Received: May 3, 2011 / Accepted: June 7, 2011 Address for correspondence: Joong-Yang Cho, MD, PhD
Department of Neurology, Ilsan Paik Hospital, College of Medicine, Inje University, 2240 Daewha-dong, Ilsan-gu, Goyang-si, Gyeonggi-do 411-706, Korea
Tel: +82-31-910-7995, Fax: +82-31-910-7368, E-mail: [email protected]
* 본 논문은 2009년도 인제대학교 학술연구조성비 보조에 의한 것임.
근위축성측삭경화증의 전반적 관리
인제대학교 의과대학 일산백병원 신경과
조 중 양
Management of Amyotrophic Lateral Sclerosis
Joong-Yang Cho, MD, PhD
Department of Neurology, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea
KEYWORDS Amyotrophic lateral
sclerosis, Management
Amyotrophic lateral sclerosis (ALS) is a relatively rare neurodegenerative disorder and a steadily progressive disease resulting in death on average within 3 years. Approximately 20% of patients survive more than 5 years and 10% of patients more than 10 years. Although this disease is completely incurable, it is not untreatable. The mainstay of clinical management includes pharmacologic management of symptoms, management of dysphagia and respiratory symptoms, palliative care, and multidisciplinary care clinics. Currently, the management of ALS is essentially symptoms-based, and riluzole is the only drug for the treatment of ALS approved by the FDA, but with only modest increase in survival. Here, current practice in the management of ALS will be reviewed.
서 론
근위축성측삭경화증 (amyotrophic lateral sclerosis; ALS)은 뇌의 운동피질에 있는 상부 운동 신경원과 뇌간에 위치한 하부 운동 신경원의 선택적인 사멸을 특징으로 하는 신경 퇴행성 질환이다. 발병기전에 관해서는 여러 가지 가설들 이 있으나, 아직 정확하게 밝혀져 있는 것은 없으며 ALS 환 자의 90% 가 산발적 ALS이며 나머지 10%의 환자가 가족성 ALS 로 알려져 있고, 가족성 ALS의 약 20% 환자들이 Cu/Zn superoxide dismutase (SOD1)의 과오 돌연변이(missense muta- tion)에 의한 독성 기능의 획득(gain of function)을 통해 발생 한다고 알려져 있다. 질병자체가 파괴적이며 비참한 결과
를 초래하는 질환으로 진단뿐 아니라 치료에도 많은 어려 움이 있다 . 현재, ALS의 완치나 예방을 가능하게 하는 뚜렷 한 치료법이 없는 상태에서 질병을 변화(disease-modifying) 시킬 수 있는 치료와 삶의 질을 높일 수 있는 방법들에 대 한 관심이 점점 높아져 가고 있다 . 본고에서는 현재 시행되 고 있는 약물 치료를 포함한 ALS의 전반적인 관리에 대해 서 알아보고자 한다 .
본 론
ALS 치료는 과거 10여년 동안 급속하게 변화되어 왔다.
1999년 진료지침이 AAN (American Academy of Neurology)
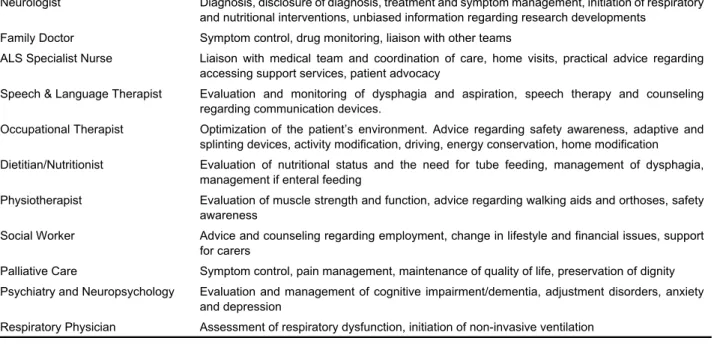
Table 1. Roles of the multidisciplinary team
3Neurologist Diagnosis, disclosure of diagnosis, treatment and symptom management, initiation of respiratory and nutritional interventions, unbiased information regarding research developments
Family Doctor Symptom control, drug monitoring, liaison with other teams
ALS Specialist Nurse Liaison with medical team and coordination of care, home visits, practical advice regarding accessing support services, patient advocacy
Speech & Language Therapist Evaluation and monitoring of dysphagia and aspiration, speech therapy and counseling regarding communication devices.
Occupational Therapist Optimization of the patient’s environment. Advice regarding safety awareness, adaptive and splinting devices, activity modification, driving, energy conservation, home modification Dietitian/Nutritionist Evaluation of nutritional status and the need for tube feeding, management of dysphagia,
management if enteral feeding
Physiotherapist Evaluation of muscle strength and function, advice regarding walking aids and orthoses, safety awareness
Social Worker Advice and counseling regarding employment, change in lifestyle and financial issues, support for carers
Palliative Care Symptom control, pain management, maintenance of quality of life, preservation of dignity Psychiatry and Neuropsychology Evaluation and management of cognitive impairment/dementia, adjustment disorders, anxiety
and depression
Respiratory Physician Assessment of respiratory dysfunction, initiation of non-invasive ventilation
에서 발표되었고 ,
1최근에는 EFNS(European Federation of Neurological Societies)에서 치료에 대한 근거중심적 고찰을 제공하였다 .
2ALS 치료에는 많은 의학적 문제점들과 기능 적 장애 , 정신사회적 문제들이 포함되며, 관련된 분야의 다 양한 의학적 전문가가 참여하는 multidisciplinary ALS clinic 이 필수적이다(Table 1).
3,41. 대증치료(treating symptoms)
Pathologic laughing이나 crying은 환자의 50%에서 발생하 고, 대개 약물에 잘 반응한다. 무작위 연구에서 dextro- methorphan과 quinidine을 같이 쓰면 효과적이라는 보고가 있으나 장기간 (long-term) 부작용과 내약성(tolerability)에 대 한 향후의 연구가 필요하다.
5근육경련(cramp), 근육연축 (fasciculation), 근강직(spastciity), 침흘림(drooling) 증상들은 적절한 약물들에 의해서 완화될 수 있다. 강직을 완화시키 는 약물들은 적당한 강직이 있는 것이 완전히 flaccid 상태 보다 움직임에 있어서는 더 나을 수 있으므로 주의를 요한 다. 치료에 불응성인 침흘림은 botulinum toxin 주사 또는 침 샘의 방사선요법(irradiation)이 고려될 수 있다.
6,7환자의 73%까지 통증을 호소하는데 근골격계의 통증은 대개 관절 주위의 변화된 근긴장도(tone)나 근위축에 의해서 발생하 며,
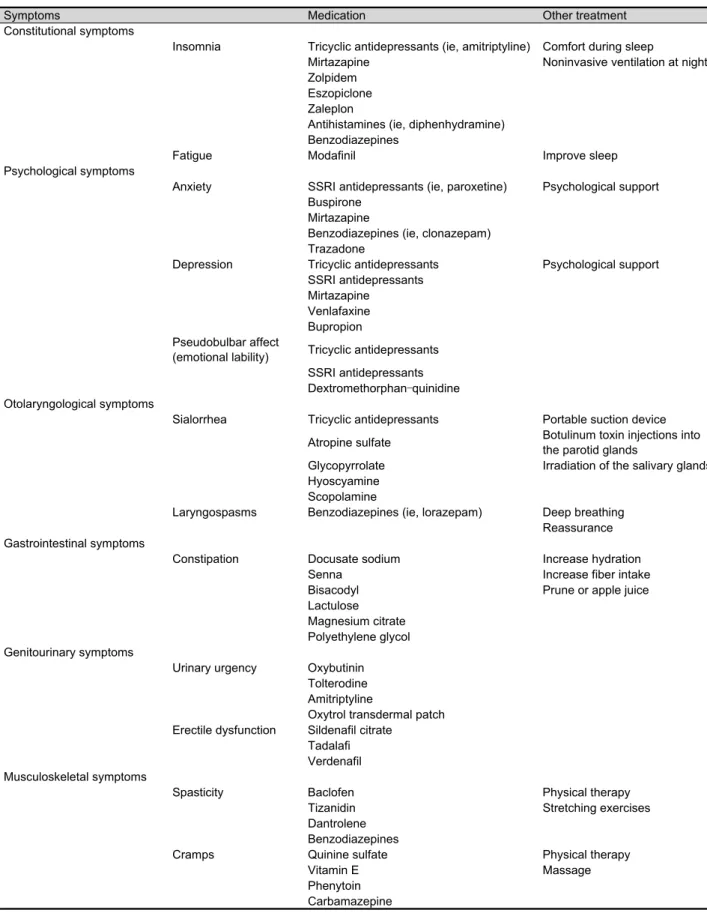
8치료는 physiotherapy, NSAIDs, opioid 등이 있다. 전반적 인 대증치료방법에 대해 Table 2에서 정리하였다.
92. 정신 및 심리사회적 치료(psychiatric and psy- chosocial issues)
신체적인 문제뿐 아니라, 대부분의 환자들이 진단 후 우 울증의 시기를 겪으므로 상담이 필요하다 . 주요 우울증은 약 10%정도로 드물지만 스스로 우울감에 대해 호소하는 경 우가 전체 환자의 44~75%까지 이른다.
10,11Selective serotonin reuptake inhibitor가 가장 흔히 사용되지만, amitriptyline은 침 흘림이나 emotional lability, 수면장애 같은 다른 증상들에 대해서도 좋은 효과를 보인다 . 환자와 간병인사이의 스트 레스 정도와 환자의 우울증이 일치한다는 결과가 있으므로 간병인의 정신적인 건강에 대한 관심이 환자의 스트레스를 줄여 줄 수 있다.
12심리사회적 (psychosocial) 치료도 중요한데, 미국의 자료 에 의하면 많은 환자들이 의사의 도움을 받는 자살(phy- sician-assisted suicide)에 관심을 보인다.
10환자에게 희망과 삶 의 의미를 갖게 하기 위해서는 현재 상태에 대한 적절한 평가 와 약물치료 이외의 여러 치료방법을 시도하는 것을 고려해 야 한다 . 또한 환자를 보살피는 것에 대한 가족들의 부담이 환 자 자신들의 부담보다 클 수 있으므로 특별한 주의가 필요하 고 이런 경우 환자협회에 도움과 조언을 구하는 방법도 있다 .
3. 병의 진행을 늦추는 치료(slowing disease progression)많은 약물들이 연구되고 있지만, 현재까지 인정 받은 것
Table 2. Symptomatic management in amytrophic lateral sclerosis
9Symptoms Medication Other treatment
Constitutional symptoms
Insomnia Tricyclic antidepressants (ie, amitriptyline) Comfort during sleep
Mirtazapine Noninvasive ventilation at night
Zolpidem Eszopiclone Zaleplon
Antihistamines (ie, diphenhydramine) Benzodiazepines
Fatigue Modafinil Improve sleep
Psychological symptoms
Anxiety SSRI antidepressants (ie, paroxetine) Psychological support Buspirone
Mirtazapine
Benzodiazepines (ie, clonazepam) Trazadone
Depression Tricyclic antidepressants Psychological support SSRI antidepressants
Mirtazapine Venlafaxine Bupropion Pseudobulbar affect
(emotional lability) Tricyclic antidepressants SSRI antidepressants Dextromethorphan–quinidine Otolaryngological symptoms
Sialorrhea Tricyclic antidepressants Portable suction device Atropine sulfate Botulinum toxin injections into
the parotid glands
Glycopyrrolate Irradiation of the salivary glands Hyoscyamine
Scopolamine
Laryngospasms Benzodiazepines (ie, lorazepam) Deep breathing Reassurance Gastrointestinal symptoms
Constipation Docusate sodium Increase hydration
Senna Increase fiber intake
Bisacodyl Prune or apple juice
Lactulose Magnesium citrate Polyethylene glycol Genitourinary symptoms
Urinary urgency Oxybutinin Tolterodine Amitriptyline
Oxytrol transdermal patch Erectile dysfunction Sildenafil citrate
Tadalafi Verdenafil Musculoskeletal symptoms
Spasticity Baclofen Physical therapy
Tizanidin Stretching exercises
Dantrolene Benzodiazepines
Cramps Quinine sulfate Physical therapy
Vitamin E Massage
Phenytoin
Carbamazepine
Table 3. Recommendation for breaking the news. AAN Practice Parameter
23The physician should give the diagnosis to the patient and discuss its implications. Respect the cultural and social background of the patient in the communication process by asking whether the patient wishes to receive information or prefers that the information be communicated to a family member. (Guideline)
The diagnosis should always be given in person and never by telephone. (Guideline)
Provide printed materials about the disease and about support and advocacy organizations (Guideline), and a letter or audiotape summarizing what the physician has discussed. (Option)
Avoid the following: withholding the diagnosis, providing insufficient information, delivering information callously, or taking away or not providing hope. (Guideline)
은 glutamate 분비를 억제하는 riluzole이 유일하다.
13Riluzole 은 2개의 대규모 무작위 대조군 연구에서 ALS의 환자의 수 명을 약 3-6개월 정도 연장시켰다.
14,15Cochrane systematic review에서는 the probability of surviving one year에서 약 9%
이득을 , 생존기간에서 약 2개월 연장시키는 효과가 있었 다.
16Riluzole 복용시 오심과 무기력감 등이 발생할 수 있고, 간수치의 상승이 보고되기도 하지만, 대체로 큰 불편 없이 복용 할 수 있다. 또한 장기간 복용에 대한 안정성은 노인 환자 및 말기 환자들을 포함하여 어느 정도 확인되었다.
17-19그 밖의 약물들은 여러 동물모델에서는 효과를 보였지만 임상시험에서는 만족스러운 결과를 보이지 않았다.
4. 근거 중심 치료(evidence-based treatment)
ALS치료에서 근거에 기초를 둔 치료지침을 만들고자 하 는 노력을 많이 해 왔으며, 여러 임상연구와 전문가 의견 등이 기초가 되었다 . 대부분의 환자 관리에 있어 다음과 같 은 원칙이 보편적으로 받아들여진다. 첫째, 환자의 자율성 (autonomy)을 존중해야 하고, 둘째, 환자의 문화적 또는 정 신사회적 배경을 참조하여야 하며, 셋째, 중요한 결정을 할 경우 적절한 timing 을 선택하며, 마지막으로 진단에서부터 말기까지 연속적인 치료를 제공해야 한다.
1) 환자에게 정보 제공하기(informing the patient)
ALS 라는 진단을 환자에게 전달하는 과정에 대한 방법 론은 대부분 암환자들의 연구에 기초한다 . 조용하고 가족 과 함께 있는 환경에서 의사의 참석하에 환자에게 전달하 도록 하며, 환자가 가지고 있는 문화적 배경을 고려하는 것 이 좋다. 환자나 보호자에게 희망을 앗아가는 내용으로 전 달하는 것은 피해야 하며 , 몇 가지 희망적인 이야기를 해 주는 것이 좋다 . 예를 들면, 20% 정도의 환자는 약 5년 이상 생존하고, 10% 환자는 약 10년 이상 생존하기도 하며, 환자 가 겪을 수 있는 문제는 대증치료가 가능하고, FDA 승인을 받은 Riluzole이라는 약물이 있으며, 현재 신경보호 물질에 대한 연구, 유전자 치료, 줄기세포 치료 등 여러 치료 방법
들이 연구 중이므로 향후 보다 효과적인 치료 방법이 개발 될 것이라는 등의 내용을 함께 전달하는 것이 추천된다 . 환 자에게 정보를 제공하는 지침은 Table 3과 같다.
202) 영양공급(nutrition)
영양상태와 체중감소는 생존의 예후 인자이다.
21영양실 조와 체중감소는 연하 장애 , 팔 근육의 위약으로 인한 식사 시간의 연장 , respiratory compromise 로 인한 hypermetabolism 등에 기인한다 . 사래 등으로 인해 입으로 먹는 것이 더 이 상 힘들 때, percutaneous endoscopic gastrostomy (PEG)가 시 행되어야 한다 .
22PEG와 관련된 morbidity는 호흡기능과 연 관성이 있으며, 호흡기능이 악화되면 morbidity는 상승한다.
BDNF 약물연구에서 PEG 의 30일 mortality는 약 9.6%였으 며, vital capacity (VC)가 50% 이상인 환자들에서는 mortality 가 0%였다.
23따라서 안전성과 효율성을 높이기 위해서는 PEG는 forced vital capacity (FVC)가 50% 미만이 되기 전이 나, sniff nasal inspiratory nasal pressure (SNIP)가 40 cmH2O 미만으로 감소되기 전에 시행하는 것이 좋다 .
1Bulbar 증상 이 심하거나 호흡기능이 약화되어 있을 경우 방사선과의 도움을 받아 radiologically inserted gastrostomy (RIG) 를 하는 것이 고려될 수 있다 .
243) 호흡관리(respiratory management)
호흡곤란 (dyspnea)은 ALS 환자에서 매우 심각한 증상이 고 대부분의 환자들이 호흡곤란으로 사망하게 된다. 호흡 관리에 있어 첫째 , 초기 호흡 부전을 감지할 수 있는 가장 좋 은 검사 방법은 무엇인가? 둘째, noninvasive positive pressure ventilation (NPPV)이 저호흡(hypoventilation)을 호전시키고 수명을 연장시킬 수 있는가 ? 셋째, 기계호흡이 삶의 질을 향상시킬 수 있는 가? 넷째, 기계 호흡을 중단할 때, 최적의 방법은 무엇인가? 등의 의문점들이 존재한다.
호흡부전을 초기에 감지할 수 있는 확실하게 우월한 검
사 방법은 없어서 ,
25대개 vital capacity가 50% 이상 감소하
면 호흡 증상이 나타나는 것을 근거로 해서 , vital capacity
를 측정하여 호흡관리 계획을 세워왔다 . 그러나 vital ca-
Table 4. Provisional European consensus criteria for NIV (European ALS/MND Consortium and European Neuromuscular Centre workshop on non-invasive ventilation in MND, May 2002)
Suggested criteria for non-invasive ventilation
Symptoms related to respiratory muscle weakness. At least one of
– Dyspnoea, orthopnoea, disturbed sleep (not caused by pain), morning headache, poor concentration, anorexia, excessive daytime sleepiness (ESS > 9)
AND
Evidence of muscle weakness FVC ≤ 80 % or SNIP ≤ 40 cm H20 AND
Evidence of either
Significant nocturnal desaturation on overnight oximetry OR morning ear lobe gas pC02 ≥ 6.5 kPa ESS Epworth sleepiness scale.
pacity는 민감도에 문제가 있고, 근육위약이나 apraxia가 있 는 환자들은 제대로 실행을 할 수 없으며, 생존과의 연관성 도 낮다. 따라서 최근에는 sniff nasal inspiratory nasal pressure (SNIP)가 유용한 방법으로 사용되고 있다. SNIP은 횡경막의 근력과도 관련이 있고,
26호흡근육의 강도 변화에도 민감하 다.
2798명을 대상으로 한 전향적 관찰연구에서는 마지막 방 문(사망 전이나 연구 종료 전)까지 FVC나 MIP (maximal in- spiratory pressure)에 비해서 SNIP을 비교적 잘 수행할 수 있 었다고 하였다(94 versus 84 versus 79%, respectively).
28SINP
< 40 cmH2O는 6개월 사망을 예견하는 데 FVC 와 비교시 민감도가 높지만 (97 versus 58%), 특이도는 약간 낮은 것으 로 (79 versus 96%) 보고하였다.
NPPV는 저호흡에 효과적이며 삶의 질을 향상시키고 생 존기간을 연장시킨다.
29기관절개술 상태에서 기계호흡을 하는 것은 생존기간을 연장시키지만 비용과 간호 부담이 가중된다 . 기계 호흡을 시작할 때는 어느 상황에서 기계호 흡을 중단할 지 환자와 충분한 교감이 있어야 한다. 왜냐하 면 말기로 갈수록 환자와의 의사소통이 불가능해지기 때문 이다. 마지막으로 기계 호흡을 중단할 때, opioids, 산소, 항 불안제 등이 제공되어야 하고, paralytic drug는 사용하지 않 도록 한다.
NIV에 대한 적응증은 Table 4와 같다.
4) 완화의료(palliative care)