1
Dep. of Implantology, Graduate School of Clinical Dentistry, Ewha Womans University
2
Dep. of Dentistry, School of Medicine, Ewha Womans University
Abstract
The purpose of this study was to evaluate the 6-year cumulative survival rate (CSR) of single implants placed in mandibu- lar posterior free end region and examined associated factors.
One hundred and eight single implants placed in mandibular posterior free end region were selected from subjects who had visited the Dental Hospital of Ewha Womans University, from January 2002 through June 2008. One to six year CSR was calculated using the life-table analysis. In addition, associated factors, such as the implant systems, length and diameter of the implant fixture, and the age and gender of patients were compared and analyzed using the chi-squre test.
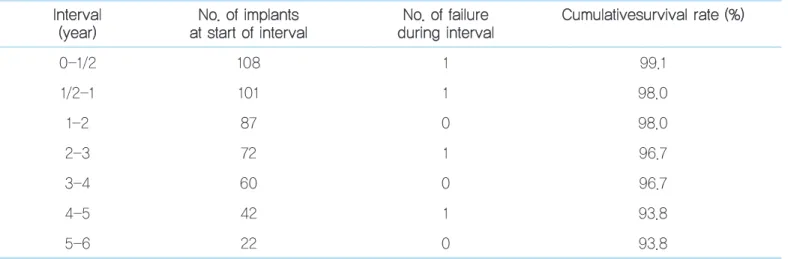
Of 108 implants, four has failed. The 6 year CSR was 93.8%. There were no significant differences between the age groups and gender of patients in the CSR and the CSR between the implant systems were not significant. The length and diameter of the implant fixtures may not be related with cumulative survival rate. The single implants placed in mandibular posterior free end region presented a reliable CSR, 93.8% for 6years. Within the limitation of this results, the length, diame- ter, and the implant systems did not show any significant differences in cumulative survival rate.
Key words: free end; posterior mandible; survival rate; single implant;
Survival rate of the single implant restoration placed in posterior mandibular free end
Ho-Jin Kwon
1, Myung-Rae Kim
1, 2, Ji-Man Park
2, Eun-Kyoung Pang
2, Sun-Jong Kim
1, 2하악 구치부 유리단에 식립된 단일 임프란트보철물의 생존률에 대한 연구
권호진1, 김명래1, 2, 박지만2, 방은경2, 김선종1, 2
1
이화여자대학교 임상치의학대학원 임프란트과
2
이화여자대학교 의학전문대학원 치과학교실
임
프란트의 성공은 식립 위치는 물론 임프란트의 종 류와 길이, 고정체의 표면 처리, 고정체와 지대주 의 연결방식, 술자의 숙련도 등 다양한 요소의 영 향을 받을 수 있다. 최근에는 재료와 술식의 발달로 합병증이 많이 줄고 치료의 신뢰성도 높게 평가받고 있으나 단일 임프 란트 수복은 인접 구조의 지지를 받지 못하므로 시술 방법과 임프란트 선택에 신중해야 하며 특히 최후방 구치의 경우 세 심한 고려가 필요하다. 상악과 하악은 골질이 다르고 동일 악 골 내에서도 후방으로 갈수록 교합력이 증가하므로 성공률도 다르게 나타날 수 있다. 또 인접치의 존재 여부도 영향을 미칠 수 있으나 최후방 구치에 관한 보고는 많지 않다. Levin 등
1)은 10년간의 장기적인 연구에서 81명의 환자를 대상으로 상 하악 대구치 부위 단일 임프란트의 성공율을 92.6%로 보고했 으며 Schwartz-Arad 등
2)은 상하악대구치 부위에 식립된 78개 단일 임프란트의 성공률을 93.6%로 보고했다. 이 등
3)이 Brånemark 임프란트를 대상으로 분석한 하악 대구치 단 일 임프란트에 관한 연구를 보면 제 1대구치의 생존율이 100%, 제 2대구치는 70.37%로 많은 차이를 보였고, Jung 등
4)
은 하악 대구치 부위에 식립된 sand-blasted, large-grit,
과 같은 의미로 임프란트를 제거하기 전까지 구강 내에 남아 있으면서 기능하는 임프란트의 비율로 정의할 수 있으며, 임 프란트의 임상적 적합성에 대한 다양한 평가 기준을 만족시 키는 성공률과는 차이가 있다.
본 연구는 하악 최후방 대구치 유리단에 식립된 단일 임프 란트의 6년 누적생존율을 통해 치료의 신뢰성을 평가하고, 연 령, 성별, 임프란트 종류, 임프란트 고정체의 길이와 직경과 같은 관련 요소의 영향을 알아보기 위해 시행되었다. 방사선 사진을 통해 임프란트 주위 골변화도 를 조사하여 임프란트 의 안정성에 대해 알아보았다.
1. 연구대상
2002년 1월부터 2008년 6월까지 이화여자대학교 목동병 원 치과진료부에 내원하여 하악 최후방 구치부 유리단에 단 일 임프란트가 식립된 98명의 환자를 대상으로 하였다. 10명 의 환자에서 양측 최후방에 2개의 단일 임프란트를 식립되어
Ⅱ
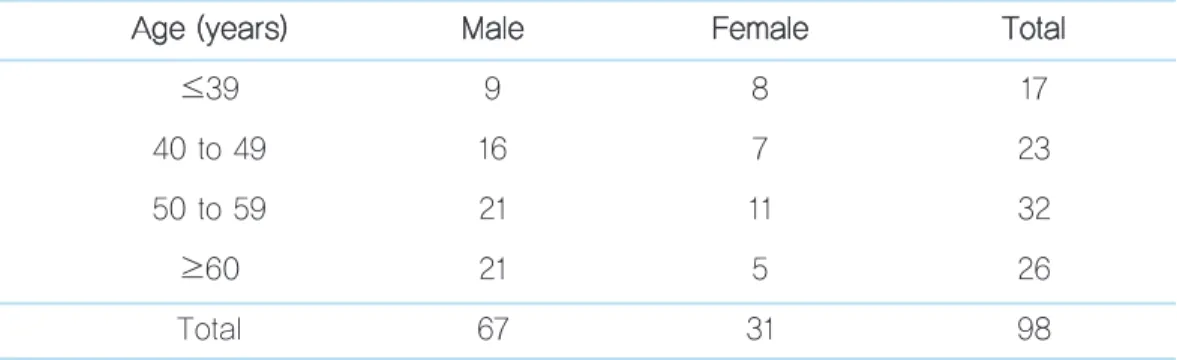
Table 1. Age and Gender of the Subjects Followed up for 6 Years A
Ag ge e ((y ye ea arrs s)) M Ma alle e F Fe em ma alle e T To otta all
≤39 9 8 17
40 to 49 16 7 23
50 to 59 21 11 32
≥60 21 5 26
Total 67 31 98
Ho-Jin Kwon et al: Survival rate of the single implant restoration placed in posterior mandibular free end. Implantology 2010
original article
임프란트 개수는 모두 108개였다. 98명 중 남성은 67명, 여성 은 31명이었다. 연령은 24세부터 76세까지의 분포를 보였고 50대 환자가 32명으로 가장 많았으며 60대 이상이 26명, 40 대가 23명 순이었다. 평균 연령은 51.3세였다(Table 1).
2. 연구방법
통상적인 술식으로 임프란트 수술을 시행하였고 최소 2개 월 이상의 치유기간이 지난 후 상부 보철물을 제작하였다. 보 철물 장착 여부와 관계없이 구강 내에서 제거된 임프란트는 실패로 간주하였다. 생존율은 연령 및 성별, 임프란트 종류, 임프란트 고정체의 길이와 직경을 일정 범위로 분류하여 각 각 계산하였다. 사용된 임프란트는 5종류로서Replace Select
Ⓡ(Nobel Biocare, Sweden)가 36개, Branemark MKIII
Ⓡ(Nobel Biocare, Sweden)가 25개, Osstem SSII
Ⓡ(Osstem, Korea)가 25개, Ankylos
Ⓡ(Degussa, Germany) 가 18개, ITI
Ⓡ(Straumann, Swiss)가 4개 식립되었다.
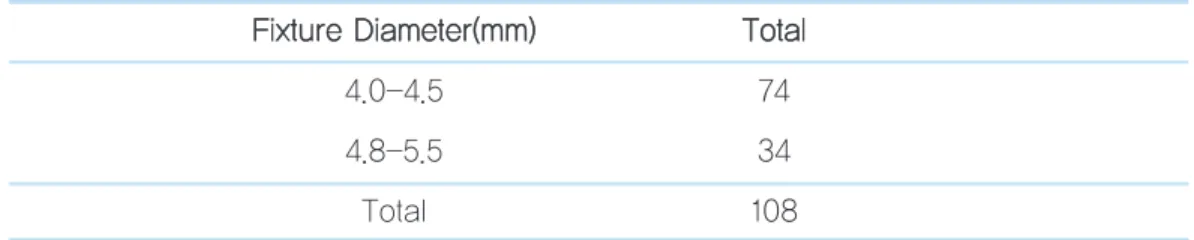
고정체의 길이와 직경은 각 제조회사에 따라 차이가 있어 일정범위를 정하였다. 길이는 8, 8.5, 9.5, 10, 11, 11.5, 13, 14 mm로 8종류를 세 범위로 나누었고 직경은 4, 4.1, 4.3, 4.5, 4.8, 5, 5.5mm 모두 7종류를 두 범위로 나누어 생존율 을 계산하였다(Table 2, Table 3).
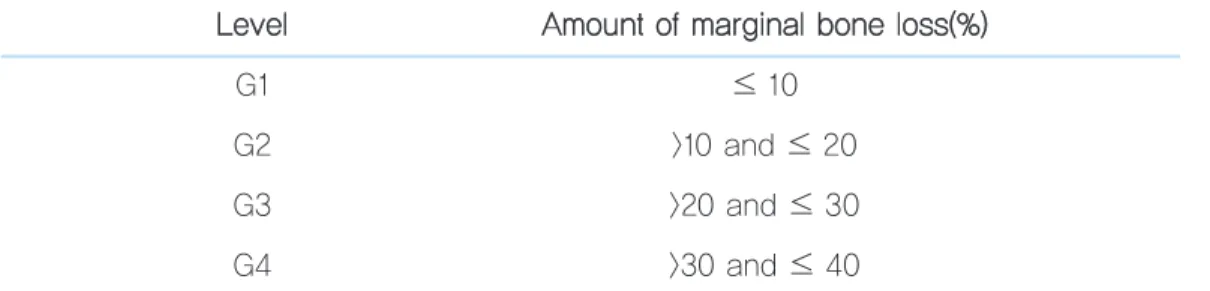
임프란트 주위 변연골 흡수 정도를 알아보기 위해 파노라마 사진을 이용하였다. 식립 당시 고정체가 매식된 골양, 즉 골- 임프란트 계면의 최하방으로부터 임프란트 collar 부근 골이 덮여있는 높이까지를 100으로 하였으며 근원심 중 흡수가 더 많이 된 최저점을 기준으로 하여 수직골 소실만을 조사하였 다. 6개월, 1년, 2년, 4년, 6년에 걸쳐 흡수된 양에 따라 Table 4에서 보는 바와 같이 10% 단위로 등급을 정했다.
식립된 총 108개의 임프란트에 대하여 Life-table analy- sis를 시행하고, 각 기간별로 제거된 임프란트 수를 기록하여 6년간의 누적 생존율을 계산하였다.
6)Table 2. Number of Implants Grouped by Fixture Length F
Fiix xttu urre e L Le en ng gtth h((m mm m)) T To otta all
≤9.5 12
10-11.5 65
≥13 31
Total 108
Ho-Jin Kwon et al: Survival rate of the single implant restoration placed in posterior mandibular free end. Implantology 2010
Table 3. Number of Implants Grouped by Fixture Diameter F
Fiix xttu urre e D Diia am me ette err((m mm m)) T To otta all
4.0-4.5 74
3. 통계학적 분석
각 항목의 자료를 토대로 여러 요인에 따른 생존율을 계산 하고, SPSS 프로그램에서 χ
2- test를 통해 유의성을 검증하 였다(P <0.05).
연령별 생존율을 보면 40대에서 2개 실패하여 91.3%, 50 대, 60대 이상에서 1개씩 실패하여 각각 96.9%, 96.2%를 보 였다. 전체 생존율은 95.9%였다(Table 5). 성별에 따른 생존 율의 차이를 보면 남성은 95.5%, 여성은 96.8%였다. 두 요인
모두 통계학적 유의성은 없었다(P>0.05).
1. 임프란트 종류에 따른 생존율
Replace Select
Ⓡ가 2개, Branemark MKIII
Ⓡ가 2개 실패 하여 94.4%, 92%를 보였고 다른 임프란트는 모두 생존하였 으나 통계학적 유의성은 없었다(Table 6).
2. 임프란트 고정체의 길이와 직경에 따른 생존율
10mm 길이의 임프란트가 2개, 11.5mm, 13mm의 임프란 트가 각각 1개씩 실패하였고, 4mm 직경 임프란트가 2개, 4.3mm 임프란트가 2개 실패하였다. 생존율에 다소 차이가 있으나 통계적 유의성은 없었다(Table 7, Table 8).
Ⅲ
G2 >10 and ≤ 20
G3 >20 and ≤ 30
G4 >30 and ≤ 40
Ho-Jin Kwon et al: Survival rate of the single implant restoration placed in posterior mandibular free end. Implantology 2010
Table 5. Survival Rate According to Age Group A
Ag ge e T To otta all F Fa aiille ed d iim mp plla an ntts s S Su urrv viiv va all rra atte e((% %))
≤39 17 0 100
40 to 49 23 2 91.3
50 to 59 32 1 96.9
≥60 26 1 96.2
Total 98 4 95.9
Ho-Jin Kwon et al: Survival rate of the single implant restoration placed in posterior mandibular free end. Implantology 2010
original article
3. 누적 생존율