INTRODUCTION
The recanalization of the occluded artery is the major goal for the treatment of patients suffering from an acute ischemic stroke and related to a good clinical outcome (1). On the basis of the results of the National Institute of Neurological Disor- ders and Stroke (NINDS) trial published in 1995 (2), throm- bolytic therapy with intravenous (IV) recombinant tissue plasminogen activator (rt-PA) has been approved as a stan- dard treatment of acute ischemic stroke within 3 hours after symptom onset by the United States Food and Drug Admin-
istration (FDA). However, less than 3% of patients currently receive IV rt-PA in daily practice because of numerous con- traindications and the short treatment time window (3). More- over, it is reported that the recanalization rate after IV throm- bolysis is only 46.2% (1). Although intra-arterial thrombolysis may extend the therapeutic window to 6 hours from symp- tom onset and shows a better recanalization rate of up to 66%, the use of thrombolytics may cause symptomatic intracranial hemorrhage.
For patients with a contraindication for thrombolytics, a large artery occlusion, or a symptom onset of less than 8
J Korean Soc Radiol 2011;65(1):41-51
Received February 28, 2011; Accepted May 5, 2011 Corresponding author: Sang Joon Kim, MD Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, 86 Asanbyeongwon-gil, Songpa-gu, Seoul 138-736, Korea.
Tel. 82-2-3010-3953 Fax. 82-2-476-0090 E-mail: [email protected]
This study was supported by a grant (grant number:
2008-336) from the Asan Institute for Life Science, Seoul, Korea.
Copyrights © 2011 The Korean Society of Radiology
Index terms Stroke Ischemia
Thromboembolism Models, Animal
Thrombolytic Therapy Stents
Purpose: To evaluate the feasibility of a self-expanding stent for acute embolic oc- clusion, and recanalization mechanism by histologic examination.
Materials and Methods: Five mongrel dogs were used as study subjects. Each ver- tebral artery was occluded, and a self-expanding stent was used for recanalization.
We evaluated the technical success rate for the placement of the stent to the tar- geted vessel, the recanalization rate, and residual stenosis. We obtained two speci- mens of the stented vertebral arteries for histologic evaluation.
Results: One dog died of an unknown cause during the induction of anesthesia. In two dogs, only one side of the vertebral artery was used, whereas both vertebral arteries were used in the remaining dogs. A total of six vertebral arteries were suc- cessfully occluded. The technical success rate for stenting without complication was 66.7%. The immediate recanalization rate after stenting was 100%. The resid- ual stenosis was 35.6 ± 18.6%. On microscopic examination, the stent concentri- cally displaced the clot and the clot was captured between the stent mesh and ar- terial wall.
Conclusion: Self-expanding stents were effective in revascularizing the cerebrovas- cular embolic occlusion. The self-expanding stent seemed to achieve recanalization by pushing the clot to the arterial wall and capturing the clot between the stent mesh and arterial wall.
Mechanical Recanalization of Cerebral Artery Embolic Occlusion Using a Self-Expanding Stent: Experimental Analysis in Canine Model
1자가 팽창성 스텐트를 사용한 색전성 뇌혈관 폐쇄의 기계적 재개통:
잡견 모델에서의 실험적 평가
1Jin Woo Choi, MD
1,2, Sang Joon Kim, MD
1, Deok Hee Lee, MD
1, Dae Chul Suh, MD
11Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea
2Department of Radiology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea
and tested the feasibility, safety, and effectiveness of self-ex- panding stents for recanalization of acute occlusions resulting from radiopaque blood clots.
MATERIALS AND METHODS
Animal Preparation
All experimental procedures were conducted in accordance with the National Institute of Health guidelines for humane handling of animals and were approved by the Institutional Animal Care and Use Committee at our institute. Five male mongrel dogs weighting 24 to 25 kg were used in this study.
Anesthesia was induced in each dog with intramuscularly in- jected ketamine hydrochloride (Ketara; Yuhan coporation, Seoul, Korea) and atropine sulfate (Atrophine; Daewon Pharm Co., Ltd., Seoul, Korea), and was maintained throughout the procedures with intravenous ketamine hydrochloride. After ex- posure of the femoral artery, 8-F sheath (Terumo, Tokyo, Ja- pan) was placed in the femoral artery using a modified Seld- inger technique.
Clot Preparation
The radio-opaque clot for occlusion was prepared by mixture of autologous arterial blood (10 mL) with thrombin (Throm- bin; Reyon Pharmaceuticals, Seoul, Korea) (50 IU) and barium sulfate (Solotop; Taejun Pharm Co., Ltd., Seoul, Korea) (1 g) by modifying the clots used in previously published animal stud- ies (27, 28). The mixed blood was injected into a transparent silicone tube with a 3-mm inner diameter and 200-mm length.
To minimize the sedimentation of the barium to the dependent portion of the clotting blood, we manually rolled the tube for the first 5 minutes. The total incubation time was 60 minutes at room temperature.
Angiography and Clot Application
A baseline angiography was performed through the right femoral approach using a 4-F diagnostic catheter (Head-Hunt- er; Jeongsung Medical, Seoul, Korea). Anteroposterior and later- al projection images of both vertebral arteries were obtained by the manual injection of the contrast media, and the maximal di- ameter of the cervical vertebral arteries was measured. After a baseline angiography of the vertebral arteries, a 7-F guiding hours, various mechanical thrombolytic techniques using mi-
croguidewire, microcatheter, snare, balloon, stent, and other devices have been reported as effective treatments (5-12).
These mechanical devices and techniques can reduce the time to recanalize, decrease the required dose of adjuvant throm- bolytics, and have a superior recanalization rate compared with IV and IA thrombolysis (1). Although stents are not ap- proved by the FDA as a treatment method for acute ischemic stroke, stent insertion showed a higher recanalization rate than that of the MERCI device (Concentric Medical, Moun- tain View, CA, USA), which the FDA has approved as a me- chanical clot retrieval device for reperfusion therapy in pa- tients suffering an acute ischemic stroke (10-16). Stent placement for an acute intracranial arterial occlusion using balloon-expandable coronary stents or self-expanding stents seems to be effective in revascularizing occluded arteries (10, 12, 14, 17-20). Recently, there have been several studies em- ploying stents to treat acute occlusions of cerebral vessels;
they showed high recanalization rates (67.5-92%) of occluded cerebral arteries in a limited number of case series or case re- ports (18-21). Although the self-expanding stent has lower outward radial force compared with the balloon expandable stent, these studies used self-expanding stents to revascularize occluded cerebral arteries. Its lower profile and higher flexi- bility ease tracking into the small intracranial target arteries (17-26). In spite of its low outward radial force, the self-ex- panding stent appears to revascularize occluded arteries by compressing the clot to the inner wall of the parent arteries.
However, the exact mechanism of the recanalization is un- clear, and there remains a concern about the fragmentation and distal migration of the clot during the stent placement, which could cause occlusion of the significant perforators or cortical branches. To investigate the mechanism of the self- expanding stent for recanalizing cerebral artery occlusion and to evaluate the occurrence of fragmentation and distal migra- tion, an animal study is essential. An animal study is also in- dicated to eliminate the effects of other factors such as the concomitant use of the thrombolytics or mechanical devices in the recanalization of the acute occlusion, which are almost inevitable in clinical practice.
In this study, we developed an embolic cerebrovascular oc- clusion model in mongrel dogs using radiopaque blood clots,
monitor the respiration status and cardiac motion of the dogs for one hour. The technical success of the stent deployment was defined as the safe placement of the stent at the site of the occluded vessel with full coverage of the lesion without frag- mentation and distal embolization of the clot. Fragmentation and distal migration were defined as the dislocation of any part of the radiopaque clot and embolization to a previously unaffected vessel induced by microguidewire, microcatheter, contrast injection, or stent deployment as observed on fluoro- scopic examination. A one-hour selective angiogram after stent placement was performed and used for evaluating the rate of recanalization, immediate stenosis rate after stent place- ment, and fragmentation and distal migration of the clot. Suc- cessful recanalization was defined as achieving an Arterial Occlusive Lesion (AOL) recanalization score of II or III as ob- served in Interventional Management of Stroke Trials (29, 30).
The stenosis rate after stent insertion was calculated by divid- ing the diameter of the opened segment of occluded vessel af- ter stenting by the diameter of distal normal vertebral artery.
Histologic Examination
All animals were euthanized with an overdose of zylazine hydrochloride (Rompun; Bayer Schering Pharma, Seoul, Ko- rea). In two dogs, we harvested the stented vertebral artery for microscopic examination. Under fluoroscopic guidance, we identified the stented segment of both vertebral arteries and surgically harvested the stented vessels. The arteries were cleared and perfused with 10% neutral buffered formalin at physiologic pressure. After fixation for 24 h, the specimens were embedded in methyl methacrylate (Polyscience Inc., Warrington, FL, USA) and cut into serial sections for hema- toxylin and eosin staining. Sections (40-50 μm) were photo- graphed under a light microscope (BX51, Olympus Optical Co., Tokyo, Japan). Two independent observers performed histologic analyses of the intimal injury and evaluated the re- lationship between the stent and the clot (S.J.K., J.W.C).
RESULTS
Occlusion of the Vertebral Artery by Endovascular Methods
One dog died of unknown cause during the induction of catheter (Guider soft-tip; Boston Scientific, Fremont, USA) was
placed at the cervical vertebral artery under road-map guidance.
The clot was cut into 20 mm in length before application, and rinsed with normal saline. After loading the clot and saline in the syringe, we injected the clot through the catheter. When we pushed the plunger of the syringe, the radio-opaque clot emitted through the nozzle of the syringe by conforming its diameter to the inner diameter of the nozzle of the syringe. Occlusion of the vessel was documented by digital subtraction angiography (DSA) immediately after clot application. Continuous flushing with heparinized normal saline was performed. After 1 hour, we checked the location, fragmentation, or other unpredictable changes to the clot, as well as the occlusion of the vessel by an angiogram with or without DSA.
Stent Placement
After confirming that the occluded vertebral artery by the ra- dio-opaque clot did not spontaneously recanalize through a fol- low-up selective angiogram in one hour, a stent was deployed in the occluded segment. Systemic anticoagulation was achieved by administering a single bolus loading dose (80 IU per kg) of heparin before stent insertion; no anti-platelet agent was used. A 0.014-inch exchange microguidewire (Transcend 14; Boston Scientific Corporation, Fremont, USA) was passed through the occluded segment and maintained distal to the occluded seg- ment by radio-opaque clot. We passed the microdelivery cathe- ter through the clot over the microguidewire and deployed a self-expanding stent, 4.5 × 20 mm in size (Neuroform 3; Boston Scientific Coporation, Fremont, USA). To achieve recanaliza- tion, we intended to cover the whole length of the clot with the stent. Owing to the barium mixed in the clot, the whole length of the radio-opaque clot was visible under fluoroscopic exami- nation and we tried to place the undeployed stent to cover the whole length of the radio-opaque clot. Before stent deployment, we paid special attention to whether the distal and proximal ends of the radio-opaque clot were between the distal and proxi- mal radio-opaque markers of the stent.
Outcome Assessment
Immediately after stent placement, we performed a selec- tive vertebral angiogram to evaluate the recanalization of the stented segment of the occluded vertebral artery and carefully
between a vertebral artery and small side branches. The mean length of the occluded segment of each vertebral artery, as measured by the mean length of the radio-opaque clot, was 11.9 mm (11.9 ± 2.0 mm).
Stent Placement and Outcome
Although one distal migration of the stent occurred during deployment, which resulted in an incomplete coverage of the proximal end of the radio-opaque clot by the stent, antegrade flow with an AOL score of 2 was achieved immediately after stent placement in all cases (Fig. 1). Fragmentation and distal embolization of the radio-opaque clot while passing a micro- guidewire through the occluded segment was observed in one vertebral artery (17%) (Fig. 2). Therefore, we achieved a 66.7% technical success rate (4 of 6 lesions). On follow-up an- sedation with ketamine hydrochrolide. In the remaining dogs,
we successfully inserted an 8-F sheath through the right femo- ral route. All of the vertebral arteries were successfully catheter- ized with a 4-F diagnostic catheter. All right vertebral arteries originated from the right subclavian arteries and the opposing arteries originated from the left subclavian arteries. The mean maximal diameter of the vertebral arteries was 3.4 mm (3.4 ± 0.37 mm).
Six vertebral arteries were successfully occluded in four dogs. One vertebral artery was used in two dogs and both vertebral arteries were sequentially used in the other two dogs. All six vertebral arteries were occluded with a radio- opaque clot using an endovascular method. Two clots were wedged at the point where the diameter of arterial lumen was less than that of the clot, and the four clots were anchored in
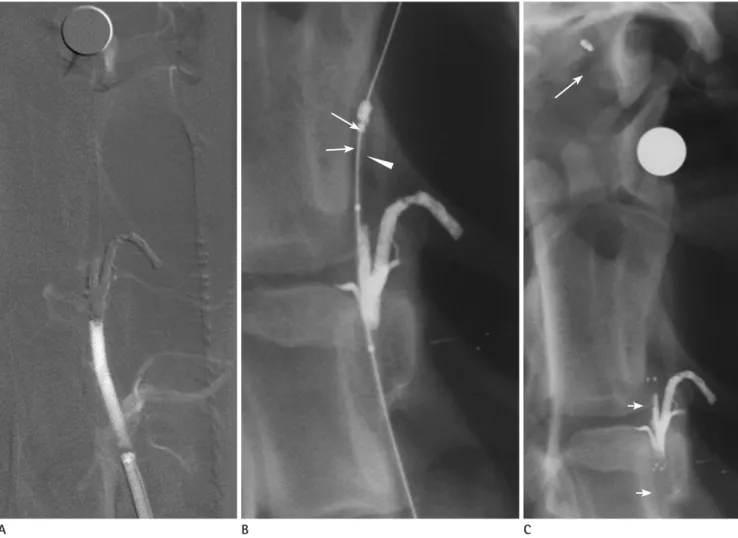
Fig. 1. A baseline anteroposterior (AP) view of a left vertebral arteriogram using digital subtraction angiography (DSA) shows normal blood flow and anatomy (A).
After the radio-opaque clot (arrows) was successfully delivered into the cervical segment of left vertebral artery (B), the AP view of the left verte- bral arteriogram using DSA shows the complete occlusion of the cervical segment of left vertebral artery by the clot (C).
AP view without DSA shows the self-expanding stent (arrow heads) completely covering the clot (D).
A follow-up angiogram shows flow with an AOL score of 2 through the stented segment of the left vertebral artery (E).
Note.-AOL = Arterial Occlusive Lesion
A B C D E
DISCUSSION
In this experimental study, we evaluated the feasibility and effectiveness of the self-expanding stent for the treatment of acute embolic occlusions. Additionally, we tried to investigate the mechanism of the recanalization in acute cerebral embolic occlusions treated by a self-expanding stent by histologic exam- ination. Our study revealed a 66.7% technical success rate for placing a self-expanding stent in the occluded vessels and a 100% recanalization rate. On microscopic examination, the clot was pushed concentrically to the arterial wall by the stent, and the clot was captured between the stent mesh and arterial wall.
For our experiment, we used vertebral arteries of Mongrel dogs. We decided to use vertebral arteries for simulating the embolic occlusion for two reasons. First, it was easy to access giograms an hour later, we could not observe further frag-
mentation and distal embolization of the radio-opaque clot or changes of the AOL score; the recanalization rate was 100%.
The residual stenosis after stent placement was 35.6 ± 18.6%
and the results are summarized in Table 1.
Microscopic Examination
We could obtain only two specimens of the stented verte- bral arteries in two dogs, because the stented vertebral arter- ies were ruined in the process of the sawing and cutting of the vertebral column and transverse process. On microscopic ex- amination, the stent was placed at the center of the radio- opaque clot, thus capturing the clot. We observed some areas of clot protrusion through the pore of the stent and areas of the denuded intima (Fig. 3).
Fig. 2. Left vertebral angiogram using DSA shows complete occlusion of the artery (A).
During the passage of the microdelivery catheter (arrowhead) over the microguidewire, fragmentation of the clot occurred (long arrows) (B).
Although the stent (short arrows) is placed successfully to cover the whole length of the clot, distal migration of the fragmented clot (large ar- row) is observed at distal branch (C).
A B C
model using an endovascular method on pigs and dogs (23, 27, 28, 31-34). It is difficult to evaluate burden of the clot at a specific artery with non-radio-opaque clot, which might criti- cally affect the recanalization rate of thrombolysis. Using a ra- dio-opaque clot, we could exactly evaluate the location and length of the clot with real-time fluoroscopic evaluation dur- ing the interventional procedure. Moreover, it was possible to see movement, fragmentation, and distal migration of the clot during the interventional procedure, which was helpful to analogize the recanalizing mechanism of the stent for embolic to the vertebral arteries using 7F guiding due to their straight
course. Second, in our pilot study, we found the mean diame- ter of the vertebral arteries to be 3.3 mm, which is similar to the intracranial distal internal carotid artery in humans. We used radio-opaque clots for vessel occlusion. We believe visu- alization of the artificial clot is very important in the case of the experimental studies with mechanical thrombolysis. A non-radio-opaque clot has previously been used for occlud- ing the arteries to evaluate the efficacy of systemic thromboly- sis and previous studies evaluated a site-specific occlusion
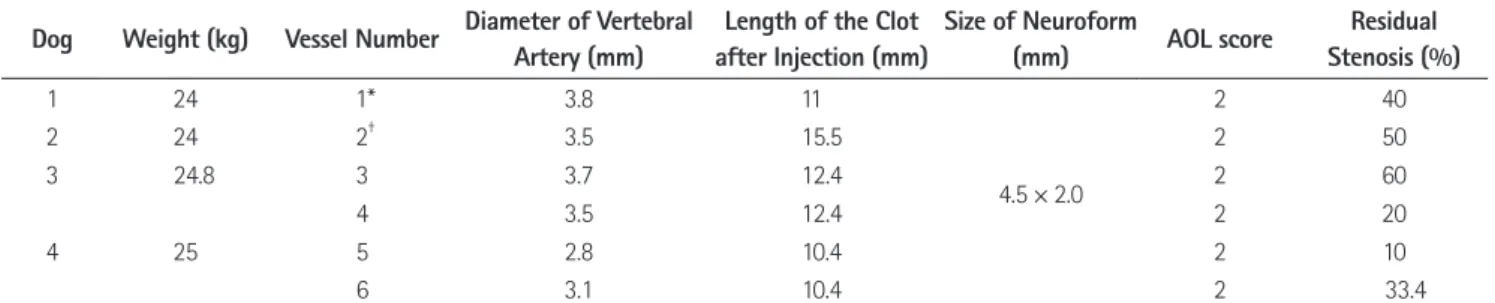
Table 1. Baseline Characteristics of the Dogs, Length of the Occluded Vertebral Arteries, Size of the Neuroform, and Revascularization after Stenting
Dog Weight (kg) Vessel Number Diameter of Vertebral Artery (mm)
Length of the Clot after Injection (mm)
Size of Neuroform
(mm) AOL score Residual
Stenosis (%)
1 24 1* 3.8 11
4.5 × 2.0
2 40
2 24 2† 3.5 15.5 2 50
3 24.8 3 3.7 12.4 2 60
4 3.5 12.4 2 20
4 25 5 2.8 10.4 2 10
6 3.1 10.4 2 33.4
Note.-*One distal migration of the stent occurred during the deployment, which resulted in the incomplete coverage of the proximal end of the radio- opaque clot by the stent.
†During the passage of the microdelivery catheter over the microguidewire, fragmentation of the clot occurred.
AOL = Arterial Occlusive Lesion
Fig. 3. A microscopic image (× 40) of the distal end of a stented segment of the right vertebral artery of the fourth dog shows good apposition of the stent strut to the arterial wall. Two areas of the denuded intima (open arrows) are noted and compared with intact intima (A).
A microscopic image (× 40) of the stented segment of the occlusion by clot shows the capture of the clot between the stent strut and arterial wall (B). However, one strut cannot appose to the clot completely (short arrow) and the protruded portion of clot though the wide stent mesh (long arrows) is seen.
A B
into the occluded vessel. The repeated introduction of the MERCI retrieval device into the clot and the corresponding vessel results in occurrence of vascular complications such as vasospasms, dissections, and clot fragmentation with distal embolization, could increase. Moreover, indirectly compared with the recanalization rate of the MERCI retriever approved by FDA due to its high recanalization rate, the recanalization rate of stenting with or without angioplasty showed better re- canalization rates up to 79% (10, 12, 13, 15, 16, 39). However, the large profile of the stent makes it difficult to navigate small and tortuous intracranial artery and impossible to reach an occluded segment. The other weak point of the balloon-ex- pandable stent is the lack of further adjustment of the diame- ter after the stent is deployed.
A Neuroform is a self-expanding stent, originally designed for assisting the coiling of a broad-neck aneurysm (22). The advantage of this self-expanding stent over a balloon-expand- able stent is its smaller profile and the adjustment of the di- ameter to the vascular lumen. Although the outward radial force of the self-expanding stent is lower than that of the bal- loon-expandable stent, from the result of some case reports in patients with thromboembolic cerebrovascular occlusion, the radial force of the self-expanding stent seems to be sufficient to recanalize embolic occlusions (17-20, 23). For these rea- sons, self-expanding stents have been increasingly used for treatment of acute cerebrovascular occlusions. Levy et al. (23) demonstrated that the self-expanding stent is equally effective with the balloon-expandable stent for recanalizing acute cere- brovascular occlusions using a canine model. In clinical stud- ies using the self-expanding stent for revascularization of the cerebrovascular occlusion, the recanalization rate was up to 92% (19, 20). However, the results from the limited number of experimental and clinical studies are not sufficient enough to continue treatment of an acute cerebrovascular occlusion using self-expanding stents. Moreover, the direct effect of the self-expanding stent to revascularize occluded artery was not easily analogized due to adjuvant treatments such as IV, IA thrombolytics, MERCI retriever, or angioplasty in previous studies (19, 20). Our study supports the previously reported data that the self-expanding stent can be an alternative option for patients with acute embolic occlusions. An immediate res- toration of the blood flow after deploying of the self-expand- occlusion.
On the basis of the result of the NINDS trial that reported administration of rt-PA in acute ischemic stroke, which im- proved clinical outcome at three months, IV rt-PA has be- come a standard treatment for acute ischemic stroke (2).
However, researchers have reported that the recanalization rate after IV thrombolysis remains at 46.2% (1). For patients with a contraindication for thrombolytics, large artery occlu- sion, or a symptom onset of less than 8 hours, various me- chanical thrombolytic techniques using a microguidewire, microcatheter, snare, balloon, stent, and other devices have been used (5, 6, 8-12, 16, 35). These methods can reduce time to recanalization and reduce the necessary dose of adjuvant thrombolytics and seem to have superior recanalization rates compared with IV and IA thrombolysis (1). With microcathe- ter or microguidewire, either a simple mechanical clot pene- tration or an aggressive mechanical clot disruption was per- formed. However, although, these techniques proved to be effective in recanalizing occluded vessels, the mechanism of recanalization is mechanical crushing of the clot into small pieces. Therewith, for mechanical crushing, there is a poten- tial risk of distal embolization, which may produce a small cortical artery occlusion and subsequent infarctions.
MERCI (Concentric Medical, Mountain View, CA, USA) was designed to revascularize intracranial vessel occlusion by removing the clot from the vessel and have it approved by the FDA for treatment of acute ischemic stroke within 8 hours of symptom onset (11, 13, 15, 16, 36, 37). However, the recanali- zation rate was only 43-54% with the retriever alone and 64- 69% with the retriever plus IA rt-PA in the MERCI phase I and Multi-MERCI trials (13, 15, 16). Recently, the Penumbra sys- tem (Penumbra Inc., Alameda, CA, USA), neuroembolectomy devices specifically designed to remove thrombus, showed promising initial results (36). The Penumbra system was able to revascularize the primary occlusion arteries in > 80% of patients, which was higher than those reported for the MER- CI device (36, 37).
Stent placement for acute intracranial arterial occlusion us- ing balloon-expandable coronary stents seems to be effective in revascularizing occluded arteries (7, 10, 12, 38, 39). Com- pared with the MERCI retrieval device, primary stenting did not necessarily require repeated introduction of the device
pushing the clot to the arterial wall, despite the lower radial force of the self-expanding stent. Moreover, clot fragmenta- tion and distal migration can be reduced by the careful ma- nipulation of the microguidewire and microcatheter.
Our study has several limitations. First, there is a possibility that the recanalization rate of our study could have been modified because of the nature of the clot. We added barium and thrombin into the whole blood to make a radio-opaque clot. The physical and chemical properties of the radio-opaque clot compared to natural clot, however, are not clearly known yet and the results of our experiment could be over- or under- estimated. Second, we do not have follow-up results for re- canalization. Because the dogs were sacrificed immediately after a 1-hour follow-up angiography to harvest the vessels, we could not observe the fate of the residual clot trapped in the stent. We focused on the feasibility and recanalization mechanism of the stent for an acute embolic occlusion, and we did not intend to obtain a follow-up angiogram in several days. Although, it may not be to predict whether the residual clot would increase in size and eventually occlude the vessel, or decrease and dissolve it completely, we think that the re- canalized lumen will remain open for 1 or 2 days if it is open 1 hour after the procedure as in our series. In the clinical set- ting, a low dose of thrombolytics and antiplatelets can be used to prevent reocclusion and enhance thrombolysis of residual clot. Finally, in this study, we only simulated an embolic stroke and therefore, cannot generalize our results to the all of the patients with cerebrovascular occlusions. In Asian and His- panic populations, intracranial atherosclerotic stenosis is more common (40), and the use of the self-expandable stent in cases of atherosclerotic occlusion is questionable for recan- alizing an occlusion.
The decision between using a self-expanding stent and a balloon-expandable stent should be made on the basis of sev- eral facts. First, a review of an initial angiogram that is fo- cused on the shape of the occlusion end; one with an abrupt cut-off of the lumen might be considered as an embolic occlu- sion, and the other with a tapered end as observed for athero- sclerotic occlusions. Finally, due to the limited movement of the microguidewire during the passage of the occluded seg- ment, the degree of difficulty passing the lesion, and the dis- tribution pattern of the very small amount of contrast agent ing stent, with an AOL score of 2, was achieved in all cases.
With regard to the mechanical thrombolysis or stent inser- tion, there is a concern about fragmentation and distal migra- tion of the clot during the procedure. In our second case, we experienced fragmentation and distal migration of the clot when we crossed the clot with a microdelivery catheter over the 0.014 microguidewire, which had been placed through the clot. From this case, we assumed that the insertion of the microdelivery catheter over the microguidewire through the clot was the most critical step for successful recanalization.
Subsequently, we manipulated the microcatheter very careful- ly so as not to disrupt the clot during the passage of the mi- crocatheter. During or immediately after stent deployment, we did not have any clot fragmentation or distal migration.
There had been no report about the morphologic changes of clot during or after stent insertion and about the recanali- zation mechanism. On the microscopic examination in our study, the stent was placed at the center of the clot and cap- tured the clot by pushing it to the arterial wall. In one recent animal study, the authors observed that the microguidewire passed between the vessel wall and thrombus and never pene- trated the clot (34). They suggested that the risk of permanent perforator occlusion could be reduced by controlling the po- sition of the microguidewire to the ipsilateral side of branch- ing vessels, because the stent located in the ipsilateral side of the branching vessel could push the clot to the contralateral side of branching or perforating vessels. However, in our study, the stent was located in the center of the clot on micro- scopic examination. It was not always possible to assume the location of the microguidewire related to an invisible clot in the clinical field and one should always weigh the importance of distal perfusion of occluded vessel against sacrificing an important side branch or perforator. We also observed that certain portions of the clot protruded into arterial lumen through the stent mesh of the open-cell design stent. Theoret- ically, the projecting portion of the clot through the strut of the stent might be fragmented and cause distal embolization.
However, there was no distal embolization of the fragmented radio-opaque clot after the self-expanding stent was success- fully placed. On the basis of microscopic examination and re- al-time fluoroscopic examination of the radio-opaque clot in our study, we postulated that recanalization was achieved by
5. Ueda T, Sakaki S, Nochide I, Kumon Y, Kohno K, Ohta S.
Angioplasty after intra-arterial thrombolysis for acute oc- clusion of intracranial arteries. Stroke 1998;29:2568-2574 6. Nakano S, Iseda T, Yoneyama T, Kawano H, Wakisaka S. Di- rect percutaneous transluminal angioplasty for acute mid- dle cerebral artery trunk occlusion: an alternative option to intra-arterial thrombolysis. Stroke 2002;33:2872-2876 7. Spreer J, Els T, Hetzel A, Arnold S, Klisch J, Huppertz HJ, et
al. Primary stenting as emergency therapy in acute basilar artery occlusion. Neuroradiology 2002;44:791-795 8. Martinez H, Zoarski GH, Obuchowski AM, Stallmayer MJ,
Papangelou A, Airan-Javia S. Mechanical thrombectomy of the internal carotid artery and middle cerebral arteries for acute stroke by using the retriever device. AJNR Am J Neuroradiol 2004;25:1812-1815
9. Noser EA, Shaltoni HM, Hall CE, Alexandrov AV, Garami Z, Cacayorin ED, et al. Aggressive mechanical clot disruption:
a safe adjunct to thrombolytic therapy in acute stroke?
Stroke 2005;36:292-296
10. Levy EI, Ecker RD, Horowitz MB, Gupta R, Hanel RA, Sau- vageau E, et al. Stent-assisted intracranial recanalization for acute stroke: early results. Neurosurgery 2006;58:458- 463; discussion 458-463
11. Smith WS. Safety of mechanical thrombectomy and intra- venous tissue plasminogen activator in acute ischemic stroke. Results of the multi Mechanical Embolus Removal in Cerebral Ischemia (MERCI) trial, part I. AJNR Am J Neu- roradiol 2006;27:1177-1182
12. Choi JW, Kim JK, Choi BS, Kim JH, Hwang HJ, Kim JS, et al.
Adjuvant revascularization of intracranial artery occlusion with angioplasty and/or stenting. Neuroradiology 2009;51:
33-43
13. Smith WS, Sung G, Starkman S, Saver JL, Kidwell CS, Gobin YP, et al. Safety and efficacy of mechanical embo- lectomy in acute ischemic stroke: results of the MERCI tri- al. Stroke 2005;36:1432-1438
14. Eberhardt O, Naegele T, Raygrotzki S, Weller M, Ernemann U. Stenting of vertebrobasilar arteries in symptomatic ath- erosclerotic disease and acute occlusion: case series and review of the literature. J Vasc Surg 2006;43:1145-1154 15. Flint AC, Duckwiler GR, Budzik RF, Liebeskind DS, Smith
WS; MERCI and Multi MERCI Writing Committee. Me- injected at the lesion site through the microcatheter, may all
additionally help in differentiating an embolic occlusion from an atherosclerotic occlusion.
Although the self-expanding stent seemed to be effective and feasible to recanalizing an embolic occlusion of the cere- bral vessels, it should not be considered as a first-line endo- vascular treatment in patients with an acute stroke. Basically, a stent is a foreign body and insertion of a foreign body under thrombogenic conditions may potentially induce further clot formation and the stent insertion necessitates the extended usage of the antithrombotic agent after recovery. Therefore, recanalization with a self-expanding stent for an embolic oc- clusion, should be considered as a rescue treatment after fail- ing to revascularize the occluded artery using intra-arterial thrombolytics or embolectomy devices.
In conclusion, a self-expanding stent was effective for re- vascularizing cerebrovascular embolic occlusions. Fragmenta- tion with distal embolization of the clot may happen during the microcatheter passage and could be avoided by careful manipulation of the devices. Recanalization of the occluded ar- tery was achieved by pushing the clot to the arterial wall and the clots were captured between the stent mesh and arterial wall. Further investigation in clinical and experimental studies is warranted to approve label use of the self-expanding stent for the treatment of acute ischemic stroke in selected patients.
REFERENCES
1. Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a meta-analysis. Stroke 2007;38:967-973 2. Tissue plasminogen activator for acute ischemic stroke.
The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med 1995;333:
1581-1587
3. Molina CA, Saver JL. Extending reperfusion therapy for acute ischemic stroke: emerging pharmacological, mechani- cal, and imaging strategies. Stroke 2005;36:2311-2320 4. Furlan A, Higashida R, Wechsler L, Gent M, Rowley H, Kase
C, et al. Intra-arterial prourokinase for acute ischemic stroke. The PROACT II study: a randomized controlled trial.
Prolyse in Acute Cerebral Thromboembolism. JAMA 1999;
282:2003-2011
nial stenoses using the Neuroform stent system: initial ex- perience in five cases. Neuroradiology 2006;48:479-485 27. Gralla J, Schroth G, Remonda L, Fleischmann A, Fandino J,
Slotboom J, et al. A dedicated animal model for mechani- cal thrombectomy in acute stroke. AJNR Am J Neuroradiol 2006;27:1357-1361
28. Gralla J, Burkhardt M, Schroth G, El-Koussy M, Reinert M, Nedeltchev K, et al. Occlusion length is a crucial determi- nant of efficiency and complication rate in thrombectomy for acute ischemic stroke. AJNR Am J Neuroradiol 2008;
29:247-252
29. Tomsick T, Broderick J, Carrozella J, Khatri P, Hill M, Palesch Y, et al. Revascularization results in the Interventional Man- agement of Stroke II trial. AJNR Am J Neuroradiol 2008;29:
582-587
30. Khatri P, Neff J, Broderick JP, Khoury JC, Carrozzella J, Tomsick T; IMS-I Investigators. Revascularization end points in stroke interventional trials: recanalization versus reperfusion in IMS-I. Stroke 2005;36:2400-2403
31. Kaufman HH, Anderson JH, Huchton JD, Woo J. A new ca- nine model of proximal internal carotid embolism. Stroke 1979;10:415-418
32. Qureshi AI, Boulos AS, Hanel RA, Suri MF, Yahia AM, Alberi- co RA, et al. Randomized comparison of intra-arterial and intravenous thrombolysis in a canine model of acute basilar artery thrombosis. Neuroradiology 2004;46:988-995 33. Ringer AJ, Guterman LR, Hopkins LN. Site-specific throm-
boembolism: a novel animal model for stroke. AJNR Am J Neuroradiol 2004;25:329-332
34. Brekenfeld C, Tinguely P, Schroth G, Arnold M, El-Koussy M, Nedeltchev K, et al. Percutaneous transluminal angioplasty and stent placement in acute vessel occlusion: evaluation of new methods for interventional stroke treatment. AJNR Am J Neuroradiol 2009;30:1165-1172
35. Suh DC, Sung KB, Cho YS, Choi CG, Lee HK, Lee JH, et al.
Transluminal angioplasty for middle cerebral artery stenosis in patients with acute ischemic stroke. AJNR Am J Neurora- diol 1999;20:553-558
36. Penumbra Pivotal Stroke Trial Investigators. The penumbra pivotal stroke trial: safety and effectiveness of a new genera- tion of mechanical devices for clot removal in intracranial large vessel occlusive disease. Stroke 2009;40:2761-2768 chanical thrombectomy of intracranial internal carotid
occlusion: pooled results of the MERCI and Multi MERCI Part I trials. Stroke 2007;38:1274-1280
16. Gobin YP, Starkman S, Duckwiler GR, Grobelny T, Kidwell CS, Jahan R, et al. MERCI 1: a phase 1 study of Mechanical Embolus Removal in Cerebral Ischemia. Stroke 2004;35:
2848-2854
17. Fitzsimmons BF, Becske T, Nelson PK. Rapid stent-support- ed revascularization in acute ischemic stroke. AJNR Am J Neuroradiol 2006;27:1132-1134
18. Sauvageau E, Levy EI. Self-expanding stent-assisted mid- dle cerebral artery recanalization: technical note. Neuro- radiology 2006;48:405-408
19. Levy EI, Mehta R, Gupta R, Hanel RA, Chamczuk AJ, Fiorel- la D, et al. Self-expanding stents for recanalization of acute cerebrovascular occlusions. AJNR Am J Neuroradiol 2007;28:816-822
20. Brekenfeld C, Schroth G, Mattle HP, Do DD, Remonda L, Mordasini P, et al. Stent placement in acute cerebral ar- tery occlusion: use of a self-expandable intracranial stent for acute stroke treatment. Stroke 2009;40:847-852 21. Kelly ME, Furlan AJ, Fiorella D. Recanalization of an acute
middle cerebral artery occlusion using a self-expanding, reconstrainable, intracranial microstent as a temporary endovascular bypass. Stroke 2008;39:1770-1773
22. Howington JU, Hanel RA, Harrigan MR, Levy EI, Guterman LR, Hopkins LN. The Neuroform stent, the first microcath- eter-delivered stent for use in the intracranial circulation.
Neurosurgery 2004;54:2-5
23. Levy EI, Sauvageau E, Hanel RA, Parikh R, Hopkins LN.
Self-expanding versus balloon-mounted stents for vessel recanalization following embolic occlusion in the canine model: technical feasibility study. AJNR Am J Neuroradiol 2006;27:2069-2072
24. Turk AS, Niemann DB, Ahmed A, Aagaard-Kienitz B. Use of self-expanding stents in distal small cerebral vessels. AJNR Am J Neuroradiol 2007;28:533-536
25. Chiam PT, Samuelson RM, Mocco J, Hanel RA, Siddiqui AH, Hopkins LN, et al. Navigability trumps all: stenting of acute middle cerebral artery occlusions with a new self-expand- able stent. AJNR Am J Neuroradiol 2008;29:1956-1958 26. Hähnel S, Ringleb P, Hartmann M. Treatment of intracra-
39. Tsumoto T, Terada T, Tsuura M, Ryujin Y, Matsumoto H, Ma- suo O, et al. Endovascular therapy for acute thrombotic oc- clusion of the intracranial artery. Neuroradiology 2004;46:
453-458
40. Suh DC, Lee SH, Kim KR, Park ST, Lim SM, Kim SJ, et al.
Pattern of atherosclerotic carotid stenosis in Korean pa- tients with stroke: different involvement of intracranial versus extracranial vessels. AJNR Am J Neuroradiol 2003;
24:239-244 37. Grunwald IQ, Walter S, Papanagiotou P, Krick C, Hartmann
K, Dautermann A, et al. Revascularization in acute isch- aemic stroke using the penumbra system: the first single center experience. Eur J Neurol 2009;16:1210-1216 38. Mori T, Kazita K, Chokyu K, Mima T, Mori K. Short-term
arteriographic and clinical outcome after cerebral angio- plasty and stenting for intracranial vertebrobasilar and carotid atherosclerotic occlusive disease. AJNR Am J Neu- roradiol 2000;21:249-254
자가 팽창성 스텐트를 사용한 색전성 뇌혈관 폐쇄의 기계적 재개통:
잡견 모델에서의 실험적 평가
1최진우1,2
·
김상준1·
이덕희1·
서대철1목적: 자가 팽창성 스텐트가 효과적으로 뇌동맥 폐쇄를 재개통시킬 수 있는가와 조직학적 관찰을 통하여 재개통의 기전 을 알아보고자 하였다.
대상과 방법: 다섯 마리의 잡견에서 색전성 척추 동맥 폐쇄 모델을 만든 후, 폐쇄된 동맥에 스텐트를 삽입하였다. 스텐트 설치의 기술적인 성공 여부를 분석하였으며 스텐트 삽입 후 폐쇄된 부위의 재관류 여부를 분석하고 남아 있는 협착의 정도 를 계산하였다. 두 마리의 잡견에 대하여 부검을 시행하였다.
결과: 한 마리의 잡견은 마취 도중 사망하였다. 두 마리 한개의 척추 동맥을, 나머지 두 마리는 양측의 척추 동맥에 대하여 차례로 폐쇄를 시행하여 6개의 척추 동맥을 폐쇄하였다. 스텐트 설치시 1예에서 혈전을 미세 유도카테터가 지나갈 때 혈전 의 부서짐과 원위부 전위가 관찰되었고, 한 예에서 스텐트가 원위로 이동하여 혈전의 근위부를 스텐트가 완전하게 덮지 못 하여 기술적인 성공은 66.7%였으며 모든 예에서 100%의 재개통률을 보였다. 남아 있는 협착은 35.6 ± 18.6%였다. 조직 학적으로 혈전의 중앙에 스텐트가 있었으며 혈전은 스트럿과 혈관 벽 사이에 끼어 있었다.
결론: 인공적으로 유발된 척추 동맥 폐쇄에서 자가 팽창성 스텐트의 삽입은 높은 재관류율을 나타내었다. 혈전에 스텐트를 삽입하였을 때 스텐트는 혈전을 혈관 벽으로 밀어서 혈류를 재개통시키는 것으로 생각한다.
1울산대학교 의과대학 서울아산병원 영상의학과학교실, 2건국대학교 의학전문대학원 건국대학교병원 영상의학과학교실