Department of Oral and Maxillofacial Surgery, School of Dentistry, Chosun University, Gwangju, Republic of Korea
Abstract
Maxillary sinus augmentation is used for implant placement in edentulous maxilla with alveolar bone resorption. It has relatively few complications and a high success rate. The purpose of this study was to evaluate the prognosis for various conditions after maxillary sinus grafting to improve insufficiency of remaining bone when placing implants in posterior maxilla over the last 10 years. We analyzed 1,121 implants in 404 patients who underwent maxillary sinus grafting and implantation during the last 10 years at Chosun University Dental Hospital. Statistically speaking, the implant survival rates did not differ significantly according to systemic disease and bone quality, implant type and surface treatment, graft materi- als, surgery stage or type of membrane. In contrast, residual bone height, approach technique and Schneiderian membrane perforation were associated with significant differences in implant survival. Overall, however, implants generally survived well. This study suggested that maxillary sinus grafting is a safe procedure.
Key Words : maxillary sinus grafting, retrospective study, survival rate (Implantology 2010; 14(2): 82~95)
The Maxillary Sinus Grafting and Survival Rate of Implants : A 10-year Retrospective Study
Su-Gwan Kim, Kyung-In Jeong
조선대학교 치의학전문대학원 구강악안면외과학교실
※ 본 연구는 2009년도 대한구강악안면임프란트학회 치예원 학술상의 지원에 의하여 수행되었음.
서론
1960년대 보철 치료를 위해 Boyne과 James1에 의해 상악동 거상술이 시작된 이후로 거상술을 이용한 임프 란트 식립의 빈도는 날로 증가하고 있으며 상악동 거상 방법과 재료, 임프란트에 대한 연구가 꾸준히 이루어지고 있 다1-4.
본 연구는 조선대학교 치과병원에 내원하여 상악동 거상술 및 임프란트를 식립한 환자들에 대한 약 10년간의 추적조사 를 통해 전반적인 임프란트 생존율을 평가하고 치과의사에게 새로운 정보를 제공하는 데 있다.
연구 대상 및 방법
본 연구는 2000년부터 2010년까지 조선대학교 치과병원 에 내원하여 상악동 거상술 및 임프란트 식립을 시행한 404 명의 환자의 1,121개 임프란트를 대상으로 하였다. 환자 분류 는 성비, 연령대, 임프란트 직경과 길이, 전신질환 유무, 골 질, 수직골 높이, 식립한 임프란트의 종류 및 그에 대한 표면 처리 방법, 거상술과 임프란트의 즉시 식립 및 지연 식립의 유 무, 거상술 방법, 골이식재와 차단막의 종류, 상악동 천공 유 무를 기준으로 하였고 각각의 조건에 대한 임프란트 생존율
을 조사하였다.
통계학적 분석을 위해 SPSS version 12.0을 이용하였으 며, P-value가 <0.05일 경우를 통계학적으로 유의한 차이 가 있다고 평가하였다.
연
연구 구결과
상악동 거상술 및 임프란트 식립을 시행한 404명의 환자에 대한 1,121개 임프란트 중 실패 개수는 25개로, 전체 생존율 은 97.8%였다.
남자와 여자에 따른 생존율
성비에 따른 임프란트 생존율을 조사하였다. 1,121개 임프 란트 중 남자 환자에게 식립된 임프란트는 728개였으며 실패 된 임프란트는 14개로 생존율은 98.1%로 집계되었다. 여자 환자에게는 393개의 임프란트가 식립되었으며 생존율은 97.2%로 성비에 따른 임프란트 생존율은 유의한 차이가 없었 다(Table 1).
연령에 따른 임프란트 생존율
식립된 임프란트를 연령에 따라 분석한 결과, 모든 연령대 에서 임프란트 생존율은 매우 우수하였으며 각각 통계적으로 유의한 차이는 없었다(Table 2).
Ⅲ
Ⅱ I
Table 1. Implant survival rate according to gender P
Pllaacceedd iimmppllaannttss ((nn)) FFaaiilleedd iimmppllaannttss ((nn)) SSuurrvviivvaall rraattee ((%%))
Male 728 14 98.1
Female 393 11 97.2
Su-Gwan Kim et al. : The Maxillary Sinus Grafting and Survival Rate of Implants: A 10-year Retrospective Study. Implantology 2010
임프란트의 길이에 따른 생존율
식립된 임프란트 길이는 8mm 이상에서 15mm까지 분포 되었다. 제조사마다 제공되는 임프란트 길이는 다양하여 분 류에서 소수점은 제외하였다. 식립된 임프란트 길이가 표기 되어 있지 않은 unknown 군은 조사에서 제외시켰으며 총 165개, 1개 실패를 확인하였고, 따라서 본 연구에서는 임프란 트 956개, 그 중 실패된 24개 임프란트 만을 대상으로 하였 다. 임프란트 길이에 따른 생존율 또한 모두 우수하였으며 p
값은 0.69로 길이에 따른 생존율의 유의한 차이는 없었다 (Table 3).
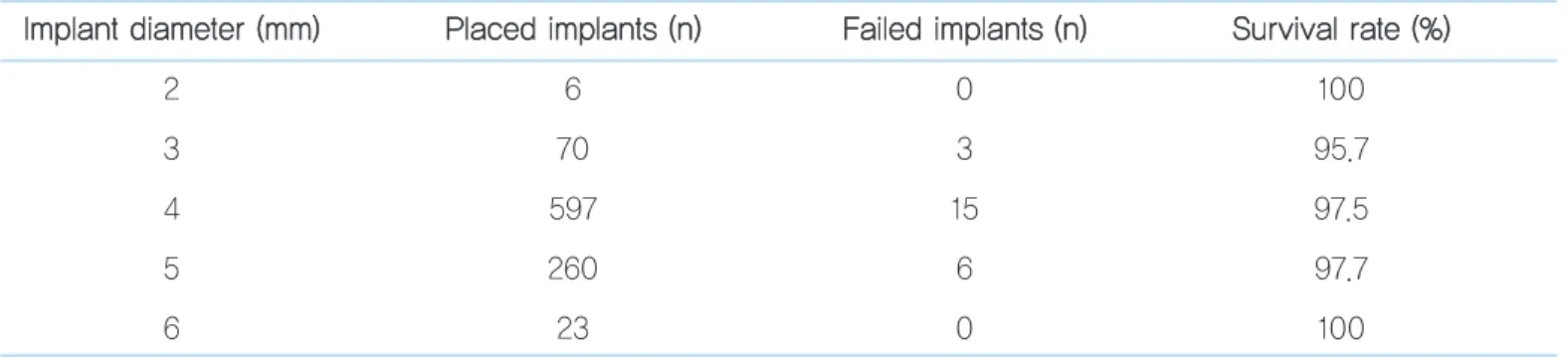
임프란트의 직경에 따른 생존율
식립된 임프란트 직경은 2.8mm부터 시작하여 6mm까지 분포되었다. 제조사마다 제공되는 임프란트 직경은 다양하여 분류에서 소수점은 제외하였다. 식립된 임프란트 직경이 표 기되어 있지 않은 unknown 군은 제외하였고 임프란트 956 Table 2. Implant survival rate according to age distribution
A
Aggee ((yyeeaarrss)) PPllaacceedd iimmppllaannttss ((nn)) FFaaiilleedd iimmppllaannttss ((nn)) SSuurrvviivvaall rraattee ((%%))
20 ~ 29 60 1 98.3
30 ~ 39 82 2 97.6
40 ~ 49 190 3 98.4
50 ~ 59 496 12 97.6
60 ~ 69 249 5 98.0
≧70 44 2 95.5
Su-Gwan Kim et al. : The Maxillary Sinus Grafting and Survival Rate of Implants: A 10-year Retrospective Study. Implantology 2010
Table 3. Implant survival rate according to implant length
IImmppllaanntt lleennggtthh ((mmmm)) PPllaacceedd iimmppllaannttss ((nn)) FFaaiilleedd iimmppllaannttss ((nn)) SSuurrvviivvaall rraattee ((%%))
8 21 0 100
9 49 2 95.9
10 168 3 98.2
11 257 7 97.3
12 65 3 95.4
13 312 7 97.8
14 43 0 100
15 41 2 95.1
개, 실패된 24개 임프란트 만을 대상으로 하였다. 식립된 임 프란트 직경에 따른 분포에서 3mm군의 임프란트가 가장 많 았으며, 직경에 따른 생존율 또한 유의한 차이가 없었다 (Table 4).
Systemic disease
전신질환의 유무와 임프란트 생존율에 대해 조사하였으며 전신질환으로 당뇨, 심혈관질환, 고혈압, 간질환, 신장질환 등을 포함하였다. 고혈압군으로 평균 혈압이 수축기 140mmHg, 이완기 90mmHg 이상인 경우와 항고혈압약을 투약중인 환자를 대상으로 하였으며, 심혈관질환자로는 심장 판막증, 협심증 및 심부전, 다수의 관상동맥질환자를 대상으 로 하였다.
총 404명의 환자 중 전신질환을 가진 환자는 162명이었으 며 식립된 임프란트는 380개였다. 이중 4개가 실패하여 생존 율은 98.7%이었다. 건강한 환자의 임프란트 741개 중 실패는 21개로 생존율은 97.3%이었고 생존율의 유의한 차이는 없었 다.
전신질환 군에서 당뇨 환자 및 심혈관 질환자의 임프란트의 생존율은 100%였다. 고혈압환자에서는 83개 임프란트 중 실 패는 1개였고 생존율은 98.8%였다. 간염, 간경화를 포함한 간질환 환자에서는 25개의 임프란트 중 3개가 실패하였고, 생존율은 88.0%로 기타 질환들과 유의한 차이가 있었다 (Table 5). 그 외 당뇨 및 고혈압을 가진 환자 중 14개의 임프 란트가 식립되었고 실패는 없었으며, 심혈관 질환과 고혈압 을 동시에 가진 환자에서도 12개 임프란트 중 실패는 없었다.
Table 4. Survival rate according to implant diameter
IImmppllaanntt ddiiaammeetteerr ((mmmm)) PPllaacceedd iimmppllaannttss ((nn)) FFaaiilleedd iimmppllaannttss ((nn)) SSuurrvviivvaall rraattee ((%%))
2 6 0 100
3 70 3 95.7
4 597 15 97.5
5 260 6 97.7
6 23 0 100
Su-Gwan Kim et al. : The Maxillary Sinus Grafting and Survival Rate of Implants: A 10-year Retrospective Study. Implantology 2010
Table 5. Implant survival rate in patients with systemic diseases D
Diiaabbeetteess CCaarrddiioovvaassccuullaarr ddiisseeaassee HHyyppeerrtteennssiioonn LLiivveerr ddiisseeaassee
The number of placed implants (n) 27 18 83 25
The number of failed implants (n) 0 0 1 3
Su-Gwan Kim et al. : The Maxillary Sinus Grafting and Survival Rate of Implants: A 10-year Retrospective Study. Implantology 2010
Bone quality
골질의 평가는 술자마다 경향이 달라 평가법이 다소 주관적 이나 본 연구에서는 CT 촬영을 한 경우 V Implant program 을 평가법에 이용하였고, 그 외 값은 기록에 의해 분석을 하였 다. 이때 type II에 해당하는 환자의 임프란트는 37개로 이중 1개가 실패하였다. type III에 해당하는 경우 690개의 임프란 트가 상악동 거상술 후 식립되었으며, 이중 13개가 실패하여 임프란트 생존율은 98.1%를 기록하였다. 골질 type IV에서 는 394개의 임프란트가 식립되었으며 이중 11개의 임프란트 가 실패하여 생존율은 97.2%로 분석되었다. type III와 IV간 의 유의한 차이는 발견되지 않았으며 골질에 따른 생존율의 유의한 차이는 없었다(Table 6).
Vertical bone height (bone quantitiy)
잔존골 수직 높이에 따른 임프란트 생존율을 조사하였다.
환자의 파노라마 사진을 기준으로 하였고 sinus floor로부터 가장 낮은 crestal bone height을 기준으로 하였으며 파노라 마 확대율 110%를 감안하였다. 잔존골은 2mm 미만, 2~4mm, 4~6mm, 6~10mm, 10mm 초과로 그룹을 형성하 였다(Table 7).
임프란트 생존율은 6~10mm의 잔존골 그룹을 제외하고 모두 높았으며 이 그룹의 임프란트 생존율은 p값 0.013으로 유의하게 낮았다. 실패 원인으로 임프란트 초기 고정 실패가 7개, 상악동 천공으로 인한 경우가 5개, 만성 임프란트 주위 염이 1개였다. 실패한 13개 임프란트 중 8개의 임프란트는 lateral window technique으로 2 stage하에 식립한 경우였 으며, 그 외 lateral window technique과 1 stage으로 식립한 경우는 3개, osteotome을 사용하여 1 stage로 식립한 경우가 2개였다.
Table 6. Implant survival rate according to bone quality B
Boonnee qquuaalliittyy TThhee nnuummbbeerr ooff ppllaacceedd TThhee nnuummbbeerr ooff ffaaiilleedd SSuurrvviivvaall rraattee iimmppllaannttss ((nn)) iimmppllaannttss ((nn)) ((%%))
Type II 37 1 97.3
Type III 690 13 98.1
Type IV 394 11 97.2
Su-Gwan Kim et al. : The Maxillary Sinus Grafting and Survival Rate of Implants: A 10-year Retrospective Study. Implantology 2010
Table 7. Implant survival rate according to vertical bone height V
Veerrttiiccaall bboonnee hheeiigghhtt ((mmmm)) IImmppllaanntt
<
< 22 22--44 44--66 66--1100 1100 << The number of placed implants (n) 234 348 229 264 46
The number of failed implants (n) 5 4 3 13 0
Survival rate (%) 97.9 98.9 98.7 95.1* 100
Type of implant
임프란트의 종류에 따른 생존율을 조사하였다. 본원에서 식립한 임프란트 종류는 9가지였다. 대부분 임프란트의 생존 율은 우수하였고, ITI의 생존율도 92.3%로 나머지 임프란트 와 유의한 차이를 보이지 않았다(Table 8).
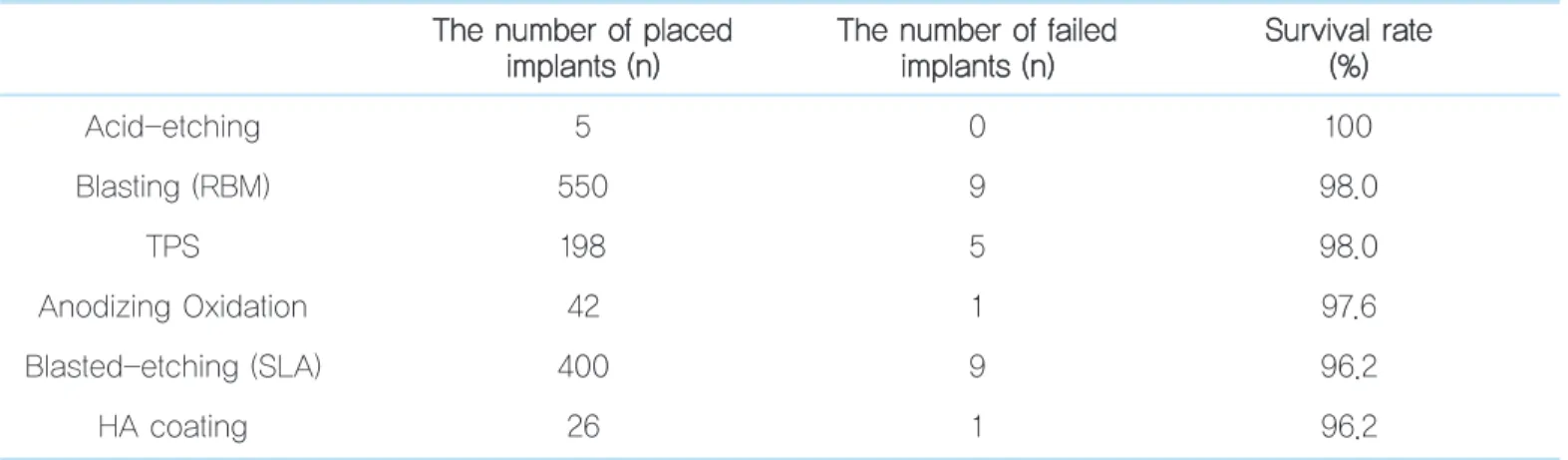
Surface treatment of implant
각각의 임프란트 생존율을 추적 조사하였다. 분석 결과, 대 부분의 조건에서 임프란트 생존율은 매우 우수하였으며 95%
신뢰수준에서 각각 유의한 차이는 없었다(Table 9).
Table 8. Implant survival rate according to types of implants T
Thhee nnuummbbeerr ooff ppllaacceedd TThhee nnuummbbeerr ooff ffaaiilleedd SSuurrvviivvaall rraattee iimmppllaannttss ((nn)) iimmppllaannttss ((nn)) ((%%))
Dentis 71 0 100
Branemark 28 0 100
Frialit 22 0 100
Osstem 251 3 98.8
Zimmer 47 1 97.9
Xive 46 1 97.8
Astra 84 2 97.6
3i 507 13 97.4
ITI 65 5 92.3
Su-Gwan Kim et al. : The Maxillary Sinus Grafting and Survival Rate of Implants: A 10-year Retrospective Study. Implantology 2010
Table 9. Implant survival rate according to surface treatment methods T
Thhee nnuummbbeerr ooff ppllaacceedd TThhee nnuummbbeerr ooff ffaaiilleedd SSuurrvviivvaall rraattee iimmppllaannttss ((nn)) iimmppllaannttss ((nn)) ((%%))
Acid-etching 5 0 100
Blasting (RBM) 550 9 98.0
TPS 198 5 98.0
Anodizing Oxidation 42 1 97.6
Blasted-etching (SLA) 400 9 96.2
HA coating 26 1 96.2
Su-Gwan Kim et al. : The Maxillary Sinus Grafting and Survival Rate of Implants: A 10-year Retrospective Study. Implantology 2010
Graft materials
404명의 환자 중 골이식을 시행하지 않은 3명의 환자 4개 의 임프란트를 제외하고 조사하였다. 자가골과 동종골인 Tutoplast (Tutoplast Spongiosa Mikrochip, Puros,
Zimmer Dental, Carlsbad, CA, USA), 이종골인 Bio-Oss (Geistlich, Wolhusen, Switzerland), 합성골을 조사하였고 최근 도입된 자가치아 회분말 골이식재 (AutoBT, Seoul, Korea)도 포함하였다. 단일 골이식재를 사용한 경우부터 분
Table 10. Implant survival rate according to single bone graft T
Thhee nnuummbbeerr ooff ppllaacceedd TThhee nnuummbbeerr ooff ffaaiilleedd SSuurrvviivvaall rraattee iimmppllaannttss ((nn)) iimmppllaannttss ((nn)) ((%%))
Tooth ash 5 0 100
Tutoplast 188 2 98.9
Synthetic bone 49 1 98.0
Bio-Oss 398 11 97.2
Autobone 60 2 96.7
Su-Gwan Kim et al. : The Maxillary Sinus Grafting and Survival Rate of Implants: A 10-year Retrospective Study. Implantology 2010
Table 11. Implant survival rate according to combined bone graft T
Thhee nnuummbbeerr ooff ppllaacceedd TThhee nnuummbbeerr ooff ffaaiilleedd SSuurrvviivvaall rraattee iimmppllaannttss ((nn)) iimmppllaannttss ((nn)) ((%%))
1+4 25 0 100
1+5 4 0 100
2+4 7 0 100
3+5 23 0 100
1+3+4 11 0 100
1+3+5 25 0 100
3+4+5 1 0 100
1+2+3+4 2 0 100
1+3+4+5 12 0 100
3+4 163 3 98.2
1+3 104 4 96.2
4+5 44 2 95.5
1. Autogenous bone, 2. Tooth ash, 3. Bio-Oss, 4. Tutoplast, 5. Synthetic bone.
석하였다(Table 10). Bio-Oss는 총 398개의 임프란트 식립 에 이용되어 가장 많은 비율을 보였으며 97.2%의 생존율을 보였다. 자가치아 회분말 골이식재의 단일 사용은 총 5개의 임프란트 식립에 이용되었으며 아직 실패는 보고되지 않았으 며, 모든 이식재는 거상술 및 임프란트 식립에 우수한 생존율 을 보였다. 합성골인 synthetic bone으로는 OsteonTM (GENOSS, Suwon, Korea)의 사용이 가장 많았다.
골이식재를 혼합 사용한 경우에 실패된 임프란트는 자가골 과 Bio-oss를 혼합한 경우로 104개 임프란트 중 4개가 실패 하였으며, 다음은 Bio-Oss와 Tutoplast를 혼합한 경우로 163개 임프란트 중 3개가 실패하였다. Tutoplast와 syn- thetic bone을 혼합 사용한 경우 44개 임프란트 중 2개가 실 패하였다(Table 11).
Sinus approach technique
Osteotome technique으로 상악동 거상을 한 307개의 임
프란트 중 2개의 임프란트에서 실패를 보였다. 814개의 임프 란트가 Lateral window technique으로 식립되었으며 23개 의 실패를 보여 97.2%의 생존율을 보였다. 생존율은 모두 높 았으나 osteotome technique은 통계학적으로 유의하게 생 존율이 높은 것으로 분석되었다(Table 12).
Implant surgery stage
상악동 거상술과 임프란트 식립을 동시에 시행하는 술식을 immediate implantation (1 stage), 거상술 후 임프란트 식 립을 하는 경우를 delayed implantation (2 stage)라고 한 다. 일반적인 1 stage와 2 stage의 선택 기준은 4mm의 잔존 골량으로 알려져 있으나2이에 영향을 미치는 요소는 골량 뿐 만 아니라 골질 및 초기 고정을 얻을 만한 임프란트 직경과 길 이 등 실제 임프란트 식립시에는 술자의 주관적인 요소가 많 이 개입된다3. 따라서 Osteotome technique을 시행할 경우 대부분 1 stage로 식립하지만 드문 경우 2 stage 중에서도 부
Table 12. Implant survival rate according to sinus floor elevation T
Thhee nnuummbbeerr ooff ppllaacceedd TThhee nnuummbbeerr ooff ffaaiilleedd SSuurrvviivvaall rraattee iimmppllaannttss ((nn)) iimmppllaannttss ((nn)) ((%%))
Osteotome technique 307 2 99.4*
Lateral window technique 814 23 97.2
*Significantly different from lateral window technique (P <0.05, ANOVA).
Su-Gwan Kim et al. : The Maxillary Sinus Grafting and Survival Rate of Implants: A 10-year Retrospective Study. Implantology 2010
Table 13. Implant survival rate according to stages T
Thhee nnuummbbeerr ooff ppllaacceedd TThhee nnuummbbeerr ooff ffaaiilleedd SSuurrvviivvaall rraattee iimmppllaannttss ((nn)) iimmppllaannttss ((nn)) ((%%))
1 stage 538 13 97.6
2 stage 583 12 97.9
Su-Gwan Kim et al. : The Maxillary Sinus Grafting and Survival Rate of Implants: A 10-year Retrospective Study. Implantology 2010
분적으로 osteotome technique을 사용하는 경우가 있어 크 게 stage로 분류하여 이에 따른 임프란트 생존율을 분석해 보 았다(Table 13).
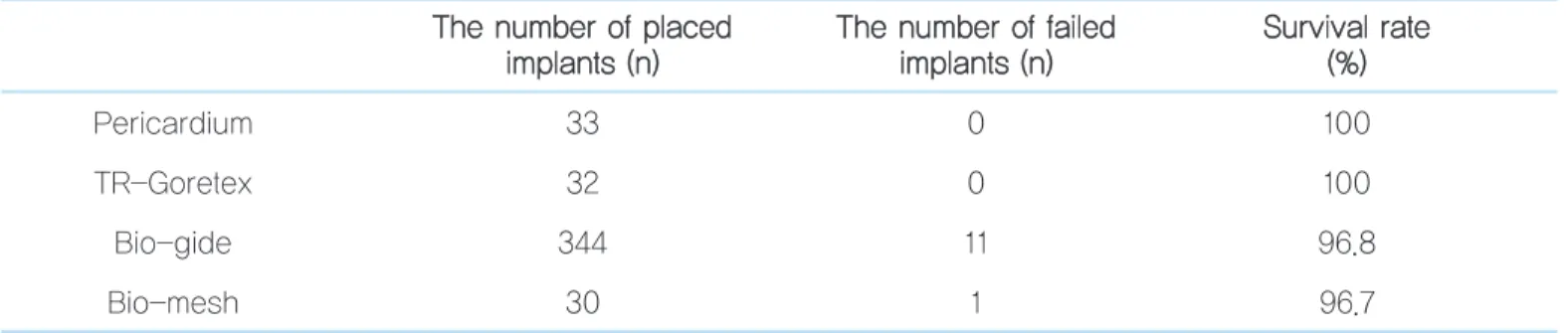
Membrane on lateral wall
Lateral window technique으로 상악동 거상술 시행시 이 때 쓰인 membrane의 유무에 따른 임프란트 생존율 및 membrane 종류에 따른 생존율을 조사하였다. Lateral window technique으로 접근한 환자 중 membrane을 사용 한 130명의 환자는 생존율이 97.5%를 보였으며, membrane 을 사용하지 않은 환자에서는 생존율이 97.6%로 사용한 군에 대하여 유의한 차이는 나타나지 않았다.
본원에서 사용한 membrane은 Bio-gide (Geistlich Pharma Ag., Wolhusen, Switzerland), pericardium (Tutoplast PericardiumⓇ, Tutogen Medical GmbH), Bio-mesh (Samyang, Seoul, Korea), TR-Goretex membrane (W. L. Gore & Associates, CA, USA) 등으로 크게 4종류로 분류되었다. 각각의 생존율을 조사하였다 (Table 14).
Bio-gide를 사용한 경우 11개의 실패한 임프란트 중에서 1 개의 상악동 천공, 10개의 임프란트 초기 고정 실패가 원인으
로, membrane의 노출과 그로인한 감염과는 거리가 멀었다.
Bio-mesh를 사용한 경우 1개의 실패한 임프란트에서도 초 기 고정 실패가 원인이었다.
그 외 membrane을 두 종류 이상 사용한 경우도 있었는데, 5개의 임프란트에서 Bio-gide와 Pericardium을 사용하였 고, 4개의 임프란트는 Bio-gide와 Gore-tex, 2개의 임프란 트에서 Pericardium과 Bio-mesh를 사용하였으며 모두 실 패한 경우는 없었다.
Schneiderian membrane perforation
상악동 천공은 상악동 거상술에서 가장 흔한 합병증이다.
천공에 따른 이식재의 이탈 및 감염의 가능성은 임프란트의 성패를 좌우하기도 한다. 천공 시 대처 방안으로 여러 가지 방 법이 추천되고는 있으나 아직 임프란트 예후와 무관하다 할 수는 없다. 천공 유무에 따른 임프란트 생존율을 조사해 보았 다(Table 15).
상악동 거상술 시 상악동 점막이 천공된 경우 생존율은 89.8%로, 상악동 점막이 천공되지 않고 안전하게 임프란트 가 식립된 경우의 생존율인 98.7%와 통계학적으로 유의한 차 이를 보였다. 실제로 실패된 25개의 임프란트 중 상악동 점막 의 천공으로 인한 실패가 9증례에서 발생되어, 임프란트 식립 의 실패에 상악동 점막의 천공 여부가 중요함을 알 수 있었다.
Table 14. Implant survival rate according to the use of membrane T
Thhee nnuummbbeerr ooff ppllaacceedd TThhee nnuummbbeerr ooff ffaaiilleedd SSuurrvviivvaall rraattee iimmppllaannttss ((nn)) iimmppllaannttss ((nn)) ((%%))
Pericardium 33 0 100
TR-Goretex 32 0 100
Bio-gide 344 11 96.8
Bio-mesh 30 1 96.7
Causes of failed implant
실패로 분류된 25개 임프란트의 실패 원인에 대해 분석하 였다. 대표적인 실패의 원인 요소에는 상악동 점막의 천공, 초 기 고정 실패, 임프란트 주위염의 처치 실패, 차단막의 노출 등이 있었다(Table 16).
실패 원인 중 초기 감염 등은 술자가 조절이 가능하며 fol- low up 기간 내 해결할 수 있어 임프란트 실패로 이어지지 않 았다. 그러나 오랜 기간 동안의 만성 임프란트 주위염은 환자 교육과 오랜 기간 follow up의 어려움으로 임프란트 실패로 이어지는 경우가 있었다. 이중 상악동 점막의 천공이 가장 높 은 비율을 차지했으며, 이는 일단 천공이 되면 임프란트 식립 제한, 골이식재의 유출, 상악동염 등을 유발하며 술자의 처치 에도 불구하고 조절이 쉽지 않음을 의미한다. 그리고 초기 고 정의 실패도 임프란트의 예후를 예측하기가 어려워 실패로 이어지는 경우가 많았다.
총괄 및 고찰
Sinus graft와 임프란트 식립에 대해 많은 연구가 있어 왔 고 본 연구에서도 지금까지 발표된 여러 저널들과 비슷한 경 향을 후향적 조사를 통해 관찰할 수 있었다. 여러 전신질환을 가진 환자에 대해서도 임프란트 성공률은 크게 뒤지지 않는 데, 이는 이미 밝혀진 것처럼 "controlled patient" 때문인 것 으로 생각된다. 그러나 특히 전신질환 중 간 질환자에서 실패 율이 상대적으로 더 높았다.
골질에 대한 임프란트 성공률은 기존 연구와 크게 다르지 않다. Molly5는 골질 자체는 임프란트 초기 고정을 결정하는 중요한 요소이나 골질과 임프란트 성공률은 크게 차이가 없 다고 하였다. Blomqvist 등6도 골질에 따라 임프란트 성공률
Ⅳ
Table 16. Causes of failed implant
T
Thhee nnuummbbeerr ooff ffaaiilleedd iimmppllaannttss ((nn)) FFaaiilluurree rraattee ((%%))
Perforation 9 36
Poor primary stability 8 32
Uncontrolled chronic peri-implantitis 6 24
Membrane exposure 2 8
Su-Gwan Kim et al. : The Maxillary Sinus Grafting and Survival Rate of Implants: A 10-year Retrospective Study. Implantology 2010
Table 15. Implant survival rate according to schneiderian membrane perforation P
Peerrffoorraattiioonn TThhee nnuummbbeerr ooff ppllaacceedd TThhee nnuummbbeerr ooff ffaaiilleedd SSuurrvviivvaall rraattee iimmppllaannttss ((nn)) iimmppllaannttss ((nn)) ((%%))
Yes 88 9 89.8
no 1033 14 98.7
Su-Gwan Kim et al. : The Maxillary Sinus Grafting and Survival Rate of Implants: A 10-year Retrospective Study. Implantology 2010
을 평가하는 것은 어려우며 골질에 따른 임프란트 성공률에 통계적 유의한 차이는 없다고 보고하였다.
임프란트 표면처리법과 관련하여 임프란트 성공률에 대해 많은 논문이 있었으며 Braceras 등7은 표면처리법에 따라 임 프란트 주위 골 침착이 달라질 수 있다고 주장하였다. Ion- implant와 sand-blasted and acid-etched (SLA), 그리고 machined surface 처리법에 대해 SLA에서 bone과 implant 사이 가장 많은 골량이 관찰되었으며 machined surface에서는 그 값의 0.4 밖에 관찰되지 않았다고 보고하 였다. Chiesa 등8은 임프란트 표면처리 실험에서 특별한 처 치를 시행하지 않은 대조군 임프란트도 골유착이 우수하였으 나 chemical-etching을 시행한 실험군 임프란트에서 좀 더 우수한 골유착을 보였다. 대부분의 연구에서 표면처리법에 따라 임프란트 주위 골 면적이 넓어짐이 입증되었으나 이것 이 임프란트 성공률 전체를 좌우하는 것은 아닐 것으로 생각 되며 임프란트 성공률에 대한 후향적 연구에서 이 같은 통계 값은 의미 있을 수 있다.
골이식재에 대한 연구 값은 기존 연구와 비슷하다9. 골이식 재의 생존율은 모든 종류에서 높았다. Seol 등10은 동종골인 Tutoplast는 human mineralized cancellous bone으로 높 은 다공성 때문에 표면적이 넓어 빠른 치유를 보인다고 밝혔 다. 또한 Kim 등11,12과 Bae 등13은 상악동 골 이식술에 자가골
과 이종골인 Bio-Oss, 합성골인 Osteon에 대한 단독 또는 혼합사용에 대한 골의 성숙도에 대해 연구하였으며, 합성골 인 Osteon의 단독 사용 시에도 우수한 치유과정을 보이므로 동종골과 이종골의 사용 간에 유의한 차이성이 없다고 보고 하였다. Hürzeler 등14도 Bio-Oss와 Interpore200의 1:1 혼 합 사용, 자가골과 Interpore200의 1:3 혼합 사용, 자가골과 Interpore200의 1:1 혼합 사용에 대해 연구하였으며, 모든 경우에 식립된 임프란트에서 성공적인 골유착을 보였다고 보
고하였다15,16. 자가골, 동종골, 합성골의 자체의 치유과정에
유의한 차이는 없으나 Hatano 등17은 상악동 골이식술 후 repneumatization이 2~3년 내에 다시 시작되므로 골 흡수 속도를 줄일 수 있도록 자가골과 골이식재를 동시에 사용해 야 한다고 하였다18.
Osteotome technique은 Summers3에 의해 시작되어 그 동안 많은 연구가 진행되었다. 이 술식은 골질이 낮은 부위에 서 골을 압박하는 힘으로 초기 고정을 좀 더 쉽게 얻을 수 있 으며 거상량을 최대한 4~5mm까지 얻을 수 있어 비교적 안 전하고 간단한 술식으로 소개되었다. 잔존 골량이 적어 거상 량이 많을 경우 lateral window technique을 사용하게 되는 데 이때 immediate 또는 delayed implantation을 하는 기 준에 대해 Zitzmann 등2은 아래와 같이 보고한 바 있다 (Table 17).
Table 17. Indication criteria for the different methods of sinus floor elevation R
Reessiidduuaall bboonnee hheeiigghhtt MMeetthhooddss TTiimmiinngg ooff ppllaacceemmeenntt
≤ 4mm Two-step lateral window technique Second step 6-8month later 4-6mm One-step lateral window technique Simultaneous (one-step)
≥ 6mm Osteotome technique Simultaneous (one-step)
이에 따르면 vertical bone height가 4mm 이하라면 2 stage로 하는 것이 추천되며, 잔존골이 6mm 이상인 경우 osteotome technique의 예후가 좋다. 잔존골이 4~6mm 일 경우는 lateral window technique로 하되 1 stage 임프란트 식립이 가능하다. Zitzmann 등2은 osteotome technique과 lateral window technique과의 예후 차이에 대해, osteotome technique의 임프란트 성공률이 유의하게 높으 며 특히 type IV 골질에 있어서 더욱 우수하였다고 보고하였 다19,20. 또한 1 stage와 2 stage에 따른 임프란트 성공률은 하 중 부하 후 1년까지 통계적 유의성이 없이 모두 우수하였으나 더 긴 추적조사가 필요하다고 보고하였다.
Jurisic 등21의 연구에서는 80개의 임프란트에 대하여 vertical bone height에 따라 osteotome과 lateral window technique으로 식립하였을 때의 성공률을 조사하였는데, 이 때 osteotome 방식으로 임프란트를 식립할 수 있는 잔존골 의 양은 최소 5mm라고 하였으며 잔존골의 양에 따라 tech- nique을 분류하였다22.
본 연구에서는 잔존골에 따른 상악동 접근법은 위의 연구와 비슷하였으며, 임프란트 생존율은 approach technique에 관계없이 모두 우수하였다.
최근에는 골이식재 사용 없이 osteotome technique으로 상악동 거상술을 시행할 수 있다는 연구도 발표되고 있으며 Nedir 등23은 골이식술 없이 거상할 수 있는 양은 5.1±
1.3mm이었으며 이 공간은 새로 형성된 골로 치환된다고 보 고하였다. 그러나 이 경우에서 immediate implant 식립은 초기 고정이 충분히 얻어질 수 있을 때로 한정되어 이에 대한 더 많은 연구가 필요하다고 하였다. Thor 등24도 골이식술을 하지 않고 점막만 올리는 방법은 골이식재의 실패에 대한 대 안이 될 수 있으며 submerged type으로 식립한다면 잔존 수 직골량의 최소한의 한계는 정해지지 않고 임프란트 상방으로 부터 2~5mm 내외의 골이 만들어질 수 있다고 하였다. 임프 란트 직경은 5mm 이상이어야 하며 성공률은 97.7%였다고 보고하였다.
차단막의 사용에 대해서 Dergin 등25, Hockers 등26도 본 연구와 마찬가지로 그 종류에 관계없이 임프란트 생존율은 높다고 보고하였다. 그리고 e-PTFE와 collagen membrane 인 Ossix, collagen barrier인 Bio-gide의 치유과정에 대한 유의한 차이는 없었으며 e-PTFE 차단막 노출이 41.2%로 다 소 높았으나27, 이것은 환자의 치유능력이나 술자의 피판에 대한 처치가 더 많이 좌우된다고 보고하였다.
Ardekian 등28은 schneiderian membrane의 천공에 대 해서는 임프란트 성공률과 크게 상관이 없다는 연구가 많으 며 상악동 천공에 가장 중요한 요인으로 잔존골의 높이를 꼽 을 수 있다고 하였다. 그의 연구에 따르면 perforation group의 임프란트 성공률은 94.4% 이었으며 non-perfo- ration group의 성공률은 93.9%로 유의한 차이가 없다고 하 였다. 본 연구에서는 vertical bone height에 따른 임프란트 생존율은 유의한 차이가 없었으며 특히 6~10mm 그룹에서 유의하게 생존율이 낮았다. 13개 실패한 임프란트 중 8개의 임프란트는 lateral window technique으로 2 stage하에 식 립한 경우로, 이것은 위에서 밝힌 것처럼 환자의 wound healing이나 술자의 technique 등 조절 외의 요인이 작용했 을 가능성이 크다18.
결론
지난 10년간의 상악동 골이식술을 시행한 임프란트에 대한 후향적 연구에서 어떤 술식과 조건에서건 대부분의 임프란트 생존율은 매우 우수하였으며 안전한 술식이라는 점이 밝혀졌 다. 향후 상악동 거상술후 사용한 골이식재의 종류, 상악동 거 상술후 골이식술을 시행하지 않은 경우의 임프란트의 예후 등에 대한 연구가 더욱 진행되어야 할 것으로 생각된다.
Ⅴ
참고문헌
1. Boyne PJ, James RA. Grafting of the Maxillary sinus floor with autoge- nous marrow and bone. J Oral Surg. 1980; 38: 613-616.
2. Zitzmann NU, Scharer P. Sinus elevation procedure in the resorbed pos- terior maxilla. Comparison of the crestal and lateral approaches. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998; 85: 8-17.
3. Summers RB. A new concept in maxillary implant surgery: the osteotome technique. Compend Contin Educ Dent. 1994; 15: 152-162.
4. Friedmann A, Dard M, Kleber BM, et al. Ridge augmentation and max- illary sinus grafting with a biphasic calcium phosphate: histologic and histomorphometric observations. Clin Oral Implants Res. 2009; 20:
708-714.
5. Molly L. Bone density and primary stability in implant therapy. Clin Oral Implants Res. 2006; 17: 124-135.
6. Blomqvist JE, Alberius P, Isaksson S, et al. Importance of bone graft quality for implant integration after maxillary sinus reconstruction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998; 86: 268-274.
7. Braceras I, De Maeztu MA, Alava JI, et al. In vivo low-density bone apposition on different implant surface materials. Int J Oral Maxillofac Surg. 2009; 38: 274-278.
8. Chiesa R, Giavaresi G, Fini M, et al. In vitro and in vivo performance of a novel surface treatment to enhance osseointegration of endosseous implants. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;
103: 745-756.
9. Schwartz-Arad D, Herzberg R, Dolev E. The prevalence of surgical cmplications of the sinus graft procedure and their impact in implant survival. J Periodontol. 2004; 75: 511-516.
10. Seol KY, Kim SG, Kim HK, et al. Effects of decortication in the treat- ment of bone defect around particulate dentin-coated implants: an experimental pilot study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 108: 529-536.
11. Kim YK, Yun PY, Kim SG, et al. Analysis of the healing process in sinus bone grafting using various grafting materials. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 107: 204-211.
12. Kim YK, Yun PY, Lim SC, et al. Clinical evaluations of OSTEON as a new alloplastic material in sinus bone grafting and its effect on bone healing. J Biomed Mater Res B Appl Biomater. 2008; 86: 270-277.
13. Bae JH, Kim YK, Kim SG, et al. Sinus bone graft using new alloplastic bone graft material (Osteon)-II: clinical evaluation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010; 109: e14-20.
14. Hürzeler MB, Quiñones CR, Kirsch A, et al. Maxillary sinus augmenta- tion using different grafting materials and dental implants in monkeys.
Part III. Evaluation of autogenous bone combined with porous hydrox- yapatite. Clin Oral Implants Res. 1997; 8: 401-411.
15. Friedmann A, Dard M, Kleber BM, et al. Ridge augmentation and max- illary sinus grafting with a biphasic calcium phosphate: histologic and histomorphometric observations. Clin Oral Implants Res. 2009; 20:
708-714.
16. Mardas N, Kostopoulos L, Stavropoulos A, et al. Osteogenesis by guid- ed tissue regeneration and demineralized bone matrix. J Clin Periodontol. 2003; 30: 176-183.
17. Hatano N, Shimizu Y, Ooya K. A clinical long-term radiographic evalu- ation of graft height changes after maxillary sinus floor augmentation with 2:1 autogenous bone/xenograft mixture and simultaneous place- ment of dental implants. Clin Oral Implants Res. 2004; 15: 339-345.
18. Barone A, Santini S, Sbordone L, et al. A clinical study of the outcomes and complications associated with maxillary sinus augmentation. Int J Oral Maxillofac Implants. 2006; 31: 81-85.
19. Jaffin NU, Naef R, Schärer P. Resorbable versus non-resorbable mem- branes in combination with Bio-Oss for guided bone regeneration. Int J Oral Maxillofac Implants. 1997; 12: 100-109.
20. Hahn J. Clinical uses of osteotomes. J Oral Implantol. 1999; 25: 23-29.
21. Jurisic M, Markovic A, Radulovic M, et al. Maxillary sinus floor aug- mentation: comparing osteotome with lateral window immediate and delayed implant placements. An interim report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 106: 820-827.
22. Jensen OT. Treatment planning for sinus grafts. In: Jensen OT, editor.
The sinus bone graft. Carol Stream (IL): Quintessence; 1999. p. 49-68.
23. Nedir R, Nurdin N, Szmukler-Moncler S, et al. Osteotome sinus floor elevation technique without grafting material and immediate implant placement in atrophic posterior maxilla: report of 2 cases. J Oral Maxillofac Surg. 2009; 67: 1098-1103.
24. Thor A, Sennerby L, Hirsch JM, et al. Bone formation at the maxillary sinus floor following simultaneous elevation of the mucosal lining and implant installation without graft material: an evaluation of 20 patients treated with 44 Astra Tech implants. J Oral Maxillofac Surg. 2007; 65:
64-72.
25. Dergin G, Gurler G, Guvercin M, et al. Vertical alveolar bone distrac- tion with polytetrafluoroethylene membrane for implant application: A
technical note. J Oral Maxillofac Surg. 2007; 65: 1050-1054.
26. Hockers T, Abensur D, Valentini P, et al. The combined use of biore- sorbable membranes and xenografts or autografts in the treatment of bone defects around implants. A study in beagle dogs. Clin Oral Implants Res. 1999; 10: 487-498.
27. Moses O, Pitaru S, Artzi Z, et al. Healing of dehiscence-type defects in implants placed together with different barrier membranes: a compara- tive clinical study. Clin Oral Implants Res. 2005; 16: 210-219.
28. Ardekian L, Oved-Peleg E, Mactei EE, et al. The clinical significance of sinus membrane perforation during augmentation of the maxillary sinus.
J Oral Maxillofac Surg. 2006; 64: 277-282.
교신저자 : 김수관
우편번호 (501-759) 광주광역시 동구 서석동 375 조선대학교 치의학전문대학원 구강악안면외과학교실 Tel : 82-62-220-3819
Fax : 82-62-228-7316 E-mail : [email protected] 원고접수일 : 2010년 5월 10일 게재확정일 : 2010년 5월 18일
Reprint requests : Su-Gwan Kim, DDS, PhD
Department of Oral and Maxillofacial Surgery, School of Dentistry, Chosun University, 375, Seosuk-Dong, Dong-Gu, Gwangju, 501-759, Republic of Korea
Tel : 82-62-220-3819 Fax : 82-62-228-7316 E-mail : [email protected]
Received for publication : May 10, 2010 Accepted for publication : May 18, 2010