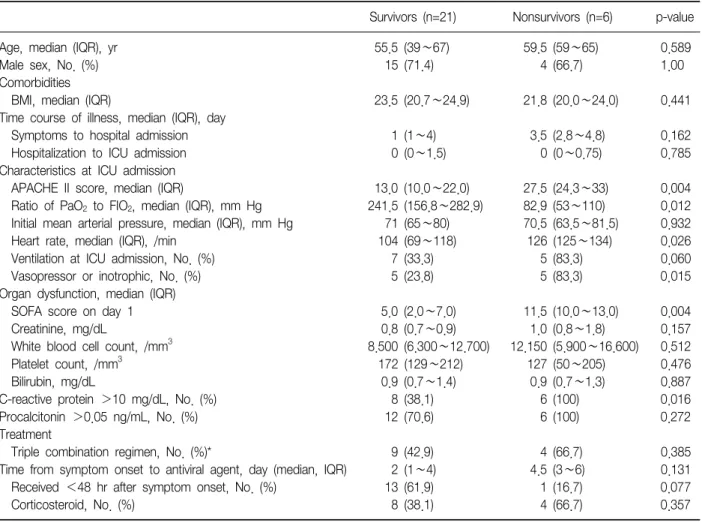
Critically Ill Patients with Pandemic Influenza A/H1N1 2009 at a Medical Center in Korea
8
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
(8)
수치


관련 문서
This book contains hundreds of complete, working examples illustrating many common Java programming tasks using the core, enterprise, and foun- dation classes APIs.. Java Examples
Hepatitis B surface antigen loss in antiviral-treated patients with HBeAg(+) chronic hepatitis B (CHB) infection: observations from antiviral-naïve patients
results of a phase II study of high-dose radiation therapy and neoadjuvant plus concomitant 5-fluorouracil with CDDP chemotherapy for patients with anal
First, there was no significant difference as a result of analyzing the differences in psychological capital, achievement goal orientation, and game roots
Intermittent hemodialysis(IDH) and Continuous renal replacement therapy (CRRT) has been used widely for treating critically ill patients with acute renal failure, We
Median overall survival of 28 multiple myeloma patients treated with Cyclophosphamide-Prednisone combination regimens as a primary therapy was 115 weeks.. Median
In addition, if the patients had a high MPV level (cut-off value of 7.95 fL) without low-dose aspirin therapy, they were at risk for ischemic stroke, especially in
Dombret H, Sutton L, Duarte M, Daniel MT, Leblond V, Castaigne S, Degos L: Combined therapy with all-trans retinoic acid and high-dose chemotherapy in
