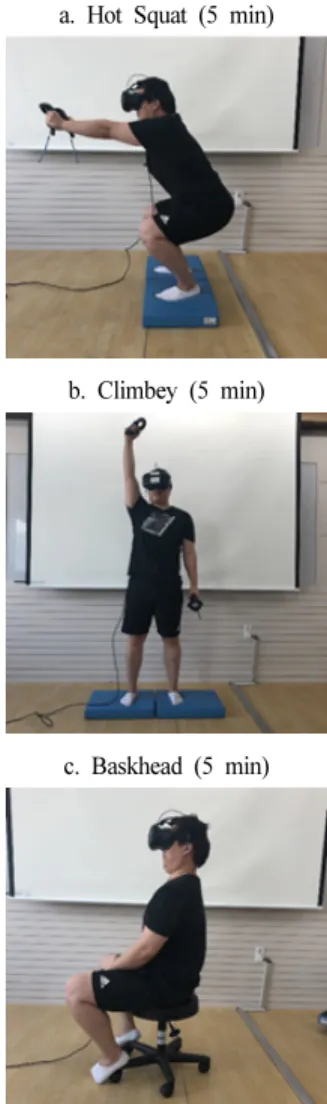
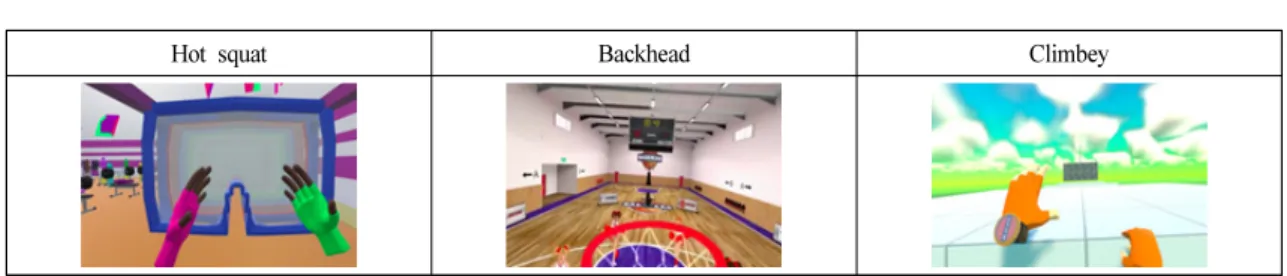
The Effects of Virtual Reality Games in Posture Correction Exercise on the Posture and Balance of Patients with Forward Head Posture
11
0
0
전체 글
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
(11)
수치


+3
관련 문서
During the term of this Agreement, Manufacturer shall not, either directly or indirectly, sell the products in the Territory without the prior consent of distributor...
The index is calculated with the latest 5-year auction data of 400 selected Classic, Modern, and Contemporary Chinese painting artists from major auction houses..
1 John Owen, Justification by Faith Alone, in The Works of John Owen, ed. John Bolt, trans. Scott Clark, "Do This and Live: Christ's Active Obedience as the
This study was conducted to develop and evaluate the effects of a posture management program based on the theory of planned behavior (TPB) which was
A virtual displacement of a generalized coordinate in physical space ~ A combination of virtual displacements subjected to the constraints of... Generally, the
The purpose of this study is to come up with a method to evaluate Virtual Reality Art. To suggest the method, Noël Carroll's category-relative evaluation
Regarding SI or BI EMG measured at upright posture on hard platform, bio-feedback group under the condition with opening both eye and aqua group under the condition with
The greatest difference in heart rate change and Wong-Baker Faces Pain Rating Scale score, between the control and virtual reality distraction groups, was seen in 5 - 7-year-olds
