대한내시경복강경외과학회지
□ 원 저 □
Vol. 10. No. 2, 2007
79
2 mm 투관침을 사용한 미세 복강경 담낭절제술의 적용
경희대학교 의과대학 외과학교실, 1동수원병원 외과
권택수ㆍ이상목ㆍ박선진ㆍ주선형ㆍ홍성화ㆍ오수명ㆍ박철운1
Clinical Application of 2 mm Trocar Mini-laparoscopic Cholecystectomy
Taek Soo Kwon, M.D., Sang Mok Lee, M.D., Sun Jin Park, M.D., Sun Hyoung Ju, M.D., Sung Wha Hong, M.D., Soo Myung Oh, M.D., Chul Woon Park, M.D.1
Department of Surgery, Kyung Hee University College of Medicine, 1Dongsuwon Hospital, Suwon, Korea
Purpose: The use of mini-laparoscopic cholecystectomy (mini-LC) has been reported to cause less postoperative pain and a better cosmetic effect than the use of conventional laparoscopic cholecystectomy (LC). However, it has not been a popular procedure because of instrument deficiencies and visual limitations. We report our experience of the clinical application of 2 mm mini-LC.
Methods: We compared three groups of patients that underwent LC. Two groups of patients underwent LC using 2 mm trocars-a consecutive group and a selective group. A third group of consecutive patients (conventional group) underwent LC using 5 mm trocars. The consecutive group consisted of 54 cases, and the selective group consisted of 117 cases that were selected by a surgeon based on patient condition. The conventional group consisted of 165 cases.
Results: The sex ratio of the consecutive group, selective group, and conventional group of patients was 1:1.16, 1:
2.77 and 1:1.54 males:females, respectively. The mean age of patients in the consecutive group, selective group, and
conventional group was 41.5, 42 and 56.1 years, respectively.
The mean surgical time of patients in the consecutive group, selective group, and conventional group was 74.7, 65.8 and 79.6 minutes, respectively, and the mean hospital stay was 2.7, 1.7 and 3.2 days, respectively. Complications occurred in 3, 10 and 5 cases for patients in the consecutive group, selective group, and conventional group, respectively. The mean surgical time and hospital stay were significant for the selective group of patients.
Conclusion: Although 2 mm mini-LC was difficult to perform due to instrument limitations and a requirement of experience, the procedure resulted in a shorter surgical time and pos- toperative hospital stay. There was no difference in the rate of complications as compared with the use of conventional LC if an experienced surgeon performed the procedure.
Key words: Laparoscopic cholecystectomy, Mini-laparosopic cholecystectomy
중심단어: 복강경 담낭절제술, 미세복강경 담낭절제술
※ 통신저자:이상목, 서울시 동대문구 회기동 1 우편번호:130-702
경희의료원 외과
Tel:02-958-8269, Fax: 02-966-9366 E-mail:[email protected]
서 론
복강경 담낭절제술은 최소침습 수술이 가지는 여러 가지 장점들로 인하여 담낭절제술의 표준술식의 하나로 인정되 고 있다.1-4 최근 2 mm 투관침을 사용한 미세복강경 담낭절 제술은 복강경 수술이 가지는 장점들 중에서 특히 미용적 인 장점과 통증의 감소를 보고하고 있다.5 하지만 기구가 약해 적용에 제한이 따르며 2 mm 카메라의 경우 시야가 좁고 화질이 좋지 않아 적응증에 제한이 있어 보편화되지 못하고 있다.
최근 시대적인 흐름이 미용학적인 측면이 강조되는 추세 로 인하여 미용학적으로 결과가 우수한 2 mm 투관침을 사
용한 미세복강경 담낭절제술의 임상적 적용이 강조되고 있 다(Fig. 1). 저자들은 제대부에 10 mm 투관침을 삽입하고 다른 부위에는 2 mm 투관침만을 사용한 미세복강경 담낭 절제술을 시행하여 기존 5 mm 투관침을 사용한 3공식 복강 경 담낭절제술과 평균 수술시간, 수술 후 평균입원 기간, 합 병증 등을 비교하여 그 임상적 유용성을 알아보고자 하였 다.
대상 및 방법 1) 환자군
경희대학교 의과대학 외과학교실에서 적극적으로 미세복 강경 담낭절제술을 시행한 2004년 1월부터 2007년 2월까지 의 171예 중에서 2004년 1월에서 2004년 8월까지 모든 수술 의 적응증이 되는 모든 환자에게 연속적으로 시행한 군(이 하 연속군) 54예와 이후 2007년 2월까지 제대부 투관침을 통하여 카메라를 삽입한 후 담낭의 상태나 환자 나이, 상태 등 임상적 특성을 고려하여 수술이 용이할 것으로 판단되어
80 대한내시경복강경외과학회지 제10권 제2호 2007
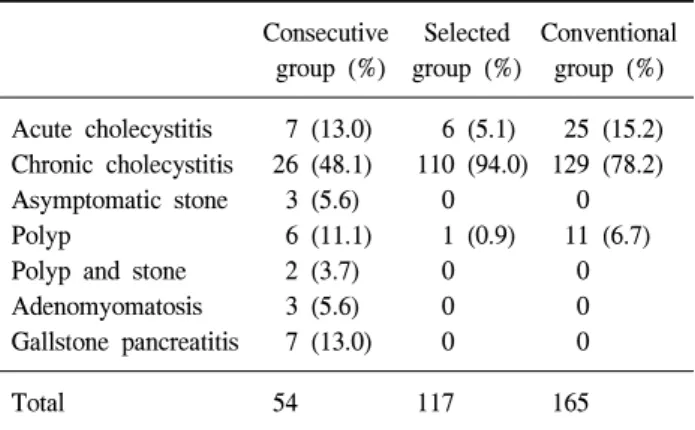
Table 1. Operative indication
Consecutive Selected Conventional group (%) group (%) group (%) Acute cholecystitis 7 (13.0) 6 (5.1) 25 (15.2) Chronic cholecystitis 26 (48.1) 110 (94.0) 129 (78.2) Asymptomatic stone 3 (5.6) 0 0 Polyp 6 (11.1) 1 (0.9) 11 (6.7) Polyp and stone 2 (3.7) 0 0 Adenomyomatosis 3 (5.6) 0 0 Gallstone pancreatitis 7 (13.0) 0 0
Total 54 117 165
Fig. 1. Comparison of scaring 36 months after surgery.
선택적으로 미세복강경 담낭절제술을 시행한 군(이하 선택 군) 117예를 구분하였고, 과거 1997년 1월에서 1998년 6월까 지 5 mm 투관침을 사용하여 3공식 복강경 담낭절제술을 연 속적으로 시행한 군(이하 고식군) 165예를 구분하였다.
2) 수술 방법
모든 환자는 전신, 흡입마취를 시행하였고 비위관은 제 대부 투관침을 통하여 카메라를 삽입한 다음 위 감압이 필 요한 경우에만 삽입하였으며 도뇨관은 급성 담낭염으로 응 급수술을 시행한 환자에게만 삽입하였다.
투관침의 위치는 제대부에 10 mm 투관침을, 기타 다른 부위는 통상적인 복강경 담낭절제술과 같은 위치에 2 mm 투관침을 삽입하였다. 2 mm 투관침은 통상적으로 3개를 사 용하였으며 수술진행에 어려움이 있는 경우, 2 mm 투관침 을 추가로 삽입하거나 2 mm 투관침을 5 mm로 전환하여 수술을 진행하였다.
수술은 먼저 제대하방에 10 mm 카메라를 삽입하고 복강 내 이상 유무를 전체적으로 확인한 다음 2 mm 투관침을 삽입하고, 2 mm 기구를 사용하여 담낭관과 담낭 동맥을 충 분히 박리한 후 검상돌기부 투관침에 2 mm 카메라를 넣고 제대부의 10 mm 투관침을 통하여 복강경 클립으로 담낭관 과 담낭동맥을 결찰한 다음 제대부에 10 mm 카메라를 재차 삽입하여 담낭관과 담낭동맥의 결찰부위를 확인한 후 2 mm 내시경 가위로 담낭관과 담낭동맥을 절단하였다. 이후 2 mm 전기소작기를 사용하여 담낭을 박리, 절제한 후 비닐 주머니에 담아 10 mm 투관침을 통하여 제거 하였다. 기타 모든 것은 통상적인 복강경 담낭절제술과 같은 방법으로 시행하였으며 2 mm 투관침이 삽입된 상처는 봉합하지 않 았다.
3) 기타
수술 시간은 피부절개부터 봉합까지 소요되는 시간으로 하였고 수술 후 재원일수는 수술을 받은 후 퇴원하는 날까 지로 하였다. 모든 자료는 의무기록을 중심으로 후향적으로 분석하였으며 평균치 비교는 일원배치 분산분석을, 합병증 비율 비교는 chi-squared test와 Fisher's exact test를 이용하였 으며 p값이 0.05 미만인 경우를 유의한 것으로 하였다.
결 과 1) 환자의 특성
연속군은 54예로 남자 25예, 여자 29예로 남녀 비는 1:
1.16, 평균나이는 41.5세였다. 선택군은 117예로 남자 31예, 여자 86예로 남녀 비는 1:2.77로 평균나이 42세였다. 고식 군의 경우 남자 65예, 여자 100예 남녀 비는 1:1.54로, 평균 나이 56.1세였다. 세 군 모두 여성의 비율이 높았으며 임상 적으로 급성 담낭염과 만성 담낭염의 증례 수는 각각 연속 군에서는 7예(13.0%)와 26예(48.1%), 선택군은 6예(5.1%)와 110예(94.0%), 고식군은 25예(15.2%)와 129예(78.2%)로 연 속군과 고식군에서 선택군에 비하여 급성 담낭염의 비율이 높았다(Table 1).
2) 수술 결과
평균 수술시간은 연속군, 선택군, 고식군에서 각각 74.7 분, 65.8분, 79.6분으로 선택군이 가장 짧았으며 수술 후 평 균입원 기간은 각각 2.77일, 1.42일, 3.2일로 선택군이 가장 짧았다.
수술진행에 어려움이 있어 2 mm 투관침을 5 mm로 전환 한 경우는 연속군에서 6예(11.1%), 선택군에서 18예(15.3%) 였지만 개복수술로 전환한 경우는 없었다. 반면에 고식군 의 경우 4공술로 전환한 경우가 6예(3.6%), 개복술로 전환 한 경우가 1예(0.6%)있었다. 합병증으로 연속군, 선택군, 고 식군이 각각 3예(5.6%), 10예(8.5%), 5예(3.0%) 있었다(Table
권택수 외 6인: 2 mm 투관침을 사용한 미세 복강경 담낭절제술의 적용 81
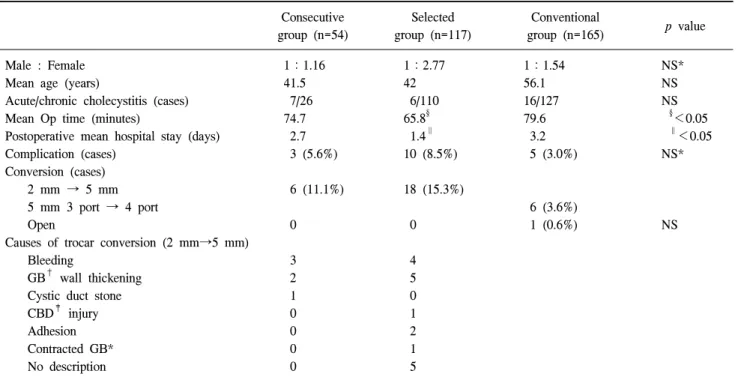
Table 2. Patient demographics and operative outcome
Consecutive group (n=54)
Selected group (n=117)
Conventional
group (n=165) p value
Male : Female 1:1.16 1:2.77 1:1.54 NS*
Mean age (years) 41.5 42 56.1 NS
Acute/chronic cholecystitis (cases) 7/26 6/110 16/127 NS
Mean Op time (minutes) 74.7 65.8§ 79.6 §<0.05
Postoperative mean hospital stay (days) 2.7 1.4∥ 3.2 ∥<0.05
Complication (cases) 3 (5.6%) 10 (8.5%) 5 (3.0%) NS*
Conversion (cases)
2 mm → 5 mm 6 (11.1%) 18 (15.3%)
5 mm 3 port → 4 port 6 (3.6%)
Open 0 0 1 (0.6%) NS
Causes of trocar conversion (2 mm→5 mm)
Bleeding 3 4
GB† wall thickening 2 5
Cystic duct stone 1 0
CBD‡ injury 0 1
Adhesion 0 2
Contracted GB* 0 1
No description 0 5
*NS = not significant; †GB = gall bladder; ‡CBD = common bile duct.
2).
평균 수술시간 및 수술 후 평균입원기간은 선택군에서 유의하게 짧았고 기타 개복술로의 전환, 합병증 발생 등은 세 군간에 유의한 차이를 보이지 않았다.
고 찰
복강경 담낭절제술은 최소침습수술로서 초창기의 성공 적 시술이 발표되어 효율성과 안정성이 인정되었고 수술 후 동통의 감소, 입원기간 단축, 정상생활로의 빠른 복귀 및 우수한 미용적 효과 등의 장점으로 인하여 최근 담낭절제 술의 80∼93%을 복강경으로 시행할 만큼 담낭절제술의 표 준술식으로 자리잡고 있다.6
최근에는 복강경 수술의 장점인 비침습적인 측면과 미용 학적인 욕구를 충족하기 위해 투관침의 숫자와 크기를 줄 이는 추세이다.7-12,27-28
감소된 절개창 통증은 복강경 수술의 장점이지만 절개창 의 크기와 통증의 감소는 직접적인 연관이 있다는 것은 통 증의 다변수적인 원인으로 인해 아직 확증적이지 않다.13 그 럼에도 불구하고 여러 연구들은 크기가 작은 절개창일수록 수술 후 통증의 감소를 보고하고 있다.14-18 Cheah 등12은 여 러 전향적 무작위 시험에서 세 개의 5 mm 투관침보다 세 개의 2 mm 투관침을 사용한 복강경 담낭절제술에서 수술 후 통증 및 진통제 사용의 현저한 감소를 보고하였다.
Bisgaard 등19은 크기가 작은 투관침에서 수술 6시간 후 통 증의 감소를 보고하였다. 또한 Novitsky 등5은 수술 후 28일 째에 5 mm 투관침을 사용한 환자들 74%에서, 2 mm 투관침 을 사용한 환자들 90%에서 유의한 차이를 보이며 통증이 사라졌다고 보고 하였다.
미용적 측면에서 객관적인 척도는 아직 없지만, 크기가 작은 투관침 사용이 최소한의 반흔과 좀더 나은 미용적 결 과가 보고 되었다.20-21 Huang 등17은 2 mm 투관침만을 사용 한 미세복강경 담낭절제술에서 기구가 약해서 수술시간의 지연은 있으나 명치부위에 5 mm 투관침을 사용하면 수술 시간에 유의한 차이가 없다고 보고하였다. 또한 다른 연구 에서도 유의한 수술시간의 지연이 없음을 보고하고 있 다.5,15,18-19,22
그러나 저자들의 경우 선택군에서 수술시간이 의미있게 단축되었다.
미세복강경 담낭절제술에서 5 mm 투관침으로 또는 개복 수술로의 전환은 23∼38%로 보고되고 있으나,16,22,23 저자들 의 경우 개복수술로의 전환한 경우는 없었지만 5 mm 투관 침을 사용한 고식군에서 개복수술로 전환된 경우가 1예 (0.6%) 있었지만 통계학적 의미는 없었다.
미세복강경 수술의 경우 수술 후 평균입원기간이 당일 퇴원에서 약 2일까지 보고되고 있는 반면 5 mm 투관침의 경우 약 4일로 보고되고 있다.24-26 저자들의 경우에서도 2 mm 선택군에서 1.4일로 연속군의 2.7일과 5 mm 투관침을 사용한 고식군의 3.2일보다 유의하게 짧았다.
82 대한내시경복강경외과학회지 제10권 제2호 2007
결론적으로 미세복강경 담낭절제술은 기구 사용의 제한 으로 인한 적응증의 제한, 카메라를 교체하는 등의 번거로 움과 복강경 수술의 많은 경험이 요구되는 수술이다.27 하지 만 복강경 수술에 경험이 많은 의사들이 선택적으로 시행 한다면 기존의 복강경 담낭절제술처럼 쉽고 안전하게 시행 할 수 있어 미용학적인 측면이 강조되는 환자들에게서 적 극적으로 시도해볼 수 있는 수술방법이라고 생각한다.
참고문헌
1) Bickel A, Rappaport A, Kanievski V, et al. Laparoscopic management of acute cholecystitis. Prognostic factors for success. Surg Endosc 1996:10;1045-1049.
2) Steinbrook RA, Brooks DC, Datta S. Laparoscopic surgery during pregnancy. Am J Surg 1997;174:222.
3) Wilson RG, Macintyre IM, Nixon SJ, Saunders JH, Varma JS, King PM. Laparoscopic cholecystectomy as a safe and effective treatment for severe acute cholecystitis. BMJ 1992;
305:394-396.
4) Eubanks S, Schauer PR. Laparoscopic surgery. In: Sabiston DC, editor. Textbook of Surgery. 15th ed. Philadelphia: W.B.
Saunders. 1997;353-354.
5) Novitsky YW, Kercher KW, Czerniach DR, et al. Advantages of mini-laparoscopic vs conventional laparoscopic chole- cystectomy: results of a prospective randomized trial. Arch Surg 2005;140:1178-1183.
6) Bailey RW, Zucker KA, Flowers JL, Scovill WA, Graham SM, Imbembo AL. Laparoscopic cholecystectomy: experience with 375 consecutive patients. Ann Surg 1991;214:531-535.
7) Kim E, Hiura A, Ikehara T, et al. Three-Portal technique for laparoscopic cholecystectomy. J HBP Surg 1996;3:285.
8) Patrick RR, Joseph IK, Bruce A, et al. Feasibility of laparoscopic cholecystectomy with miniaturized instrumenta- tion in 50 consecutive cases. World J Surg 1999;23:128-132.
9) Tanaka J, Andoh H, Koyama K. Minimally invasive needle- scopic cholecystectomy. Jpn J Surg 1998;28:111-113.
10) Kimura T, Sakuramachi S, Yoshida M, et al. Laparoscopic cholecystectomy using fine-caliber instruments. Surg Endosc 1998;12:283-286.
11) Hsieh C. Early minilaparoscopic cholecystectomy in patients with acute cholecystitis. Am J Surg 2003;185:344-348.
12) Cheah WK, Lenzi JE, Kum CK, et al. Randomized trial of needlescopic versus laparoscopic cholecystectomy. Br J Surg 2001;88:45-47.
13) Bisgaard T, Klarskov B, Rosenberg J, Kehlet H.
Characteristics and prediction of early pain after laparoscopic cholecystectomy. Pain 2001;90:261-269.
14) Ngoi SS, Goh P, Kok K, Kum CK, Cheah WK. Needlescopic
or minisite cholecystectomy. Surg Endosc 1999;13:303-305.
15) Schwenk W, Neudecker J, Mall J, Bohm B, Muller JM.
Prospective randomized blinded trial of pulmonary function, pain, and cosmetic results after laparoscopic vs micro- laparoscopic cholecystectomy. Surg Endosc 2000;14:345-348.
16) Look M, Chew SP, Tan YC, et al. Post-operative pain in needlescopic versus conventional laparoscopic cholecystec- tomy: a prospective randomised trial. J R Coll Surg Edinb 2001;46:138-142.
17) Huang MT, Wang W, Wei PL, Chen RJ, Lee WJ. Minilaparo- scopic and laparoscopic cholecystectomy: a comparative study.
Arch Surg 2003;138:1017-1023.
18) Sarli L, Iusco D, Gobbi S, Porrini C, Ferro M, Roncoroni L.
Randomized clinical trial of laparoscopic cholecystectomy performed with mini-instruments. Br J Surg 2003;90:1345- 1348.
19) Bisgaard T, Klarskov B, Trap R, Kehlet H, Rosenberg J.
Microlaparoscopic vs conventional laparoscopic cholecystectomy:
a prospective randomized doubleblind trial. Surg Endosc 2002;
16:458-464.
20) Gagner M, Garcia-Ruiz A. Technical aspects of minimally invasive abdominal surgery performed with needlescopic instruments. Surg Laparosc Endosc 1998;8:171-179.
21) Yuan RH, Lee WJ, Yu SC. Mini-laparoscopic cholecystectomy:
a cosmetically better, almost scarless procedure. J Laparoendosc Adv Surg Tech A 1997;7:205-211.
22) Alponat A, Cubukcu A, Gonullu N, Canturk Z, Ozbay O. Is minisite cholecystectomy less traumatic? Prospective randomized study comparing minisite and conventional laparoscopic cholecy- stectomies. World J Surg 2002;26:1437-1440.
23) Bisgaard T, Klarskov B, Trap R, Kehlet H, Rosenberg J. Pain after microlaparoscopic cholecystectomy: a randomized double- blind controlled study. Surg Endosc 2000;14:340-344.
24) Lee KW, Poon CM, Leung KF, Lee DW, Ko CW. Two-port needlescopic cholecystectomy: prospective study of 100 cases.
Hong Kong Med J 2005;11:30-35.
25) Leggett PL, Bissell CD, Churchman-Winn R, Ahn C.
Three-port microlaparoscopic cholecystectomy in 159 patients.
Surg Endosc 2001;15:293-296.
26) Park GJ, Shin JH. 1,000 cases of laparoscopic chole- cystectomy by a single surgeon. J Korean Surg Soc 2004;
66:123-127.
27) Jin CI, Lee SM, Hong SH. Laparoscopic cholecystectomy with miniaturized instrumentation. J Korean Soc Endosc Laparosc Surg 2005;8:62-65.
28) Hur SH, Lee SM, Koh SH, Hong SH, Oh SM. The Usefulness of Three-portal Technique for Laparoscopic Cholecystectomy.
J Korean Soc Endosc Laparosc Surg 1999;2:41-48.