pISSN 2288-9272 eISSN 2383-8493 J Oral Med Pain 2018;43(4):142-146 https://doi.org/10.14476/jomp.2018.43.4.142
Acute Malocclusion Caused by Articular Disc Perforation:
A Case Report
Hyun Nam 1 , Young-Joo Shim 1,2 , Jin-Kyu Kang 1,2
1 Department of Orofacial Pain and Oral Medicine, Wonkwang University Daejeon Dental Hospital, Daejeon, Korea
2 Wonkwang Dental Research Institute, Wonkwang University, Iksan, Korea
Received November 9, 2018 Revised December 7, 2018 Accepted December 12, 2018
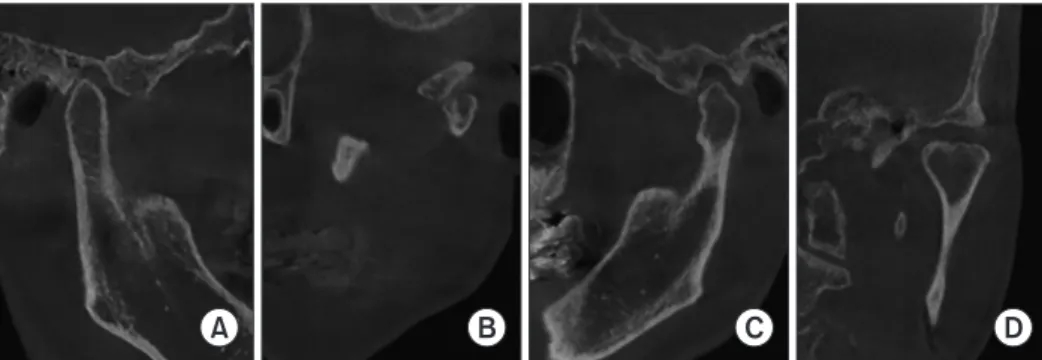
Patients with temporomandibular disorder often present with acute occlusal change and prop- erly managed with conservative treatment. If such change is caused by unusual etiology, dif- ferential diagnosis may be challenged. This article describes the diagnosis of a patient exhibit- ing pain and acute posterior open bite on the ipsilateral side after chewing hard food. After initial conservative treatment failed to resolve the complaint, magnetic resonance imaging was ordered and confirmed partial perforation of articular disc. Disc perforation itself is usually chronic in nature, but sudden macrotrauma may also cause the disorder. However, occlusal discrepancy caused by disc perforation is rare and seldom reported. We present a case of acute malocclusion caused by disc perforation with a review of related literature.
Key Words: Disc perforation; Malocclusion; Posterior disc displacement; Temporomandibular joint
Correspondence to:
Jin-Kyu Kang
Department of Orofacial Pain and Oral Medicine, Wonkwang University Daejeon Dental Hospital, 77 Dunsan- ro, Seo-gu, Daejeon 35233, Korea Tel: +82-42-366-1125 Fax: +82-42-366-1115 E-mail: [email protected] This paper was supported by Wonkwang University in 2018.
JOMP Journal of Oral Medicine and Pain
Copyright Ⓒ 2018 Korean Academy of Orofacial Pain and Oral Medicine. All rights reserved.
CC