Introduction
Since the implant was first introduced in the dental academy in 1960, a variety of implant systems have been invented. Each system has been constantly developed with the changes in the design or surface treatment of an implant in order to obtain better osseointegration and therapeutic results [1,2].
The implant that was used mainly for completely edentulous patients is currently used for the partial edentulous restoration, and it is currently accepted as a sufficiently-predictable procedure
compared to the conventional fixed prosthesis due to the long- term success rate and stability [3]. Among them, the single implant is one of the most frequently performed procedures.
Compared with the conventional prosthesis, the single implant does not require the deletion of healthy adjacent teeth and allows for easier prosthesis restoration with a better teeth formation. Also, it is more beneficial in terms of oral health;
thus, it has the advantage of reducing the risk of proximal dental caries or root treatment [4]. In addition, it has economic efficiency and particularly it is said to be recommended with sufficient bone [5].
In recent years, various researches have reported a high success rate of single implants. Gotfredsen [6] reported the implant survival rate of 100% in the 5-year research and Rossi et al. [7] reported the survival rate of 95% for the period of two years. However, those researches had limitations that the
A retrospective study of treatment outcomes of single implants in the most posterior area of the jaw in Koreans: 3-10 year follow-up
Seong-Ryong Huh
1, Hwa-Sun Lee
1, Chae-Heon Chung
2, Sang-Joun Yu
1, Byung-Ock Kim
1,*
Departments of
1Periodontology and
2Prosthodontics, School of Dentistry, Chosun University, Gwangju, Korea
ABSTRACT
Purpose: This study was conducted to investigate the long-term outcomes of single implants placed in the most posterior areas of the jaw in Koreans.
Materials and Methods: A total of 169 Korean patients who received implants at the Chosun University Dental Hospital (Gwangju, Korea) were enrolled in this retrospective study. Demographic data and individual implant data were recorded.
During the follow-up period, cumulative survival rates and mean marginal bone loss were calculated by standard X-rays taken at the first visit and the last follow-up. Statistical analyses were then performed on the patient-based and implant-based analysis (IBM SPSS Statistics ver. 20).
Results: All patients (total 169; 117 male and 52 female; 37 male smokers) were eligible for the study. Among the 184 inserted implants, 51 were placed in the maxilla and 20 were installed after sinus floor elevation. During follow-up (mean 4.86 years), four implants in four patients failed, giving a cumulative survival rate of 97.9%. The mean marginal bone loss calculated from standard X-ray was 1.53±0.62 mm. No patient or implant-based factor showed significant relationship between survival rates.
Conclusion: A reliable survival rate and normal range of marginal bone loss for the single implants in the most posterior areas was achieved after 3 to 10 years.
Key Words: Alveolar bone loss, Dental implants, Molar, Restrospective studies, Single-tooth, Survival rate
Received Sep 2, 2015; Revised version received Sep 2, 2015 Accepted Sep 18, 2015
Corresponding author: Byung-Ock Kim
Department of Periodontology, School of Dentistry, Chosun University, 303 Pilmun-daero, Dong-gu, Gwangju 61452, Korea Tel: 82-62-220-3854, Fax: 82-62-224-4664
E-mail: [email protected]
implant sites were not distinguished or the follow-up period was short less than 5 years.
In general, posterior teeth receive stronger bite force than anterior teeth; therefore, it has been known that a single implant for posterior teeth area is very likely to generate problems such as screw loosening, marginal bone loss and implant fracture [2].
Moreover, it is known to have a lower success rate than anterior teeth [8]. Therefore, there are some researches indicating that a single implant for posterior teeth area with strong bite force is not recommended [9], and Mayer et al. [10] has also proposed that it be connected with other implants in order to compensate for these shortcomings.
Still, many researches are required for the long-term observational results of a single implant installed in the most posterior area. Also, there are no reports on the survival rate of single implants in posterior area in Korean population who intake more rigid food than other population. Thus, this study is aimed to analyze the long-term results of a single implant installed in the most posterior area in Korean population through the retrospective study.
Materials and Methods
Paient selection
From the period of January 2001 to December 2009, following criteria was applied to the patients who had installed a single implant in the most posterior area at the Department of Periodontology, Chosun University Dental Hospital. All of the patients reviewed were Korean. The following patient groups were included in the experimental group: (1) the patients of 18 years old and above, (2) the patients whose hindmost posterior area were edentulous, (3) the patients who were granted the healing period of at least 8 weeks after tooth extraction, (4) the patients who had performed a prosthesis procedure 3 to 6 months after installing an implant, (5) the patients with systemic good health. The patient with general condition such as pregnant, diabetes mellitus, acquired immune deficiency syndrome and patient with long-term medication of immunosuppressant or steroid were excluded. However, we didn’t exclude the patient who have smoking habit.
Treatment protocol
The included patients were followed by similar treatment
protocol, which set in the manual of Chosun University Dental Hospital for implant treatment. They were treated by same clinicians throughout the treatment period. The surgical operator (professor, a chief of department of implant center, Chosun University Dental Hospital, 56 years old male who have clinical career over 30 years) had installed the implants and also other clinician (professor, a chief of department of prosthodontics, Chosun University Dental Hospital, 63 years old male who have clinical career over 30 years) had performed the prosthetic procedures.
For implant planning, cone-beam computed tomography (CBCT) using radiographic stent was taken. From the CBCT images, need for the surgical procedures (sinus elevation or guided bone regeneration [GBR]) was determined by the operator and the system of implant (company, length, and diameter) was selected by both clinicians. When pre-surgical preparation is done, the patients who had limited alveolar bone had treated with bone augmentation surgery and the implant installation was performed after 4 to 5 months-healing. The patient with proper alveolar bone could have implant installation surgery immediately. Throughout the surgical procedure, implant stability was recorded by resonance frequency analysis (RFA). After healing period (6 months for maxilla and 3-4 month for mandible), the second surgery was done and the stability of implant was re-evaluated by RFA and radiographic examination. If the implant was determined to be stable enough, the prosthetic treatment was started. The impression coping was engaged and an open tray impression was made with silicon impression material. The fabricated prosthesis was try-in and the occlusal and proximal contacts were evaluated with carbon paper. After 2 week follow-up, the prosthesis was finally set.
After finishing implant treatment, the patient was informed to visit 3 month follow-up at first year, and 6 month follow-up after 1 year. The radiographic examination was done every 1 year and in every case of suspicious inflammation around implant.
Research method
This research was conducted by the retrospective research method using the patients’ electronic medical records and the already taken radiographs after acquiring an approval of the Clinical Ethics Committee at Chosun University (IRB Number:
CDMDIRB-1217-83).
Definition of survival and failure of implant
Gender, age, smoking habit, implant site, diameter and length of installed implant, company name, augmentation performance status and implant failure status were investigated through the electronic medical records. To compare the stability of the treatment, the survival rate was determined for the evaluation value. The survival of the implants was determined by the same criteria applied to Buser et al. [11] and Cochran et al. [12].
(a) There should be no clinical agitation of implants.
(b) There should be no subjective pain or discomfort of patients.
(c) There should be no infection around the implants.
(d) There should be no continuous radiolucency around the implants.
As for the failure of the implants, elimination of implants, observation of excessive agitation or severe bone loss, severe infection around the implant and implant fracture were considered a failure.
Evaluation on marginal bone loss
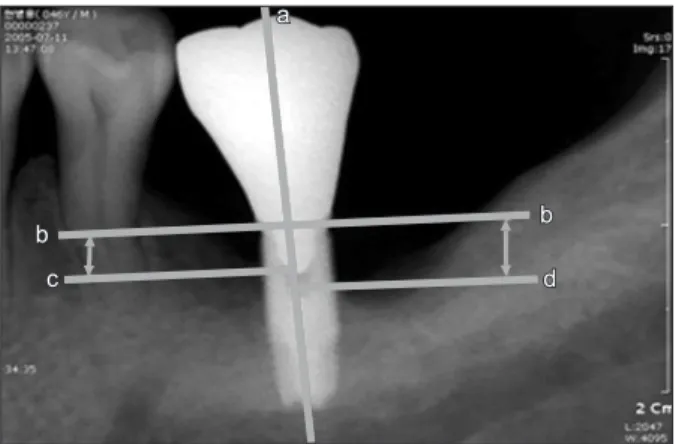
To evaluate the marginal bone loss around the implants, the standard X-rays were taken at the time of installation of the implants and at that of the most recent follow-up visit and the X-rays were taken by using paralleling cone technique. The 4 reference lines were drawn on the X-rays. The line a was the line passes the midline of the implant which is parallel to the long axis and the line b was the perpendicular line to the line a at the shoulder of implants. The line c and d were lines pass the most coronal level of bone-to-implant contact on the mesial and the distal site of implant, respectively. The distance between line b to c and line b to d was analyzed by using measurement program (PiViewStar 5.0.9.2; Infinitt, Seoul, Korea) (Fig. 1).
The measurement was conducted using the fixed magnification rate (200%) in the fixed resolution screen (1,280×720) in order to minimize the error. The mean value of the measurements at mesial and distal side was calculated.
Statistical analysis
The collected data was analyzed by using IBM SPSS Statistics ver. 20 (IBM Co., Armonk, NY, USA). The statistical analysis was performed in two categories, the patient-based and the implant-based analysis. Among the patient based
analysis, the effect of gender and smoking habit on survival rate was compiled with Fisher’s exact test. Also, the age data was evaluated with Linear-by-linear association to reveal the significance. In the implant-based analysis, the surgical procedure data was analyzed statistically with intragroup and intergroup. The significance level was p<0.05.
Results
Gender and age distribution and smoking habit of the patient
A total of 169 Korean patients were included in the present research. There were 117 men and 52 women; the number of male patients was about two times larger than that of female patients. As for the age distribution, the most common age groups were 50s, 40s and 60s in order. As for the follow-up period, the most common period was less than 4 years and the total average follow-up period was 4.86 years. There were 37 male patients who still smoke at the time of implant surgery.
The former smokers were assumed to be non-smoker. By Fisher’s exact test, the effect of gender and smoking habit on survival rate was evaluated and the result was no significant (p=1.000 and p=0.228, each). The age increasing did not significantly increase the risk of implant failure (by linear-by- linear association analysis, p=0.484).
a a
b b c
c dd
b b
Fig. 1. Reference points for the measurements of marginal bone
level. Following is the reference lines: line a Implant longitudinal
axis; line b Implant shoulder line: vertical line to a, and at the most
coronal level of the implant shoulder; line c the most coronal level of
bone-to-implant contact at the mesial site: a vertical line to a; line d
the same as c at the distal site.
Distribution for each implant site
A total of 184 single implants were installed at the most posterior area. And of those, 51 were installed in the maxilla and 133 were installed in the mandible. Approximately 2.5 times more implants were installed in the mandible than in the maxilla and approximately 5 times more implants were installed in the second molar teeth area on the left side of mandible, which had the most number of implants, than in the second posterior teeth area on the left and right sides of maxillary, which had the least number of implants (Table 1).
Distribution for each manufacturer
A s for the distribution of manufacturers sorted in the order of frequency among the 184 implants, the implants of 3i (OSSEOTITE
®or NANOTITE
®, BIOMET; Implant Innovations Inc., Palm Beach Gardens, FL, USA) accounted for 81 and Osstem (TSIISA
®; OSSTEMIMPLANT, Seoul, Korea) for 26 and ITI (ITI
®; InstituteStraumann, Basel, Switzerland) for 19 followed subsequently. There were 4 other implant systems (40 implants). The manufacturers having less than 2 implants installed were classified as ‘other’.
Diameter and length of installed implants
The most commonly installed implant had the diameter between 5 mm to 6 mm and the length between 11 mm to 12 mm (data not shown). 78.8 % of the implants was distributed in standard implant level (diameter: 4 to 6 mm, length: 10 to 12 mm).
Survival rate of the implant overtime
As for the hindmost molar single implants, 4 implants were eliminated from the 4 patients during the follow-up periods. The cumulative survival rate was 97.9%. Of the 4 failed implants, 2 were eliminated within 4 years after the installation and another was eliminated at the fourth year and another was eliminated at the eighth year additionally (Fig.
2). The cumulative survival rate and interval survival rate was calculated and at 8 to 9 year follow-up period showed highest decrease in survival rate. However, there was no statistical difference between interval survival rates. The failed implants will be analyzed in detail.
Survival rate of the implant according to the additional bone augmentation for implant installation
The cases where the maxillary sinus augmentation and the bone regeneration were performed were stated (Table 2). The maxillary sinus augmentation was performed in the 20 single implants among the total of 51 single implants installed in the maxilla, and of these, 18 cases were performed by the crestal approach while 2 cases were performed by the lateral open Table 1. Distribution of the Implants According to the Location
Variable Left Right
1st molar 2nd molar 1st molar 2nd molar Maxilla (n=51)
Mandible (n=133) 16 15
11 44
13 20
11 54
Fig. 2. Survival rate of implants in most posterior area during follow-up periods
101 100 99 98 97 96 95 94 93
Survival rate (%)
92
>10
<4 4-5 5-6 6-7 7-8 8-9 9-10
Interval survival rate Cumulative survival rate
98.9 98.9
99.2 98.3
100 98.3
100 98.3
100 98.3
95 97.9
100 97.9
100 97.9 Survival rate of implant in most posterior area
during follow-up periods
(years)
approach. The GBR procedure was performed in the total of 22 single implants. The 2 implants that were installed along with the crestal approach were eliminated; thereby, achieving the survival rate of 88.8%. Of those single implants being installed with the GBR procedure, 1 single implant was eliminated;
thereby, achieving the survival rate of 95.4%. And in the lateral open approach, the elimination of an implant has not been observed. Thus, it achieved the survival rate of 92.8% in the case of accompanying an additional augmentation technique.
However, these difference were proved to have no significance when analyzed by Fisher’s exact test. In detail, neither sinus elevation procedure nor GBR had no relationship with survival rate (p=0.598) and also the cases with additional bone augmentation didn’t have lower survival rate than the cases with proper native bone (p=0.552).
Marginal bone loss around implants overtime
The average marginal bone loss between the time of implant installation and the recent follow up visit by calculating the distance from reference lines on standard X-ray film was investigated (Fig. 1). The total bone loss quantity around the implants classified per their follow-up periods (Fig. 3).
The group with less than 4 years follow-up after the implant installation showed 1.08±0.55 mm bone loss and the group with more than 10-year follow-up showed 2.27±0.78 mm bone loss.
The mean marginal bone loss of studied implants was 1.53±0.62 mm from the initial bone-to-implant contact level. Compared to the success criteria that presented before, all of the data were within normal range of bone reaction around implant.
Analysis on failure cases
For the retrospective study, the causes of failure were investigated with reference to the electronic medical records (Table 3). During the follow-up periods, 4 implants out of the total of 4 patients were failed. Three implants from men and 1 implant from women were failed and one failure from each quadrant was observed. Looking at the pattern of the implants failure, 1 implant (5.0×10 mm, no. 1 patient) failed before loading, and 3 implants (4.0×10 mm, 5.0×10 mm, and 5.0×13.0 mm) failed after bearing the load. Particularly, the implant of
Table 2. Type of Bone Augmentation Procedures for Implant Instal- lation
Surgical procedure No. of implant
Survival rate (%) Placement with sinus floor elevation
simultaneously Crestal approach Lateral approach
Placement with GBR simultaneously Total
20
18 2 22 42
90.0
88.8 100
95.4 92.8 GBR: guided bone regeneration.
Table 3. Analysis of Failed Implants Patient
No. Gender Age
(yr) Site Implant diameter
Implant
length Time of failure Cause of failure Implant system
Augmentation procedures 1
2 3 4
Male Female Male Male
52 73 46 57
#16
#26
#46
#37 5.0 4.0 5.0 5.0
10.0 10.0 10.0 13.0
11 months after surgery 12 months after loading 8 years 4 months after loading 3 years 2 months after loading
Fixture mobility Fixture mobility Fixture mobility Peri-implant infection Severe pain
3i 3i 3i 3i
SFE: Crestal SFE: Crestal
- GBR
SFE: sinus floor elevation, GBR: guided bone regeneration.
Fig. 3. Mean marginal bone loss of implant in most posterior area during follow-up period.
3.0
2.5
2.0
1.5
1.0
Marginalboneloss(mm) 0.5
0.0
>10
<4 4 5- 5 6- 6 7- 7 8- 8 9- 9 10- Cumulative bone loss Mean m of implant in most posterior
area during follow-up periods arginal bone loss
Follou up interval (year)-