112 Received: April 21, 2010, Accepted for Publication: June 5, 2010
*Corresponding author: Myung Ho Jeong, 501-757, The Heart Research Center, Chonnam National University Hospital, Phone: +82-62-220-6243, FAX:
+82-62-228-7174, E-mail: [email protected] Chonnam Medical Journal
Vol. 46, No. 2, pp. 112∼116 DOI: 10.4068/cmj.2010.46.2.112
Successful Management of Spontaneous Dissection with Spasm in both Coronary Arteries
Seon Gyu Choi1, Myung Ho Jeong2*, Seung Wook Bak1, Jin Woo Park1, Seung Jin Jeong1, Young Joon Hong2, Ju Han Kim2, Doo Sun Sim2, Young Keun Ahn2 and Jung Chaee Kang2
1Yeosu Chonnam Hospital, Yeosu, 2The Heart Center of Chonnam National University Hospital, Gwangju, Korea
Spontaneous coronary artery dissection (SCAD) is a rare cause of acute coronary syndrome. SCAD frequently occurs in young women during the peripartal period. There are few reports of SCAD associated with vasospasm. We report a case of a 36-year-old man who presented at our institution with SCAD with spasm. He presented with continuous chest pain for 1 hour. Initial EKG showed pathologic Q wave and ST elevation in lead II, III, and aVF. Emergent coronary angiography (CAG) revealed diffuse spastic narrowing of the left anterior descending coronary artery (LAD) and right coronary artery. On follow-up CAG, spontaneous type B dissection of the proximal LAD extending to the left main and middle LAD were detected. We decided to treat with medical therapy because he had no chest pain. Three days later, patient complained of severe chest pain. Emergency CAG revealed dissection in the left main to middle LAD and proximal left circumflex artery (LCx) with poor distal flow and spasm in the distal LAD. We performed percutaneous coronary intervention for SCAD in the LAD. The follow-up CAG performed 6 months later showed patent LAD stents. This case illustrates the successful management of SCAD that developed in both the culprit and non-culprit arteries of acute myocardial infarction associated with vasospasm.
Key Words: Coronary artery disease; Dissection; Spasm
Introduction
Spontaneous coronary artery dissection (SCAD) is a rare but important cause of acute coronary syndrome.
Spontaneous coronary artery dissection is the separation of the layers of the arterial wall, making a false lumen.
The true lumen can be compromised by the expansion of hematoma in the false lumen, which causes acute coronary syndrome.1 The first case report of SCAD was
in 1931.2 Many cases have been diagnosed by autopsy, because SCAD presented as sudden death. In one series, 75% of cases occurred in women, half of which were associated with the postpartum state.3
The overall incidence of SCAD in coronary artery angiography ranges from 0.28% to 1.1%.4 Seventy percent of SCAD occurs in women, 30% of which is associated with a postpartum state.3 The most common involved location of the coronary artery is the left anterior descending artery, which accounts for over 60%. There are a few reports about SCAD associated with vasospasm.4
We report a case of SCAD that developed in both
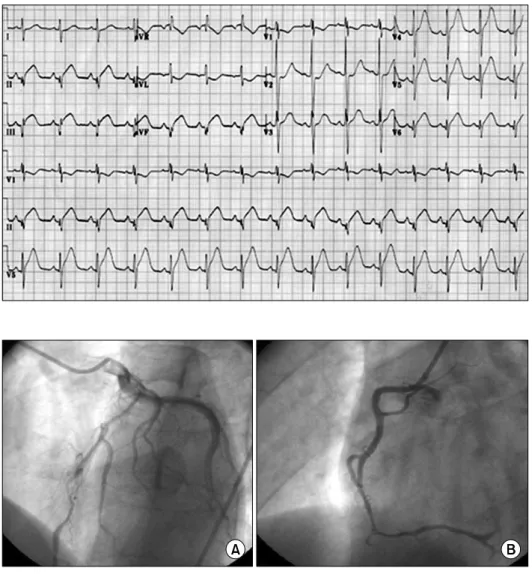
Fig. 1. The ECG showed Q wave with ST-segment elevation in II, III, and aVF.
Fig. 2. The CAG revealed diffuse spastic narrowing of the LAD (A) and RCA (B) (CAG, coronary angiography;
LAD, left anterior descending coron- ary artery; RCA, right coronary artery).
the culprit and non-culprit arteries of acute myocardial infarction associated with vasospasm.
Case Report
A 36-year-old man presented with continuous chest pain for 1 hour. He had been treated in the nephrology department for an acute renal infarction. No thrombotic or embolic source was found on trans-esophageal echo- cardiography, abdominal CT angiography (CTA), or serologic tests including protein C, protein S, anti- phospholipid antibody, and anti-nuclear antibody. His initial EKG showed pathologic Q wave and ST elevation in lead II, III, and aVF (Fig. 1). The levels of cardiac enzymes were elevated: creatine kinase (CK) was 1537
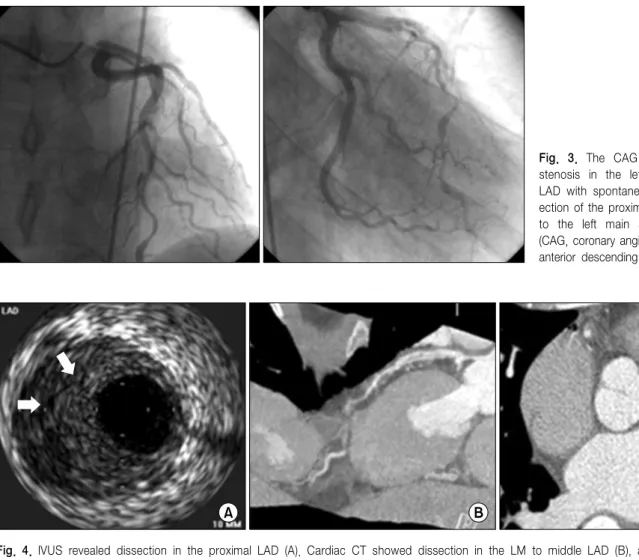
U/L (35∼172), CK-MB was 36.6 U/L (2.3∼9.5), and troponin-I was 0.58 ng/mL (0-0.05). Emergent coronary angiography (CAG) revealed diffuse spastic narrowing of the left anterior descending coronary artery (LAD) and right coronary artery (RCA), but no significant stenosis was detected (Fig. 2). There was no regional wall motion abnormality and his ejection fraction was 69.8% on echocardiography. On the follow-up coronary angiogram, diffuse stenosis in the left main to distal LAD with spontaneous type B dissection of the proximal LAD extending to the left main and middle LAD were detected (Fig. 3). These findings were also shown by intravascular ultrasonography (IVUS) (Fig. 4A) and cardiac CT angiography (Fig. 4B, 4C). We decided to treat with medical therapy because the patient had no chest pain. Three days later, he complained of
Fig. 4. IVUS revealed dissection in the proximal LAD (A). Cardiac CT showed dissection in the LM to middle LAD (B), and dissection in the proximal RCA (C) (IVUS, intravascular ultrasonography; LM, left main coronary artery; RCA, proximal right coronary artery).
Fig. 3. The CAG revealed diffuse stenosis in the left main to distal LAD with spontaneous type B diss- ection of the proximal LAD extending to the left main and middle LAD (CAG, coronary angiography; LAD, left anterior descending coronary artery).
severe chest pain with a 3-fold increase in CK-MB (from 4 U/L to 14.1 U/L) and markedly elevated troponin-I (from 0.03 ng/mL to 2.20 ng/mL). His EKG showed a tall T wave in V2-4 with Q wave in II, III, and aVF. Emergency CAG revealed dissection in the left main (LM) to middle LAD and proximal LCx with poor distal flow and spasm in the distal LAD. We decided to perform percutaneous coronary interven- tion (PCI) for these lesions and deployed the following Cypher stents (Cordis Corp, Johnson & Johnson, Miami Lakes, FL): 3.5×18 mm for proximal LCx, 3.5×28 mm for LM to proximal LAD, 3.5×33 mm for middle LAD, and 3.0×33 mm for distal LAD. The final CAG showed a remaining small dissection in the distal LAD stent edge (Fig. 5). Apico-septal wall akinesia was detected and the patient's ejection fraction was 60% on the
echocardiogram after PCI. The follow-up CAG and renal angiogram were performed 6 months later. CAG showed patent Cypher stents, and no significant stenosis in either renal artery.
Discussion
The possible conditions associated with SCAD are atherosclerosis,5 the peripartum period,4 vasculitis, poly- arteritis nodosa, systemic lupus erythematosus, Marfan's syndrome, Ehlers-Danlos syndrome, hypertension, variant angina, and cocaine use.6,7 The mechanism related to atherosclerosis in SCAD is thought to be atherosclerotic plaque rupture causing disruption of the intimal-medial junction resulting in intramural hematoma formation.
Fig. 5. CAG revealed dissection in the LM to middle LAD and proximal LCx with poor distal flow and spasm in the distal LAD (A). The final CAG after PCI for these lesions showed antegrade TIMI III flow with small dissection in the edge of the distal LAD stent (B) (CAG, coronary angio- graphy; LM, left main coronary artery;
LAD, left anterior descending coro- nary artery; LCx, proximal left circu- mflex artery; PCI, percutaneous cor- onary intervention).
The mechanism of peripartum dissection, however, is related to eosinophilic infiltration in the coronary artery adventitia breaking down the medial-adventitial layers.8
In this case, the SCAD was associated with vasospasm and there was no significant atherosclerosis on IVUS.
In variant angina, spasm may increase the shear stress, leading to SCAD. Eosinophils may cause vasospasm in variant angina. In an animal model, extracts from eosi- nophils caused strong contraction of intestinal smooth muscle.8 This supports that eosinophils can initiate the coronary spasm in humans. In relation to vasospasm, coronary dissection has been reported in cocaine use.
The principal effects of cocaine are mediated by alpha- adrenergic stimulation, which causes an increase in myocardial O2 demand and a reduction in O2 supply because of coronary vasoconstriction.
In this case, we concluded that the culprit coronary artery was the left main to left anterior descending artery (LM to LAD), because apico-septal (LAD terri- tory) wall akinesia was detected on echocardiography.
On the initial CAG, spastic narrowing was detected in the left anterior descending coronary artery and the right coronary artery but no significant atherosclerosis was seen on intravascular ultrasonography (IVUS). The second CAG showed diffuse stenosis in the left main to distal LAD with spontaneous type B dissection of the proximal LAD extending to the LM and middle LAD.
On the third CAG, SCAD was detected in the culprit lesion (LCX) and in the non-culprit lesion (LAD).
When we diagnosed SCAD on the second CAG, the patient did not complain of chest pain or related symptoms, so we chose medical therapy. However, PCI was chosen when SCAD with AMI was detected on the third CAG. Treatment options for SCAD include medical therapy, PCI, or coronary artery bypass graft surgery. There are no randomized studies about the treatment of SCAD, but when the involved vessel is small and there is no evidence of persistent ischemia or hemodynamic instability, medical therapy can be chosen.
When SCAD causes myocardial ischemia, PCI or coro- nary artery bypass graft surgery may be considered.9
In this case, because there was no atherosclerotic lesion, no calcified lesion, and no coronary artery anomaly, the possibility of catheter-induced dissection was very low. However, dissection of the LAD could be considered to be procedure-related because the first angiogram showed no definite dissection in the LAD.
There are some reasons that we consider spontaneous dissection rather than iatrogenic origin. The first reason is that spontaneous dissection was also present in the proximal RCA, which was far from the catheter-engaged site. Dissection flow was started in the proximal LAD, which also far from the catheter-engaged site, and then extended to the left main and down to the middle LAD.
This case showed that vasospasm of the coronary artery can cause SCAD. Further randomized studies on the treatment of SCAD are needed to determine the optimal treatment.
References
1. Auer J, Punzengruber C, Berent R, Weber T, Lamm G, Hartl P, et al. Spontaneous coronary artery dissection involving the left main stem: assessment by intravascular ultrasound. Heart 2004;90:e39.
2. Pretty HC. Dissecting aneurysm of coronary artery in a woman aged 42: rupture. Br Med J 1931;1:667.
3. Thompson EA, Ferraris S, Gress T, Ferraris V. Gender differences and predictors of mortality in spontaneous coronary artery dissection: a review of reported cases. J Invasive Cardiol 2005;17:59-61.
4. Nishikawa H, Nakanishi S, Nishiyama S, Nishimura S, Seki A, Yamaguch H. Primary coronary artery dissection observed at coronary angiography. Am J Cardiol 1988;61:645-8.
5. Chu KH, Menaspace FJ, Blankeship JC, Hausch R, Harrington T.
Polyarteritis nodosa presenting as acute myocardial infarction with coronary dissection. Cathet Cardiovasc Diagn 1998;44:320-4.
6. Sarmento-Leite R, Machado PR, Garcia SL. Spontaneous coronary artery dissection: stent it or wait for healing? Heart 2003;89:164.
7. Park MK, Heo JH, Lee JH, Kim HS, Kwack DH, Jung ER, et al.
A case of acute myocardial infarction associated with spontaneous coronary artery dissection. Korean Circ J 2002;32:1111-5.
8. Robinowitz M, Virmani R, McAllister HA JrU. Spontaneous coronary artery dissection and eosinophilic inflammation: a cause and effect relationship? Am J Med 1982;72:923-8.
9. Mulvihill NT, Boccalatte M, Fajadet J, Marco J. Catheter-induced left main dissection: a treatment dilemma. Catheter Cardiovasc Interv 2003;59:214-6.