Introduction
Squats are used to increase lower-body muscle strength, and are among the most common exercises performed by the general public and athletes (Escamilla et al, 2001; Fry et al, 2003; Mccurdy et al, 2005). Among closed kinetic chain exercises, squats
particularly activate the knee extensors and hip ex- tensors, and thus are effective for stabilizing the hip and knee joints (Earl et al, 2001; Stiene et al, 1996).
Squat exercises can vary in depth (partial squats: 40˚
knee angle, half squats: 70 to 100˚, and deep squats:
greater than 100˚), as well as in the intensity of load, foot placement and position (conventional Corresponding author: Oh-yun Kwon [email protected]
Comparison of Knee Extensor and Hip Extensor Strength According to Wall Squat Performance
Sung-hoon Jung1,2, BPT, PT, Moon-hwan Kim1,3, PhD, PT, Ui-jae Hwang1,2, BPT, PT, Jun-hee Kim1,2, BPT, PT, Oh-yun Kwon1,4,5, PhD, PT
1Kinetic Ergocise Based on Movement Analysis Laboratory
2Dept. of Physical Therapy, The Graduate School, Yonsei University
3Dept. of Rehabilitation Medicine, Wonju Severance Christian Hospital
4Dept. of Physical Therapy, College of Health Science, Yonsei University
5Dept. of Ergonomic Therapy, The Graduate School of Health and Environment, Yonsei University
Abstract
1)Background: The wall squat is considered an effective exercise because it can reduce the knee load and prevent excessive lumbar movement. However, the relationship between wall squat performance and strength of knee extensors and hip extensors remained unclear.
Objects: The purpose of this study was to compare the strengths of the knee extensors and hip extensors between groups with low and high wall squat performance.
Method: Nineteen males (low performance group: 9 subjects, high performance group: 10 subjects) participated in this study and performed wall squats. The subjects who were performing less than 30% of the average wall squat count were classified into the low wall squat performance group (less than or equal to 4 times) and the subjects who performed more than 30% of the average wall squat count were classified into the high wall squat performance group (greater than or equal to 8 times). Knee extensor and hip extensor strength were measured with a strength measurement system. An independent t-test was used to compare the strengths of the knee extensors and hip extensors between the groups with low and high wall squat performance.
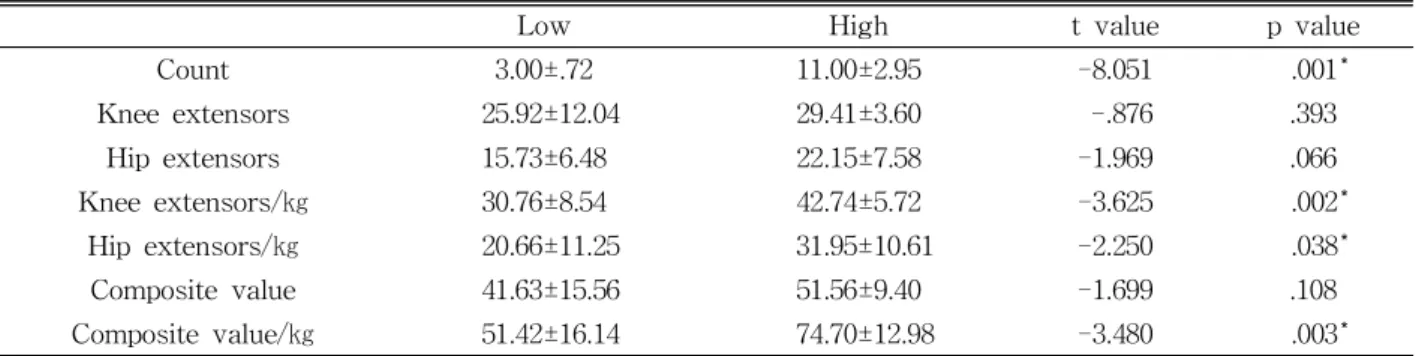
Results: The ratios of knee extensor and hip extensor strength to bodyweight were greater in the high wall squat performance group than in the low wall squat performance group (knee extensors:
p<.001; hip extensors: p=.03). In the high- and low-performance groups, the ratios of knee extensor strength to bodyweight were 42.74±5.72 and 30.76±8.54, respectively, and the ratios of hip extensor strength to bodyweight were 31.95±10.61 and 20.66±11.25, respectively.
Conclusion: Our findings suggest that knee extensor and hip extensor strength are needed for high wall squat performance. Thus, exercise to increase the knee and hip extensors strength can be recommended to improve squat performance.
Key Words: Hip extensors; Knee extensors; Strength; Wall squat performance.
squats, single-leg squats and wall squats).
The conventional squats can increase the patello- femoral compression force and stress (Escamilla et al, 2009) as well as lumbar flexion (Noyes et al, 1984; Paoli et al, 2009; Schoenfeld, 2010). They may also increase the risk of muscle ligamentous sprains, disc herniation and spondylolysis (Matsumoto et al, 2001; Vakos et al, 1994). However, wall squats can reduce these risks. Wall squat exercise involves slid- ing up and down against a wall. Because the wall squat is performed with the bodyweight on the wall, it is easy to perform this exercise as a beginner and to control the patellofemoral compression force and stress. The wall squat also has the advantage of preventing excessive lumbar flexion and extension.
Kim (2012) reported the activity of the quadriceps muscle during wall squats [vastus medialis obliquus:
87.2% of maximal voluntary isometric contraction (MVIC); rectus femoris: 52.3% of MVIC; and vastus lateralis: 89.3% of MVIC]. The average gluteus max- imus muscle activity was 17.6% of the MVIC in males and 20.4% of the MVIC in females during wall squats (Bolgla et al, 2014). In the previous study, the majority of the studies on electromyography (EMG) during walls squat were conducted. Schoenfeld (2010) reported the importance of lower extremity strength for squat ex- ercises and Kim et al (2015) reported the relationship between squat depth and lower extremity strength and range of motion. However, the relationship of wall squat performance with knee extensor and hip extensor strength remained unclear. Thus, the purpose of this study was to compare the strengths of the knee ex- tensors and hip extensors between groups with low and high wall squat performance. We hypothesized that the knee extensor and hip extensor strength would be different depending on ability of wall sqaut performace.
Methods
Subjects
32 healthy male subjects, who volunteered in this
study from among students at Yonsei University, Wonju Campus, were asked to perform wall squat as much as possible. The average wall squat count of 32 subjects was 6.9 times. In order to classify the group according to the performance of wall squat the high and low groups were classified based on completing the total average number. The subjects who were performing less than 30% (less than or equal to 4 times) of the average wall squat count were classified into the low wall squat performance group and the subjects who performed more than 30% (greater than or equal to 8 times) of the average wall squat count were classified into the high wall squat performance group. Therefore, 19 male students (low performance group: 9 subjects, high performance group: 10 sub- jects) participated in this study. Inclusion criteria in- cluded being healthy young male (20∼35 years) for homogeneity and the absence of pain in any part of the body at the time of wall squat. Exclusion criteria included the presence of pain in the back, knee and ankle region and a previous history of back, knee and ankle surgery. The mean height and weight of the subjects was 168.9±7.3 ㎝ and 66.4±14.4 ㎏, respectively.
The study was approved by the Institutional Review Board of Yonsei University (approval number: 1041849- 201603-BM-007-02).
Wall squat
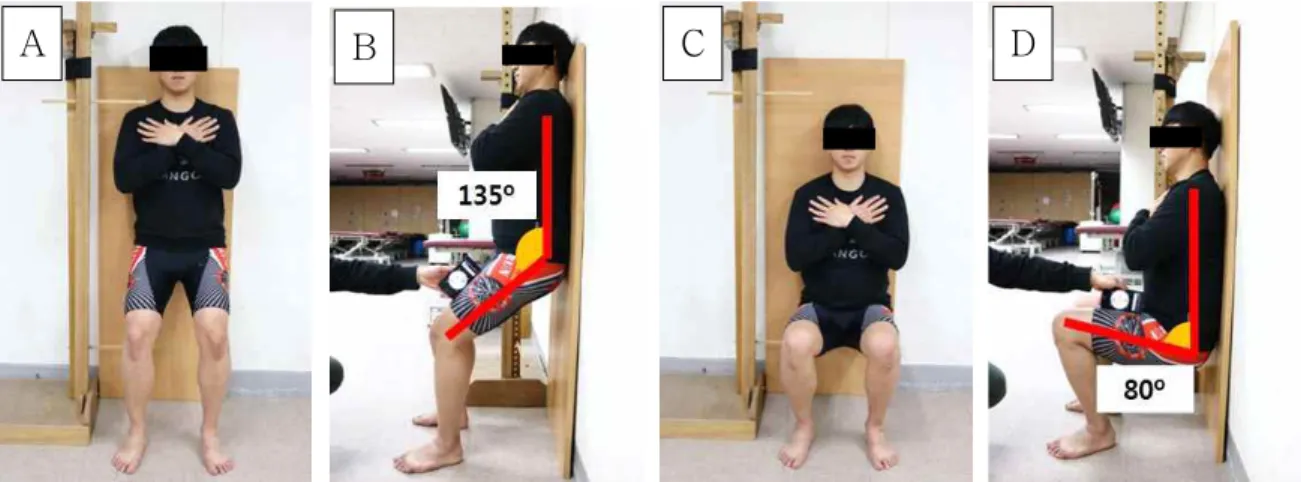
The subjects were instructed about wall squat ex- ercise and had a familiarization session of 5 minutes prior to evaluation session. For the wall squat ex- ercise, the subjects stood against a wall with their legs shoulder-width apart, with 135-degree knee flex- ion and a neutral ankle position. The pelvis and the lumbar spine were in the neutral position and the hands were crossed over the chest (Figure 1A, 1B).
The wall squat exercise used a modified Cho (2013) method to accurately control the posture and time.
During the wall squat motion, the knees were flexed to an 80-degree angle (Figure 1C, 1D) from the 135-degree starting position, without heel elevation, during a 5-second descent; the full-squat position
was held for 5 seconds; and the knees were ex- tended back to a 135-degree angle (Figure 1A) dur- ing a 5-second ascent. This was counted as one cy- cle of a wall squat. We used a mobile phone appli- cation (Clinometer level and slope finder, Plaincode Software Solutions, Stephanskirchen, Germany) to measure the start (Figure 1B) and full-squat posi- tions (Figure 1D), and placed a target bar just below the ischial tuberosity at the end position (Figure 1D).
The Metronome Beats application (Metronome Beats, Stonekick, London, England) was used to control the descent, full-squat maintenance and ascent times.
Strength measure
Knee extensor and hip extensor strength were
measured on a SMARTKEMA strength system with a load cell sensor (Relive Inc., Gimhae, Korea). For the measurement of knee extensor strength, the sub- ject was seated at the edge of the therapeutic table, with 90-degree knee flexion and 90-degree hip flexion. The subject was told to stabilize himself by holding the side of table with his hands and main- taining an upright sitting posture. A glass suction cup on the floor was attached to a restraining belt, which was tied to the subject’s ankle to limit the vertical direction of knee extension. The length of the belt was adjusted so that the subject could ex- tend the knee 45 degrees (Figure 2A). The subject performed isometric movements by extending the an- kle against the strap anchored by the glass suction
A B C D
Figure 1. Wall squat (A: initial position in frontal plane, B: initial position in sagittal plane, C: full squat position in frontal plane, D: full squat position in sagittal plane).
A B
Figure 2. Strength measure method (A: knee extensor strength measure method, B: hip extensor strength measure method).
cup and maintaining the maximum voluntary iso- metric contraction for 5 seconds.
For the measurement of hip extensor strength, the subject lay on the table in a prone position with knee flexion while his leg was slightly off the side of the table. A thigh strap was tied to the femur, 2
㎝ above the popliteal fossa. The length of the belt was adjusted so that subject’s leg would be in the position of 5-degree hip extension (Figure 2B). The examiner stabilized the rotation of the lumbar verte- bra during hip extension. The subject exerted a 5-second maximum voluntary isometric contraction twice against the strap. The mean values of the middle three seconds were averaged to generate the mean MVIC values.
Because of strength of lower extremity is influ- enced by bodyweight, the measured strength was normalized to bodyweight according to previous study (Claiborne et al, 2006) to yield the strength- to-bodyweight ratio (㎏f/㎏). And composite values that is strength of the knee extensor added strength of hip extensor were also analyzed because two muscles are working as synergists to descending for eccentric contraction and ascending for concentric contraction during the wall squat. The intra-rater reliability of the strength measurements was calcu- lated with data from two trials per subject. An in- tra-class correlation coefficient (ICC) [3,1] model and 95% confidence intervals (CI) were used to evaluate the intra-rater reliability of each strength measure- ment and strength-to-bodyweight ratio. The strength
measurement during knee extension demonstrated excellent intra-rater reliability [ICC (3,1)=.97, 95% CI:
.931, .987], and the intra-rater reliability was also good for the hip extension measurement [ICC (3,1)=.94, 95%
CI: .872, .976].
Statistical analysis
Statistical analyses were conducted with SPSS ver. 22.0 (SPSS Inc., Chicago, IL, USA). The Kolmogorov-Smirnov test was used to confirm that the data were normally distributed. An independent t-test was used to com- pare the strengths of the knee extensors and hip ex- tensors between the low and high wall squat per- formance groups. A value of p<.05 was taken to in- dicate statistical significance.
Figure 3. Knee extensor and hip extensor strengths and strength-to-bodyweight ratios (KE: knee extensor strength, KE/w: knee extensor strength-to-bodyweight ratio, HE:
hip extensor strength, HE/w: hip extensor strength-to-bodyweight ratio, Com: composite values; KE+HE, Com/w: composite value- to-bodyweight ratio; (KE+HE)/㎏, *p<.05,
**p<.001).
Low High t value p value
Count 3.00±.72 11.00±2.95 -8.051 .001*
Knee extensors 25.92±12.04 29.41±3.60 -.876 .393
Hip extensors 15.73±6.48 22.15±7.58 -1.969 .066
Knee extensors/㎏ 30.76±8.54 42.74±5.72 -3.625 .002*
Hip extensors/㎏ 20.66±11.25 31.95±10.61 -2.250 .038*
Composite value 41.63±15.56 51.56±9.40 -1.699 .108
Composite value/㎏ 51.42±16.14 74.70±12.98 -3.480 .003*
composite value: knee extensors+hip extensors, *p<.05.
Table 2. Knee extensor and hip extensor strengths and strength/bodyweight ratios
Results
Results of all outcome measures are summarized in Table 2. The ratios of knee extensor and hip ex- tensor strength to bodyweight differed significantly between the low and high wall squat performance groups (knee extensors: p<.001; hip extensors: p=.03) (Figure 3). And the ratios of composite value to bodyweight differed significantly between the low and high wall squat performance groups (p<.01). However, no significant difference was observed in the strengths of the knee extensors and hip extensors between the low and high wall squat performance groups (knee extensors: p=.39; hip extensors: p=.06).
Discussion
We investigated the differences in knee extensor and hip extensor muscle strengths between low and high wall squat performance groups. Previous studies have investigated the association between the squat 1 repetition maximum (RM) and squat performance (Bazyler et al, 2014) or studied muscle activity during wall squats (Ayotte et al, 2007; Boren et al, 2011;
Escamilla et al, 2009; Kim, 2012), but there has been insufficient research regarding the differences in muscle strengths between low and high wall squat performance groups. This study demonstrated that there was no significant difference in knee extensor or hip extensor strength between the low and high wall squat performance groups; however, the high wall squat performance group had higher body- weight-normalized knee extensor and hip extensor strengths than the low wall squat performance group.
The wall squat exercise involves descending to a full-squat position (80-degree knee flexion) and as- cending to the initial position (135-degree knee flex- ion). Previous studies (Cheron et al, 1997; Dionisio et al, 2008; Escamilla et al., 1998; Flanagan et al, 2003) have shown that quadriceps activation is high in the descending section of the squat. Kim (2012) reported
the activation of the vastus medialis obliquus (87.21%
of MVIC), rectus femoris (52.34% of MVIC) and vastus lateralis (89.37% of MVIC) during wall squats.
In the ascending section of the squat, activation of the GM was 56-86% of the MVIC (Ayotte et al, 2007).
Therefore, for successful squat performance, knee ex- tensor and a hip extensor strength will be required. In this study, the differences in the knee extensor and hip extensor strength-to-bodyweight ratios between the low and high wall squat performance groups were significant (knee extensors: p=.002, hip extensors:
p=.038). The wall squat is a closed kinetic chain ex- ercise that combines various movements, including knee extension and hip extension (Dionisio et al, 2008).
Although the individual strengths of the knee ex- tensors and hip extensors depending on weight are important, the combined strength of the two is also important for successful squat performance, because it is difficult to perform a squat successfully with only one of these strengths. Thus, composite strength val- ues that combine knee extensor and hip extensor strength should also be considered. In this study, there was a significant difference in the normalized compo- site value by weight between the two groups (p=.003).
We found no significant difference in knee ex- tensor or hip extensor strength between the low and high wall squat performance groups (knee extensors:
p=.393, hip extensors: p=.066). However, there were significant differences in the knee extensor and hip extensor strength-to-bodyweight ratios between the low and high wall squat performance groups (knee extensors: p=.002, hip extensors: p=.038). Claiborne et al (2006) also normalized strength to bodyweight.
Although the weight-bearing is less than conven- tional squat, the wall squat also was a weight-bear- ing exercise. Therefore knee extensor and hip ex- tensor strengths have limitations to explain the dif ferences in muscle strength between the low and hig h wall squat performance groups before the values are normalized by weight. Clinically, when the lower extremities are strengthened for wall squat perform- ance, exercise programs should be designed with
knee extensor and hip extensor strength normalized by weight, rather than considering only the knee ex- tensor and hip extensor strengths.
There were several limitations to the current study.
Firstly, we only considered the knee extensors and hip extensors, and did not investigate the activities of other muscles that also may have affected ankle con- trol, such as the ankle dorsiflexors and ankle plantarflexors. Secondly, we did not investigate hip, knee and ankle kinematics during the wall squats, al- though the joint angles were controlled. Future stud- ies need to be conducted to evaluate hip, knee and ankle kinematics during wall squats for the purpose of investigating asymmetrical movement. Thirdly, only healthy and relatively young subjects (21∼32 years old) were recruited for our study. Thus, our findings cannot be generalized to individuals with lumbar dys- function or to other patient populations. And this study was a cross-sectional study. Muscle strength was improved by exercise over 4 weeks, and in a study of Bazyler et al (2014), a squat exercise for 8 weeks or more was reported to improve RM.
Therefore future studies need to be evaluated to long term effects of wall squat exercise.
Conclusion
This is the first study to investigate and compare the strengths of the knee extensors and hip ex- tensors between low and high wall squat perform- ance groups. The knee extensor and hip extensor strength-to-bodyweight ratios were greater in the high wall squat performance group than in the low wall squat performance group. The results suggest that knee extensor and hip extensor strength are needed for high wall squat performance.
References
Ayotte NW, Stetts DM, Keenan G, et al. Electromyo-
graphical analysis of selected lower extremity muscles during 5 unilateral weight- bearing exercises. J Orthop Sports Phys Ther.
2007;37(2):48-55.
Bazyler CD, Sato K, Wassinger CA, et al. The effi- cacy of incorporating partial squats in maximal strength training. J Strength Cond Res.
2014;28(11):3024-3032. https://doi.org/10.1519/JSC.
0000000000000465
Boren K, Conrey C, Le Coguic J, et al.
Electromyographic analysis of gluteus medius and gluteus maximus during rehabilitation exercises.
Int J Sports Phys Ther. 2011;6(3):206-223.
Bolgla L, Cook N, Hogarth K, et al. Trunk and hip electromyographic activity during single leg squat exercises do sex differences exist? Int J Sports Phys Ther. 2014;9(6):756-764.
Cheron G, Bengoetxea A, Pozzo T, et al. Evidence of a preprogrammed deactivation of the hamstring muscles for triggering rapid changes of posture in humans. Electroencephalogr Clin Neurophysiol.
1997;105(1):58-71.
Cho M. The effects of modified wall squat exercises on average adults’ deep abdominal muscle thick- ness and lumbar stability. J Phys Ther Sci. 2013;
25(6):689-692. https://doi.org/10.1589/jpts.25.689 Dionisio VC, Almeida GL, Duarte M, et al.
Kinematic, kinetic and EMG patterns during downward squatting. J Electromyogr Kinesiol.
2008;18(1):134-143.
Earl JE, Schmitz RJ, Arnold BL. Activation of the VMO and VL during dynamic mini-squat ex- ercises with and without isometric hip adduction.
J Electromyogr Kinesiol. 2001;11(6):381-386.
Escamilla RF, Fleisig GS, Zheng N, et al.
Biomechanics of the knee during closed kinetic chain and open kinetic chain exercises. Med Sci Sports Exerc. 1998;30(4):556-569.
Escamilla RF, Fleisig GS, Zheng N, et al. Effects of technique variations on knee biomechanics dur- ing the squat and leg press. Med Sci Sports Exerc. 2001;33(9):1552-1566.
Escamilla RF, Zheng N, Macleod TD, et al.
Patellofemoral joint force and stress during the wall squat and one-leg squat. Med Sci Sports Exerc. 2009;41(4):879-888. https://doi.org/10.1249/
MSS.0b013e31818e7ead
Flanagan S, Salem GJ, Wang MY, et al. Squatting exercises in older adults: Kinematic and kinetic comparisons. Med Sci Sports Exerc. 2003;35(4):
635-643.
Fry AC, Smith JC, Schilling BK. Effect of knee po- sition on hip and knee torques during the bar- bell squat. J Strength Cond Res. 2003;17(4):
629-633.
Katoh M. Reliability of isometric knee extension muscle strength measurements made by a hand-held dy- namometer and a belt: A comparison of two types of device. J Phys Ther Sci. 2015;27(3):851-854.
https://doi.org/10.1589/jpts.27.851
Kim BJ. Comparison of Quadriceps Femoris Muscle Activations during Wall Slide Squats. J Korean Soc Phys Med. 2012;7(4):541-550.
Kim SH, Kwon OY, Park KN, et al. Lower extremity strength and the range of motion in relation to squat depth. J Hum Kinet. 2015;45:59-69.
https://doi.org/10.1515/hukin-2015-0007
Kritz M, Cronin J, Hume P. The bodyweight squat: A movement screen for the squat pattern. Strength and Conditioning Journal. 2009;31(1):76-85.
Matsumoto H, Suda Y, Otani T, et al. Roles of the anterior cruciate ligament and the medial collat- eral ligament in preventing valgus instability. J Orthop Sci. 2001;6(1):28-32.
McCurdy KW, Langford GA, Doscher MW, et al.
The effects of short-term unilateral and bilateral
lower-body resistance training on measures of strength and power. J Strength Cond Res.
2005;19(1):9-15.
Noyes FR, Butler DL, Grood ES, et al. Biomechanical analysis of human ligament grafts used in knee-ligament repairs and reconstructions. J Bone Joint Surg Am. 1984;66(3):344-352.
Paoli A, Marcolin G, Petrone N. The effect of stance width on the electromyographical activity of eight superficial thigh muscles during back squat with different bar loads. J Strength Cond Res. 2009;23(1):246-250.
Schoenfeld BJ. Squatting kinematics and kinetics and their application to exercise performance. J Strength Cond Res. 2010;24(12):3497-3506.
https://doi.org/10.1519/JSC.0b013e3181bac2d7 Stiene HA, Brosky T, Reinking MF, et al. A com-
parison of closed kinetic chain and isokinetic joint isolation exercise in patients with patellofe- moral dysfunction. J Orthop Sports Phys Ther.
1996;24(3):136-141.
Vakos JP, Nitz AJ, Threlkeld AJ, et al.
Electromyographic activity of selected trunk and hip muscles during a squat lift. Effect of vary- ing the lumbar posture. Spine (Phila Pa 1976).
1994;19(6):687-695.
This article was received January 2, 2017, was reviewed January 2, 2017, and was accepted January 31, 2017.