359 책임저자:함기백, 406-840, 인천시 연수구 송도동 7-45
이길여암당뇨연구원, 가천의과학대학교 길병원 소화 기내과
Tel: 032-899-6055, Fax: 032-899-6054 E-mail: [email protected]
접수일:2009년 11월 19일, 게재승인일:2009년 11월 30일
Correspondence to:Ki Baik Hahm
Department of Gastroenterology, Gachon Graduate School of Medicine, Gachon University Gil Hospital and Lab of Translational Medicine, Gachon University Lee Gil Ya Cancer and Diabetes Institute, 7-45, Songdo-dong, Yeonsu-gu, Incheon 406-840, Korea
Tel: +82-32-899-6055, Fax: +82-32-899-6054 E-mail: [email protected]
Risk of Gastric Cancer Development in Korean Patients with Chronic Atrophic Gastritis; Highly Predictable with
IL-1β Polymorphisms Compounded with H. pylori Infection and Alcohol Drinking
Tae Kyung Kim1, Yoon Jae Kim1, Jun Won Chung1, Yun Soo Kim1, Ju Hyun Kim1, Woon Kee Lee2 and Ki Baik Hahm1,3
Departments of 1Gastroenterology, 2General Surgery, Gil Medical Center, Gachon University of Medicine and Science, 3Lab of Translational Medicine Gachon University, Lee Gil Ya Cancer and Diabetes Institute, Incheon 406-840, Korea Interleukin 1β gene (IL-1β) polymorphism has been reported to be associated with gastric cancer (GC) or chronic atrophic gastritis (CAG), which are known to be mostly influenced by inflammatory response of Helicobacter pylori (H. pylori). However, there have been striking differences in implication of IL-1β polymorphisms as predictor for gastric cancer between Western and Asian countries, as for which plausible reason for discrepancy could be that the most association studies were done regarding association between normal control and GCs. Therefore, in the current study, we investigated an association of the genotype of IL-1β gene polymorphisms between CAG, high risk group of GC, and GC patients. A total of 365 Korean patients (CAG:257, GC:108) were studied. The polymorphisms in IL-1β gene promoter -31 or -511 were assessed by single base primer extension assay. In the univariate analysis, IL-1β-511 T allele carriers were identified in 183 of 257 in the CAG compared to 64 of 108 in GC group (76.57% vs. 64%; p=0.037) and in multivariate analysis, IL-1β-31 C/C vs. C/T vs. T/T genotype could significantly predict the risk for GC among CAG. When we repeated analysis of data comparing IL-1β haplotype (ht) among the different groups, the IL-1β ht1/ht1 vs. ht1/ht2 vs. ht2/ht2 genotype influenced GC development among patients with CAG, especially compounded with H. pylori infection and alcohol drinking. IL-1β-31 or -511 genetic polymorphisms were significantly associated with GC risk in Korean patients with high risk group of CAG, especially compounded with H. pylori infection and alcohol drinker. (Cancer Prev Res 14, 359-366, 2009)
Key Words: SNPs, Interleukin-1β, Helicobacter pylori, Alcohol, Gastritis, Stomach neoplasm
INTRODUCTION
Gastric cancer (GC) is the second most common cancer worldwide and imposing a significant global health problem, but showing rather very varying geographical distribution.1) South Korea is one of the endemic areas of GC and has much higher prevalence of Helicobacter pylori (H. pylori) infection, 47%
among the general population compared to developed coun- tries.2) Even though individuals infected H. pylori are at an increased risk of developing precancerous diseases like chronic atrophic gastritis (CAG), intestinal metaplasia (IM) and gastric epithelial dysplasia,3) by which IARC (International Agency for Research on Carcinogenesis, Lyon, France) defined H. pylori infection as class I carcinogen. Only lesser than 3% of indivi- duals infected with H. pylori were diagnosed with GC, while
Table 1. Demographic profile of chronic atrophic gastritis and gastric cancer
Demographic profile Chronic atrophic gastritis
Gastric
cancer p-value Number
Male/Female Mean age (range) Smoker (%) Alcohol drinking (%) Helicobacter pylori infection (%)
257 128/129 46.77±12.11
(16∼77) 32.74 50.89 61.40
108 63/45 58.81±12.92
(25∼79) 60.78 64.71 80.43
0.137
<0.001
0.001 0.100 0.016
Table 2. Sequences of PCR amplifying primers and extension primers used
Gene PCR amplifying primers
IL-1β-511
IL-1β-31
F: 5’-TGGCATTGATCTGGTTCATC-3’
R: 5’-GTTTAGGAATCTTCCCACTT-3’
F: 5’-AGCTTCCACCAATACTCTTTTCCCCTTTCC-3’
R: 5’-TACACACAAAGAGGCAGAGAGACAGAG-3’
the others are remained asymptomatic all through the life,4) leaving the possibility that additional host genotype or other environmental factors might influence determine the unwanted outcome after H. pylori infection.
Among these influencing factors, variations in cancer risk among H. pylori infected individuals may be attributed to their genetic predispositions. When the first study that polymorp- hisms in IL-1β was associated with gastric cancer risk was published in Nature,5) hopes that cytokine gene polymorphisms can contribute to determining the different patterns after H.
pylori gastritis,6) by which the risk for H. pylori-associated gastric carcinogenesis can be predicted and managed in ad- vance. Tailored medicine had been proposed based on the fact that IL-1β is a pro-inflammatory cytokine, two linked IL-1β single nucleotide polymorphism that increased IL-1β expres- sion −511C/T and −31C/T were associated with a 2- to 3- fold increased risk of GC.5) However, a meta-analysis afterward deemed these hopes as evidenced that the overall associations between IL-1β or IL-1RN pro-inflammatory polymorphisms and gastric cancer were null except some ethnics.7∼9) These conflicting results may be explained by variation in allele frequencies among the ethnic groups and variation in tumor types, as well as by the methodological quality of the studies.7) As plausible explanation for these contradictory outcomes, we speculated that the most of reported studies were done based on association between normal controls and GC,7∼11) leading to these contradictory or lowered values of IL-1β gene polymor- phism as predictor of risk for GC. Therefore, in the current study, we hypothesized that more clear association could be drawn from analysis among high risk group of gastric cancer, CAG, instead of normal controls and GCs. Here we aimed to investigate the association of IL-1β expression −511C/T, −
31C/T and their haplotypes among Korean patients with CAG and GC. We also incorporated the influence of gene- environmental factors in a logistic regressional analysis inclu- ding H. pylori infection, smoking and alcohol drinking the factors influencing gastric carcinogenesis.
MATERIALS AND METHODS 1. Study subjects
Between March 2002 and February 2009, a total of 365 patients enrolled from outpatient clinic of the Daejin Medical Center Jesaeng Hospital at Bundang, Seongnam city and Gachon University Gil Hospital, Incheon, Korea, were included in this study. All of the patients were single ethnic Korean subjects. Endoscopy was performed after an overnight fast with a standard upper gastroduodenoscope. They were classified into two groups according to the histopathologic evidence of CAG and GC. In patients diagnosed with CAG on endoscopy (Ta- kemoto-Kimura classification was adopted for exact extent of atrophic gastritis as open type and close type), two biopsies were obtained: one biopsy from middle part of antrum was taken and the other biopsy was taken from gastric body. In patients with GC, biopsies were done to confirm by histo- pathologic examination. H. pylori infection was evaluated by CLO test, histopathologic examination and urea breath test. In case of all of which were negative, we difined the patients as H. pylori negative and patients with positive in at least two tests out of three tests were defined as H. pylori positive. De- mographic and clinical details were obtained through a personal interview using a standard clinical protocol. All subjects had given their informed consent for the study and the protocol was approved by the institutional review board including ethnic committee. Demographic profiles were shown in Table 1. The study included 257 patients with CAG and 108 patients with GC. There were significant differences in the distribution of mean age (p=0.01), smoking (p=0.001) and H. pylori infection
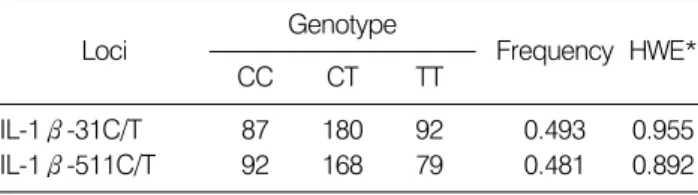
Table 3. Single nucleotide polymorphisms of human IL-1β gene and frequency
Loci Genotype
Frequency HWE*
CC CT TT
IL-1β-31C/T IL-1β-511C/T
87 92
180 168
92 79
0.493 0.481
0.955 0.892
*HWE: Hardy-Weinberg equilibrium.
Table 4. Haplotype frequencies
−31C/T −511C/T Frequencies ht1
ht2
T C
C T
0.507 0.486 (p=0.016) between the groups, but the male to female ration
(p=0.137) and alcohol drinking (p=0.100) were not differed between groups.
2. Genotyping
Genomic DNA was extracted from 300μl whole blood using a DNA Purification kit (GENTRA, Minneapolis, MN.) according to the manufacturer's instructions. The SNPs were detected by polymerase chain reaction (PCR) amplification. The sequence of the primers and probes used in the assays are provided in Table 2. The parameters for thermocycling were as follows: an initial activation step of 95°C for 10 min preceded the cycling program, followed by 35 cycles of de- naturation for 95°C, how long annealing at 72°C for 1 min, and final extension at 72°C for 7 min. Each PCR product was purified by a Qiagen PCR purification kit, and the poly- morphisms were detected by single base primer extension assay (SNP ITTM) using the method as previously described.12) Briefly, the genomic DNA region spanning the polymorphic site was PCR- amplified using one phosphorothiolated primer and one regular PCR primer. The amplified PCR products were digested with exonuclease. The 5'-phosphorothioates protected one strand of the PCR producted from exonuclease digestion, resulting in the generation of a single-stranded PCR template.
The single-stranded PCR template is overlaid onto a 384-well plate that contains covalently attached SNP-ITTM extension primer designed to hybridize immediately adjacent to the polymorphic site. The SNP-ITTM primer was extended for a sin- gle base with DNA polymerase and mixture of appropriate acycloterminator that is labeled with either FITC or biotin and complementary to the polymorphic nucleotide. The identity of the incorporated nucleotide was determined with serial colori- metric reactions with anti-FITC-AP and streptavidin-HRP, respectively. The results of yellow and/or blue color developments were analyzed with an ELISA reader and the
final genotype calls were made with the QCReviewTM program.
All genotyping results were quality controlled by including duplicate samples. We included 6 replicate samples for each of 96 well plates and checked concordances. We accepted data from a plate only if they have less than one mismatches per each plate. Overall concordances were over 99.9% throughout the experiments.
3. Statistical analysis
For univariate analysis, the χ2 test was used for Hardy- Weinberg equilibrium of alleles at individual loci and indepen- dent sample t-test for normally distributed continuous vari- ables. For multivariate analysis, multiple logistic regression ana- lysis was performed. Odds ratios (ORs) with 95% confidence intervals were computed by logistic regression using SPSS version 11.0 software (Chicago, IL). All p values were two- tailed, and a p-value <0.05 was considered to indicate sta- tistical significance throughout the study. Using SASⓇ system, we adopted proportional odds ratio (POR) model to accom- modate complex missing patterns, to increase correlated results, and to account for better “between study” variation.
RESULTS
The clinical and demographic characteristics of the CAG and GC population were compared (Table 1). There was no sig- nificant difference between CAG and GC in terms of sex (12 8:129 vs. 63:45, respectively, p=0.137) and alcohol drin- king (p=0.100). The mean age, number of smoker, and H.
pylori (+) patients was all significantly increased higher in GC compared to CAG, after which logistic regression assay was considered to put unbiased association in Table 8. As known generally, smoking and the H. pylori infection were significantly affecting factors in progression of precancerous lesion in sto- mach. The Hardy-Weinberg equilibrium of alleles at individual loci was assessed and genotype distributions at all polymorphic sites approximated the Hardy-Weinberg equilibrium (HWE, Table 3). Allelic variations were compared between CAG and
Table 5. Linkage Disequilibrium (LD)
|D`|
−31C/T −511C/T
γ2 −31C/T
−511C/T 0.970
1.000
Table 6. Allelic frequency of IL-1β polymorphisms in chronic atrophic gastritis and gastric cancer
Locus Chronic atrophic
gastritis Gastric cancer IL-1β-31
C/C C/T T/T IL-1β-511 C/C C/T T/T Haplotype ht1/ht1 ht1/ht2 ht2/ht2
67 (26.48%) 129 (50.99%) 57 (22.53%)
56 (23.43%) 123 (51.46%) 60 (25.10%)
54 (22.88%) 121 (51.27%) 61 (25.85%)
20 (18.87%) 51 (48.11%) 35 (33.02%)
36 (36.00%) 45 (45.00%) 19 (19.00%)
33 (33.67%) 47 (47.96%) 18 (18.37%)
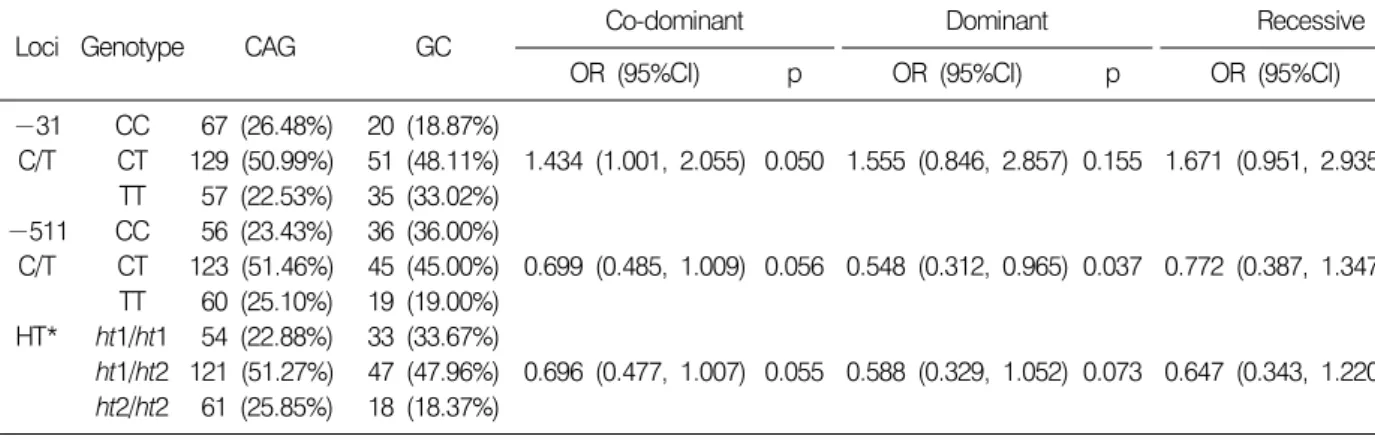
Table 7. Logistic regression of IL-1β polymorphism in chronic atrophic gastritis (CAG) and gastric cancer (GC)
Loci Genotype CAG GC Co-dominant Dominant Recessive
OR (95%CI) p OR (95%CI) p OR (95%CI) p
−31 C/T
−511 C/T
HT*
CC CT TT CC CT TT ht1/ht1 ht1/ht2 ht2/ht2
67 (26.48%) 129 (50.99%) 57 (22.53%) 56 (23.43%) 123 (51.46%) 60 (25.10%) 54 (22.88%) 121 (51.27%) 61 (25.85%)
20 (18.87%) 51 (48.11%) 35 (33.02%) 36 (36.00%) 45 (45.00%) 19 (19.00%) 33 (33.67%) 47 (47.96%) 18 (18.37%)
1.434 (1.001, 2.055)
0.699 (0.485, 1.009)
0.696 (0.477, 1.007) 0.050
0.056
0.055
1.555 (0.846, 2.857)
0.548 (0.312, 0.965)
0.588 (0.329, 1.052) 0.155
0.037
0.073
1.671 (0.951, 2.935)
0.772 (0.387, 1.347)
0.647 (0.343, 1.220) 0.074
0.306
0.179
*HT: Haplotype, Genotypic distribution and p-value for logistic analysis of three alternative models (co-dominant, dominant and recessive model).
GC. In addition, the IL-1β-31T alleles was associated with the IL-1β -511C allele (frequency=50.7%) and this haplotype was identified (ht1 at position −31T, −511C) in the Korean population (Table 4). In the case of IL-1β gene promoter polymorphism, IL-1β-31C and T alleles were completely in linkage disequilibrium with IL-1β-511C and T alleles as shown in Table 5. The frequencies of the genotype of IL-1β gene promoter in enrolled patients are summarized in Table 6.
Genotype and haplotype frequencies in the IL-1β gene promoter were analyzed in the patients with CAG and GC as shown in Table 7. Genotype frequencies in the IL-1β-31 and IL-1β-511 regions were analyzed in patients with CAG and GC.
T allele carriers at IL-1β-31 had a weak correlation with GC risk in a co-dominant model (age and sex adjusted ORs; 1.434, p=0.050) and T allele carriers in IL-1β-511 had correlation with lesser risk of GC in a dominant model (age and sex adjusted ORs; 0.548, p=0.037). In detail, IL-1β-511 T allele carriers were identified in 183 of 257 in CAG group compared to 64 of 100 in GC group (76.57% vs. 64.00%; p=0.037) and IL-1β-31 C/C vs. C/T vs. T/T genotype (p=0.050) influenced GC and CAG. Since specific IL-1β haplotype has been linked to IL-1β production and phenotype, we repeated analysis of data comparing IL-1β haplotype among the different groups.
As results, the IL-1β ht1/ht1 vs. ht1/ht2 vs. ht2/ht2 haplotype showed tendency to influence gastric cancer risk in the back- ground of chronic atrophic gastritis, but statistical significance exceeded significance as p-value of 0.055 (Table 7).
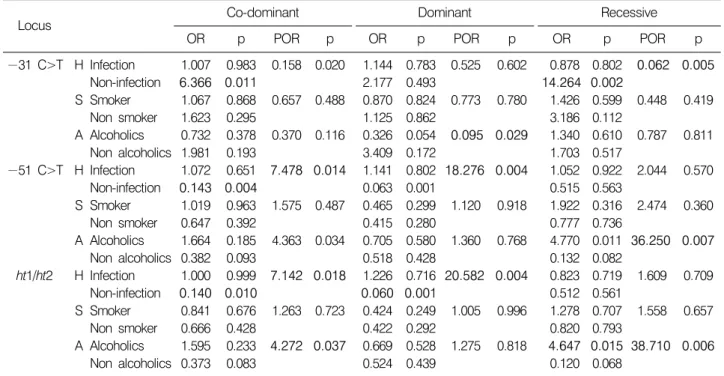
These analyses were further extended to logistic regression analysis incorporating H. pylori, smoking and alcohol parameter (Table 8). IL-1β-31 and IL-1β-511 Co-dominant (C/C vs.
C/T vs. T/T) were significantly associated with H. pylori in- fection (p=0.02 and p=0.014, respectively). Haplotype 1 co- dominant (ht1/ht1 vs. ht1/ht2 vs. ht2/ht2) were significantly asso- ciated with H. pylori infection (p=0.018) and alcohol drinking (p=0.037), suggesting that in the presence of H. pylori infection, IL-1β promoter genotype carries significant risk predictor. In a similar way, IL-1β promoter genotype affected the risk of GC in alcohol drinking patients with CAG.
Table 8. Logistic regression of IL-1β gene polymorphism about Helicobacter pylori (H), smoking (S) and alcohol drinking (A) in chronic atrophic gastritis and gastric cancer
Locus Co-dominant Dominant Recessive
OR p POR p OR p POR p OR p POR p
−31 C>T
−51 C>T
ht1/ht2 H
S
A
H
S
A
H
S
A
Infection Non-infection Smoker Non smoker Alcoholics Non alcoholics Infection Non-infection Smoker Non smoker Alcoholics Non alcoholics Infection Non-infection Smoker Non smoker Alcoholics Non alcoholics
1.007 6.366 1.067 1.623 0.732 1.981 1.072 0.143 1.019 0.647 1.664 0.382 1.000 0.140 0.841 0.666 1.595 0.373
0.983 0.011 0.868 0.295 0.378 0.193 0.651 0.004 0.963 0.392 0.185 0.093 0.999 0.010 0.676 0.428 0.233 0.083
0.158
0.657
0.370
7.478
1.575
4.363
7.142
1.263
4.272 0.020
0.488
0.116
0.014
0.487
0.034
0.018
0.723
0.037 1.144 2.177 0.870 1.125 0.326 3.409 1.141 0.063 0.465 0.415 0.705 0.518 1.226 0.060 0.424 0.422 0.669 0.524
0.783 0.493 0.824 0.862 0.054 0.172 0.802 0.001 0.299 0.280 0.580 0.428 0.716 0.001 0.249 0.292 0.528 0.439
0.525
0.773
0.095
18.276
1.120
1.360
20.582
1.005
1.275 0.602
0.780
0.029
0.004
0.918
0.768
0.004
0.996
0.818
0.878 14.264 1.426 3.186 1.340 1.703 1.052 0.515 1.922 0.777 4.770 0.132 0.823 0.512 1.278 0.820 4.647 0.120
0.802 0.002 0.599 0.112 0.610 0.517 0.922 0.563 0.316 0.736 0.011 0.082 0.719 0.561 0.707 0.793 0.015 0.068
0.062
0.448
0.787
2.044
2.474
36.250
1.609
1.558
38.710 0.005
0.419
0.811
0.570
0.360
0.007
0.709
0.657
0.006
Genotypic distribution and p-value for logistic analysis of three alternative models (co-dominant, dominant and recessive model).
OR stands for Odds ration and POR stands for proportional odds ratio model.
However, smoking was not associated with IL-1β-31 and IL-1 β-511genotypes.
DISCUSSION
Since the first published genomic epidemiologic study show- ing that polymorphisms in IL-1β, proinflammatory cytokine principally engaged in gastritis, was strongly associated with GC.5) The polymorphism of the IL-1 gene is a well-known as host biomarker in increasing the risk of H. pylori associated GC among Caucasians.5,8) Studies from Poland and Scotland have suggested that certain pro-inflammatory genotypes of the IL-1 gene cluster might be associated with GC development.5,13) Furthermore, proinflammatory genotypes of IL-1 loci, such as IL-1β-511T, were significantly related with H. pylori asso- ciated CAG and GC. A study by Rad et al.14) showed that car- riers of IL-1β-511T alleles were associated with more severe gastric inflammation than non-carriers and El-Omer et al.15) estimated the increased odds ratios for individuals having the IL-1β-511T/T genotypes of developing gastric cancer. Zhang et al.16) showed that carriers of IL-1β-31 C and of IL-1β-511
C/T genotypes have higher susceptibility to GC. However, other published reports showed that the relationship between the IL-1 β gene polymorphism and gastritis does not hold true especially in studies from Asia.7,9∼10,13) A possible explanation for these discordances between Western and Asian findings could be related to ethnicity and/or geographical variations. In addition to these factors, all of these studies were between normal controls and GC, none of the afore- mentioned studies were performed between high risk CAG and GC.
The meta-analysis reviews and summary all showed that analysis of results from Western versus East-Asian studies did not match at all except a small number of positive studies,17) deemed the value of cytokine gene polymorphisms. For in- stances, a study by Perri et al.18) performed to evaluate the cytokine gene polymorphisms in Italian patients with gastric adenocarcinoma and to assess whether the difference observed between two Italian geographic areas at high (north area) and low (south area) prevalence rate of GC could be ascribed to a different “pro-inflammatory” genetic profiles of Northern and Southern Italian populations, showed that GC is not associated with specific IL-1β genotypes in Italian population. A similar
study was performed in China by Zeng et al.19) who found that IL-1β-511 T/T genotypes were associated with an increased risk of gastric carcinoma in China and polymorphisms within the gene IL-1β were correlated with gastric cancer in popula- tions living in a geographical area of low gastric cancer pre- valence. Also, the IL-1β-511 genetic polymorphism was not associated with gastric cancer in the Japanese population.20) A study by Garza-Gonzalez et al.21) has confirmed that the proinflammatory IL-1β-31 genotypes contribute significantly to the risk of GC in a Hispanic population, mirroring the findings in Asians. A study by Lee et al.22) did not support that IL-1β-31 polymorphisms were associated with an in- creased risk of GC in Korean population. Kamangar et al.17) examined the association between several inflammation-related polymorphisms and risk of GC. Positive associations between pro-inflammatory genotypes and higher risk of GC, previously reported in other populations, were not replicated among Fin- nish male smokers. A study by Hamajima et al.23) showed that smoking interacted with the IL-1β-31 polymorphism.
However, the interaction rate was especially high among smo- kers harboring the T/T genotype, which is relatively rare for Caucasians. Alcohol drinking showed no interaction with IL-1 β-31 polymorphism.
In the present study, we could demonstrate clearly that IL-1 β polymorphisms, IL-1β-31 TT allele and IL-1β-511 C allele increase the risk of GC in the backgrounds of CAG, especially associated with H. pylori infection or alcohol drinking.
On the other hand, the T carrier genotype frequencies at position −511 in IL-1β gene promoter were significantly lo- wer in the GC group than CAG group, especially highest protective result in H. pylori patients (proportional odds ration (POR)=7.478, p=0.014) or alcohol non-drinking patients (POR=4.363, p=0.034) (Table 8). POR model was proposed to relax the “Odds ratio-homogeneity” assumption, that is, POR accommodates complex missing patterns and accounts for correlated results. Besides accounting better for “be- tween-study” variation, POR model could enhance “explain why” such variation. Therefore, the result of the present study suggests that the T carriers of IL-1β-511 were not more likely to progress GC compared with the IL-1β-511 C/C allele in CAG patients. Additionally, IL-1β-31 C/C vs. C/T vs. T/T genotype influenced GC and CAG in logistical regression analysis. Specific IL-1β haplotype has been linked to IL-1β production and phenotype, we repeated analysis of data
comparing IL-1β haplotype among the different groups. The IL-1β ht1/ht1 negatively influenced GC in the background of CAG as evidenced that patients with ht1 haplotype were very protective from GC, if the patients have not been infected with H. pylori (OR=0.140, POR=7.142, p=0.018 on co-dominant analysis and OR=0.060, POR=20.582, p=0.004 on dominant analysis), whereas if the patients were associated with alcohol drinking, higher risk of GC development in the background of CAG (POR=4,272, p=0.037 on co-dominant analysis, POR= 38.710, p=0.006 on recessive analysis).
In summary from our study, H. pylori infection and lifestyle factors were found to modify the effect of IL-1β polymorphism in the GC and CAG patients. The relationship between H. pylori infection and IL-1β polymorphism such as IL-1β-511 genotype, IL-1β-31 genotype and IL-1β ht1 genotype was examined to clarify the possible interactions in GC and CAG.
Alcohol drinking interacted with the IL-1β polymorphism in this study, but smoking status was not interactive with the IL-1β polymorphism.
Conclusively, GC has a multi-factorial pathogenesis and mul- tiple risk factors such as diet (nitroso compounds, salt, low fola- te and vitamin B12 levels etc.), cigarette smoking, alcohol and socioeconomic status in addition to H. pylori infection.24) Though support for a role of cytokine genetic polymorphisms is conflicting overall and especially lacking in some Asian populations including Korean. Our current study added the evidences that IL-1β polymorphisms could be predictor for risk of GC in high risk disease background compounded with H.
pylori infection and alcohol drinking. As further hope, ad- vancement in high throughput analysis will facilitate the search for SNP present in whole genome, in addition to cooperative efforts through the International HapMap Project and Global Human Genome Projects.25) Moreover, it is hoped that collea- gues within and between the major Asian countries including Korea where H. pylori and gastric cancer remaining among the top three causes of cancer mortality will cooperate to yield much needed mechanistic and prognostic information about gastric cancer, so that it may eventually be prevented. Our study could provide the one hope that association study should be considered between large numbers of patients with precancerous lesion and gastric cancer intermingled with the influences of contributing factors, strongly supported with the previous publication by Figueirredo et al.26) that combined bacterial/host genotyping may provide an important tool in
defining disease risk and targeting H. pylori eradication to high risk individuals.
ACKNOWLEDGEMENT
This study was supported by a grant from the National R&D Program for Cancer Control, The Ministry for Health, Welfare and Family Affairs and the Ministry for Education, Science and Technology. Republic of Korea.
REFERENCES
1) Roukos DH. Current status and future perspectives in gastric cancer management. Cancer Treat Rev 26, 243-255, 2000.
2) Kim JH, Kim HY, Kim NY, Kim SW, Kim JG, Kim JJ, Roe IH, Seo JK, Sim JG, Ahn H, Yoon BC, Lee SW, Lee YC, Chung IS, Jung HY, Hong WS, Choi KW. Seroepide- miological study of Helicobacter pylori infection in asympto- matic people in South Korea. J Gastroenterol Hepatol 16, 969-975, 2001.
3) Correa P. Human gastric carcinogenesis: a multistep and mul- tifactorial process--First American Cancer Society Award Lec- ture on Cancer Epidemiology and Prevention. Cancer Res 52, 6735-6740, 1992.
4) Peek RM Jr, Blaser MJ. Helicobacter pylori and gastrointestinal tract adenocarcinomas. Nat Rev Cancer 2, 28-37, 2002.
5) El-Omar EM, Carrington M, Chow WH, McColl KE, Bream JH, Young HA, Herrera J, Lissowska J, Yuan CC, Rothman N, Lanyon G, Martin M, Fraumeni JF Jr, Rabkin CS.
Interleukin-1 polymorphisms associated with increased risk of gastric cancer. Nature 404, 398-402, 2000.
6) Machado JC, Figueiredo C, Canedo P, Pharoah P, Carvalho R, Nabais S, Castro Alves C, Campos ML, Van Doorn LJ, Caldas C, Seruca R, Carneiro F, Sobrinho-Simoes M. A proinflammatory genetic profile increases the risk for chronic atrophic gastritis and gastric carcinoma. Gastroenterology 125, 364-371, 2003.
7) Camargo MC, Mera R, Correa P, Peek RM Jr, Fontham ET, Goodman KL, Piazuelo MB, Sicinschi L, Zabaleta J, Schneider BG. Interleukin-1b and interleukin-1 receptor antagonist ene polymorphisms and gastric cancer: a meta-analysis. Cancer Epidemiol Biomarkers Prev 15, 1674-1687, 2006.
8) Lahner E, Corleto VD, D'Ambra G, Di Giulio E, Fave GD, Annibale B. Is interleukin-1 genotyping useful for the clinical management of patients with atrophic body gastritisβ.
Aliment Pharmacol Ther 27, 355-365, 2008.
9) Shin YW, Jang JS, Kim HS, Kim SJ, Kim KH, Jang MK, Lee JH, Kim HJ, Kim HY. Polymorphisms of interleukin-1 and interleukin-2 genes in patients with gastric cancer in Ko- rea. J Gastroenterol Hepatol 23, 1567-1573, 2008.
10) Wang W, Ni K, Zhou G. Association of IL 1B polymor-
phisms with gastric cancer in a Chinese population. Clin Biochemistry 40, 218-225, 2007.
11) Hellmig S, Titz A, Steinel S, Ott S, Folsch UR, Hampe J, Schreiber S. Influence of IL-1 gene cluster polymorphisms on the development of H. pylori associated gastric ulcer. Im- munology Letters 100, 107-112, 2005.
12) Syvanen AC. From gel to chips: "minisequencing" primer extension for analysis of point mutations and single nucleotide polymorphisms. Human Mutat 13, 1-10, 1999.
13) Wang P, Xia HH, Zhang JY, Dai LP, Xu XQ, Wang KJ.
Association of interleukin-1 gene polymorphisms with gastric cancer: a meta-analysis. Int J Cancer 120, 552-562, 2007.
14) Rad R, Dossumbekova A, Neu B, Lang R, Bauer S, Saur D, Gerhard M, Prinz C. Cytokine gene polymorphisms influence mucosal cytokine expression, gastric inflammation, and host specific colonisation during Helicobacter pylori infection. Gut 53, 1082-1089, 2004.
15) El-Omar EM. The importance of interleukin 1beta in Heli- cobacter pylori associated disease. Gut 48, 743-747, 2001.
16) Zhang WH, Wang XL, Zhou J, An LZ, Xie XD. Association of interleukin-1β (IL-1β) gene polymorphisms with risk of gastric cancer in Chinese population. Cytokine 30, 378-381, 2005.
17) Kamangar F, Cheng C, Abnet CC, Rabkin CS. Interleukin-1 β polymorphisms and gastric cancer risk--a meta-analysis.
Cancer Epidemiol Biomarkers Prev 15, 1920-1928, 2006.
18) Perri F, Piepoli A, Bonvicini C, Gentile A, Quitadamo M, Di Candia M, Cotugno R, Cattaneo F, Zagari MR, Ricciardiello L, Gennarelli M, Bazzoli F, Ranzani GN, Andriulli A. Cy- tokine gene polymorphisms in gastric cancer patients from two Italian areas at high and low cancer prevalence. Cytokine 30, 293-302, 2005.
19) Zeng ZR, Hu PJ, Hu S, Pang RP, Chen MH, Ng M, Sung JJ. Association of interleukin 1β gene polymorphism and gastric cancers in high and low prevalence regions in China.
Gut 52, 1684-1689, 2003.
20) Kato S, Onda M, Yamada S, Matsuda N, Tokunaga A, Matsukura N. Association of the interleukin-1 beta genetic polymorphism and gastric cancer risk in Japanese. J Gastro- enterol 36, 696-699, 2001.
21) Garza-Gonzalez E, Bosques-Padilla FJ, El-Omar E, Hold G, Tijerina-Menchaca R, Maldonado-Garza HJ, Perez-Perez GI.
Role of the polymorphic IL-1β, IL-1RN and TNF-A genes in distal gastric cancer in Mexico. Int J Cancer 114, 237-241, 2005.
22) Lee SG, Kim B, Choi W, Lee I, Choi J, Song K. Lack of association between pro-inflammatory genotypes of the in- terleukin-1 (IL-1β-31 C/+ and IL-1RN *2/*2) and gastric cancer/duodenal ulcer in Korean population. Cytokine 21, 167-171, 2003.
23) Hamajima N, Matsuo K, Saito T, Tajima K, Okuma K, Yamao K, Tominaga S. Interleukin 1 polymorphisms, lifestyle
factors, and Helicobacter pylori infection. Jpn J Cancer Res 92, 383-389, 2001.
24) Lee DH, Hahm KB. Inflammatory cytokine gene poly- morphisms and gastric cancer. J Gastroenterol Hepatol 23, 1465- 1472, 2008.
25) Collins FS, Morgan M, Patrinos A. The human genome project; ;essons from large scale biology. Science 300, 286-290,
2003.
26) Figueiredo C, Machado JC, Pharoah P, Seruca R, Carvalho R, Capelinha AF, Quint W, Caldas C, van Doorn LJ, Carneiro F, Sobrinho-Simoes M. Helicobacter pylori and interleukin 1 genotyping: An opportunity to identify high-risk individuals for gastric carcinoma. J Natl Cancer Inst 94, 1680-1687, 2002.