 경우, 혈관의 이상에 의한 경우나 신 경 결절종 등을 감별진단으로 포함 시킬 수 있다.8 따라 서 병력과 함께 부위를 확인하기 위해서는 초음파나 자 기공명영상이 적절한 진단 수단이 될 수 있다.
Bianchi는 말초신경의 손상을 진단하는데 있어서 초음 파와 자기공명영상을 비교하였는데, 초음파는 검사자의 판단에 의한 능동적인 검사가 가능하며, 특히 긴 신경 을 보는데 짧은 시간이 걸리며, 가격이 비교적 저렴하 며, 검사를 받는 사람의 입장에서도 보다 쉽게 검사에 응하였으며, 진단적인 목적으로 보았을 때 MRI와 비교 하여서도 떨어지지 않는 결과를 보였으며,9 Simonetti 등은 소복재정맥 수술 후 발생한 비복신경 손상 진단 증례에서 근전도 검사와 함께 초음파를 이용하였을 경 우, 근전도에서 알 수 없는 해부학적인 이상소견을 발 견할 수 있다고 발표한 바가 있다.10 이번 증례의 경우 에도 근전도 검사를 시행한 후 단순 비복신경 손상이 진단된 후 원인을 알기 위하여 증례 1의 경우에는 자기 공명영상과 초음파를 증례 2의 경우에는 초음파를 시행 하였으며, 비복신경 손상의 원인을 짐작할 수 있었다.
초음파 검사는 근전도 검사와는 달리 정량적 분석이 힘 들지만, 정성적 분석과 원인을 추정하기에 좋은 검사로 생각되며, 향후 말초 신경 병변의 국소화에 있어, 근전 도 검사와 동시에 초음파 검사를 시행할 경우 더 정확 한 진단이 가능할 것으로 판단된다. 저자들은 비외상성 원인에 의한 단독 비복신경병증이 발생한 2명의 증례를 경험하였기에 문헌 고찰과 함께 보고하는 바이다.
참고문헌
1. Refaeian M, King JC, Dumitru D: Isolated sural neuropa- thy presenting as lateral ankle pain. Am J Phys Med Reha- bil 2001: 80: 543-546.
2. Mondelli M, Reale F, Cavallaro T: Neuroma of the sural nerve as a complication of stripping of the small saphe- nous vein. Surg Neurol 1997: 48: 330-332.
3. Kimura J: Electrodiagnosis in diseases of nerve and mus- cle: principals and practice. New York: Oxford University Press, 2001, pp162-166.
4. Kim YT, Moon JS, Kim JK: Anatomical investigation of sural nerve and its contributing nerves. J Korean Acad Rehab Med 2003: 27: 723-726.
5. Moore KL, Dalley AF: Clinically oriented anatomy, 4th ed, Philadelphia: Lippincott Williams & Wilkins, 1999, pp572-601.
6. Ferkel RD, Heath DD, Guhl JF: Neurological complica- tions of ankle arthroscopy. Arthroscopy 1996: 12: 200- 208.
7. Denny DE Stickler, KN Morley, EW Massey: Sural neu- ropathy: etiology and predisposing factors. Muscle Nerve 2006: 34: 482-484.
8. Seo JH, Ryan HF, Claussen GC, Thomas TD, Oh SJ: Sen- sory neuropathy in vasculitis: a clinical, pathologic, and electrophysiologic study. Neurology 2004: 63: 874-878.
9. Bianchi S: Ultrasound of the peripheral nerves. Joint Bone Spine 2008: 75: 643-649.
10. Simonetti S, Bianchi S, Martinoli C: Neurophysiological and ultrasound findings in sural nerve lesions following stripping of the small saphenous vein. Muscle Nerve 1999:
22: 1724-1726.
– 86 –