서 론
(Natrii sulfas) mirabilite
, , , ,
, ,
, , .
1). , Effect of Purgative Action with Natrii Sulfas on Brain Edema of MCAO Rats
Ho-Chang Kang1, Bum-Hoi Kim2, Eun-Sheb Shim1, Il-Hwan Kang1, Seong-Joon Kim1, Hee Kang1, Nak-Won Sohn1
1Division of Oriental Medical Science, Graduate School of East-West Medical Science, Kyung Hee University
2Department of Anatomy, College of Oriental Medicine, Dong-Eui University
Objectives: This study aimed to evaluate the effect of purgation therapy with Natrii sulfas, an oriental medical therapy for stroke patients with constipation, on physiological indexes and the brain edema of rats.
Methods: Brain edema was induced by the middle cerebral artery occlusion (MCAO); Natrii sulfas was administered once after the MCAO. At 3, 6, 15, 24, 48 hours after reperfusion, physiological indexes such as fecal weight, urine volume and water content in stool were assessed, and at 48 hours after reperfusion the edema index was measured.
Results:
1. Purgation therapy with Natrii sulfas significantly improved the reduction of fecal weight caused by ischemic insult (P<0.05).
2. Purgation therapy with Natrii sulfas significantly improved the reduction of urine volume caused by ischemic insult (P<0.05).
3. Purgation therapy with Natrii sulfas significantly improved the reduction of water content in stool caused by ischemic insult (P<0.05).
4. Purgation therapy with Natrii sulfas did not improve the neurological symptom caused by ischemic insult.
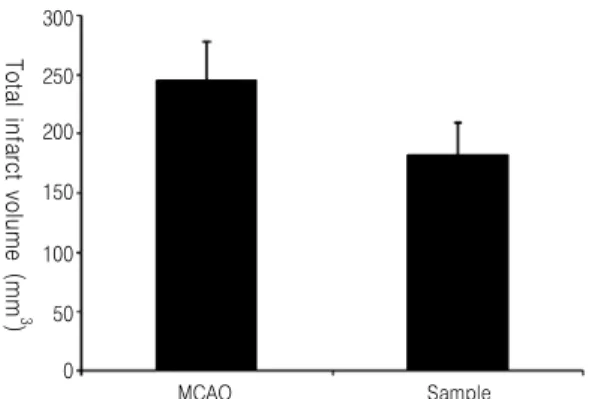
5. Purgation therapy with Natrii sulfas did not attenuate the total infarct volume caused by ischemic insult.
6. Purgation therapy with Natrii sulfas attenuated the brain edema caused by ischemic insult (P<0.05).
Conclusions: These results suggest that purgation therapy with Natrii sulfas improves some important symptoms and has a protective effect on the brain edema caused by ischemic insult.
Key Words : Natrii sulfas, middle cerebral artery occlusion, brain edema, purgation
芒硝 瀉下作用 腦浮腫
강호창1, 김범회2, 심은섭1, 강일환1, 김성준1, 강희1, 손낙원1
1경희대학교 동서의학대학원 한의과학전공, 2동의대학교 한의과대학 해부학교실
Original Article
Received:29 May 2009 Revised:15 June 2009 Accepted:31 July 2009
Correspondence to:손낙원(Nak-Won Sohn)
경기도 용인시 기흥구 서천동 1번지 경희대학교 전자정보관 444호
2). ‘ ’ .
,
3,4).
5).
6),
7-9).
10-12)
.
.
, 48
.
재료 및 방법
1. 실험동물
( ) 9 , 250 g
Sprague-Dawley
. 21~23 , 40~60%, 12
/
,
1 .
2. 뇌허혈 손상유발과 실험군의 구분
(middle cerebral artery occlusion, MCAO) .
, (electric coagulator) .
, (5-0 silk)
, (3-0 silk)
.
poly-L-lysine (4-0 nylon)
18-20 mm .
,
. ,
. 2
.
,
MCAO Sample
. Sham
,
.
6 .
3. 약물의 제조 및 투여
(Natrii Sulfas) 200 g 2,000 ml , rotary evaporator
(-70 , 10 mmHg) 185.4 g
, 92.7% .
4 g 100 g 53 mg 1
, 2
10
1 .
4. 대소변 수집
cage
, .
cage 1-2 cm
70~80
.
, cage
(g) .
(g) .
5. 대변 내 수분함유량의 측정
60 oven 24
.
.
6. 신경학적 증상의 측정
.
3, 6, 15, 24, 48 1
, .
1 m .
0 ,
1 . 1
1
2 ,
1 3 .
7. 뇌허혈 손상의 해부조직학적 평가
3, 6, 15, 24, 48 ,
brain matrix (ASI, USA) rat brain atlas
interaural distance 2 mm 6
. 6 2% TTC
37 incubator 30
, .
.
8. 뇌허혈 손상 면적의 측정
“Axiovision LE”
software (Carl Zeiss Vision, Ver.4.2, USA)
.
, (C)
(B)
(C-B) (Fig. 1).
C C C C B
B B B AA
AA Damaged Damaged Damaged Damaged
Fig. 1.
.
×
9. 뇌부종 크기의 측정
TTC
((A+B)/C) , 6
(Fig. 1).
10. 통계처리
Student’s T-test
P<0.05 P<0.01 .
결 과
1. 대변량의 변화
48
, Sample
MCAO ,
15 , 24 , 48
(P<0.05) (Table 1,
Fig. 2). 6 15 24
Cumulative Amount of Stool (g)
7
6
5
4
3
2
1
0 3h 6h 15h 24h 48h
Reperfusion Time
Sample MCAO Sham
Fig. 2.
3h 6h 15h 24h 48h
Sham 0.73±0.13 1.09±0.14 1.60±0.15 2.84±0.31 5.86±0.61
MCAO 0.38±0.09 0.45±0.13 0.91±0.18 1.27±0.14 2.17±0.18
Sample 0.73±0.19 1.01±0.37 1.95±0.29* 2.33±0.30† 3.60±0.39*
Mean ± S.E. (*; P<0.05, †; P<0.01 Vs MCAO ) Table 1.
48 .
2. 소변량의 변화
MCAO
Sample Sham .
Sample 15
MCAO 24 (P<
0.01) 48 (P<0.05) Sample MCAO (Table 2, Fig. 3).
3. 대변 내 수분함유량의 변화
3h 6h 15h 24h 48h
Sham 2.03±0.25 3.61±0.20 4.52±0.37 7.80±0.48 13.6±1.51
MCAO 1.56±0.07 2.85±0.17 3.41±0.20 3.80±0.37 5.67±0.49
Sample 1.70±0.14 3.02±0.27 3.43±0.70 5.87±0.54† 8.32±0.99*
Mean ± S.E. (*; P<0.05, †; P<0.01 Vs MCAO ) Table 2.
Cumulative Amount of Urine (g)
16
14
12
10
8
4
2
0
3h 6h 15h 24h 48h
Reperfusion Time
Sample MCAO Sham
6
Fig. 3.
3h 6h 15h 24h 48h
Sham 0.08±0.01 0.25±0.03 0.24±0.09 0.29±0.05 0.41±0.06
MCAO 0.02±0.00 0.01±0.01 0.02±0.01 0.06±0.01 0.05±0.01
Sample 0.09±0.05 0.13±0.07 0.26±0.09* 0.24±0.09* 0.19±0.05*
Mean ± S.E. (*; P<0.05 Vs MCAO ) Table 3.
, Sham 6 15
. MCAO
, Sample MCAO
,
15 , 24 , 48 (P < 0.05) . , 15
Sample Sham
. 24 , 48
Sham (Table 3,
Neurological Score
3.5
3
2.5
2
1.5
0.5
0
0h 6h 15h 24h 48h
Reperfusion Time
Sample MCAO 1
3h
Fig. 5.
Water Content In Stool (g)
0.5 0.45
0.4 0.35
0.3
0.2 0.15
0
3h 6h 15h 24h 48h
Reperfusion Time
Sample MCAO Sham
0.25
0.1 0.05
Fig. 4.
Fig. 3).
4. 신경학적 증상의 변화
3 , 6 , 15 , 24 , 48
Sample MCAO
(Fig. 5).
5. 뇌손상 면적의 변화
48 MCAO Sample
Sample MCAO
(Fig. 6, 7).
6. 뇌부종 크기의 변화
3 48 Sample
MCAO
. , 3 MCAO
1.13±0.03, Sample 1.06±0.01, 48 MCAO 1.38±0.01, Sample 1.31±0.05
MCAO Sample
Fig. 6.
MCAO Sample
300
250
200
150
100
50
0 Total infarct volume (mm 3)
Fig. 7.
Ischemia/contra-lateral ratio
1.6 1.4 1.2
1 0.8
0.6
0.4 0.2
0 3h 48h
Reperfusion Time
MCAO Sample
3 Sample MCAO (P<0.05)
(Table 4, Fig. 8).
고 찰
mirabilite .
, . , ,
, , ,
,
1). ,
.
,
13).
2,10)
. ,
, ,
,
14).
.
, , ,
2,10)
.
, ,
, 15,16).
,
,
17-19)
,
20,21)
,
, ,
3
22-25)
. 220
74.47% , 184
83 ,
98%, 88%,
46% 11).
,
26). 4
MCAO
3h 48h
MCAO 1.13 ± 0.03 1.38 ± 0.01
Sample 1.06 ± 0.01* 1.31 ± 0.05
Mean ± S.E. (*; P < 0.05 Vs MCAO ) Table 4.
. 2
Sham , MCAO
, Sham 15
15
MCAO Sham
.
,
26). ,
27,28)
. ,
Sample MCAO
. 15 , 24
, 48 Sample MCAO
(P<0.05)
6 15 , 24 48
15 Sham
.
Sample
MCAO ,
3 , 6 , 15
24 48 .
15 , 24 , 48 MCAO
(P<0.05) , 6 15
.
, 6 15
,
. Blood Brain Barrier
29-33)
, 2
3
48 BBB
34,35)
. ,
3 48
, MCAO Sample
3 48
. Sample
MCAO 3
.
48 Sample MCAO
. ,
,
,
.
결 론
(transient MCAO)
. 1.
(P < 0.05) . 2.
(P < 0.05) . 3.
(P < 0.05) . 4.
. 5.
. 6.
, 3 ,
.
참고문헌
1. . . :
. 1994:244-5.
2. Hwang CW, Byun I. A Literatual study on the Emergency care and Administration method of Medical emergency. Hye Hwa Medicine . 1994;
1(3):16-45.
3. . . : . 1997:303-48.
4. Koo BS, Lee DS, Moon SK, Go CN, Cho KH, Bae HS, Lee KS, Kim YS. Effects of Daeseungki- tang on Constipated Stroke Patients. The Journal of Korean Oriental Medicine. 2000;21(2):3-13.
5. , , , , , .
. . 1998;14(1):27-8
6. Fisher M. Characterizing the target of acute stroke therapy. Stroke. 1997;28(4):866-72.
7. . . :
. 1998:178-88, 339-49, 521-50.
8. Cho KH. Medical Management of Spontaneous Intracerebral Hemorrhage. Korean Journal of Stroke. 2003:5(1):26-9.
9. Alberts MJ. Diagnosis and treatment of ischemic stroke. Am J Med. 1999;106(2):211-21.
10. Lee Won Chul. Research on the Xiafa used at the acute stages of Stroke. The Jounal of Korean Oriental Medicine. 1998;19(1):385-90.
11. Im SU. The Clinical Evaluation of Defecation in Stroke Patients. Journal of Korea Institute of Oriental Medical Informatics. 1997;3(1)7-11.
12. Alberts MJ. Treatment of acute ischemic stroke.
J Stroke Cerebrovasc Dis. 2001;10(2 Pt 2):10-7.
13. . . : . 1982:398,
402-4, 506-8.
14. Son DH, Jo GH, Kim YS, Bae HS, Lee GS, Lee YG. The Comparison Study on the Effect of Bowel Movement between Bo-Ryu Enema(Bao- Liu Enema) and General Enema in Patients at the Acute Stage of Cerebrovascular Accident.
The Journal of Korean Oriental Medicine . 2001;22(3):51-62.
15. .
. : MIP. 2003;252.
16. Bharucha AE. Constipation. Best Pract Res Clin Gastroenterol. 2007;21(4):709-31.
17. Ullman T, Reding M. Gastrointestinal dysfunction in stroke. Semin Neurol. 1996;16(3):269-75.
18. Winge K, Rasmussen D, Werdelin LM. Constip- ation in neurological diseases. J Neurol Neurosurg Psychiatry. 2003;74(1):13-9.
19. Johanson JF, Sonnenberg A, Koch TR, McCarty DJ. Association of constipation with neurologic diseases. Dig Dis Sci. 1992;37(2):179-86.
20. Camilleri M, Bharucha AE. Gastrointestinal dysfunction in neurologic disease. Semin Neurol.
1996;16(3):203-16.
21. Han TR. Prognostic Evaluation in Stroke Rehabilitation. Journal of Korean Academy of Rehabilitation Medicine. 1997;21(5):817-25.
22. Chakrabarti SD, Ganguly R, Chatterjee SK, Chakravarty A. Squatting, blood pressure and stroke. J Assoc Physicians India. 2002;50:382-6.
23. Krogh K, Christensen P, Laurberg S. Colorectal symptoms in patients with neurological diseases.
Acta Neurol Scand. 2001;103(6):335-43.
24. Indredavik B, Bakke F, Slordahl SA, Rokseth R, Hâheim LL. Treatment in a combined acute and rehabilitation stroke unit: which aspects are most important? Stroke. 1999;30(5):917-23.
25. Bhalla A, Wolfe CD, Rudd AG. Management of acute physiological parameters after stroke.
QJM. 2001;94(3):167-72.
26. Modo M, Stroemer RP, Tang E, Veizovic T, Sowniski P, Hodges H. Neurological sequelae
and long-term behavioural assessment of rats with transient middle cerebral artery occlusion.
J Neurosci Methods. 2000;104(1):99-109.
27. Lee CZ, Litt L, Hashimoto T, Young WL.
Physiologic monitoring and anesthesia conside- rations in acute ischemic stroke. J Vasc Interv Radiol. 2004;15(1 Pt 2):S13-9.
28. Perkin GD, Murray-Lyon I. Neurology and the gastrointestinal system. J Neurol Neurosurg Psychiatry. 1998;65(3):291-300.
29. Paczynski RP, Venkatesan R, Diringer MN, He YY, Hsu CY, Lin W. Effects of fluid management on edema volume and midline shift in a rat model of ischemic stroke. Stroke. 2000;31(7):1702-8.
30. Pulsinelli W. Pathophysiology of acute ischaemic stroke. Lancet. 1992;339(8792):533-6.
31. Ting P, Masaoka H, Kuroiwa T, Wagner H,
Fenton I, Klatzo I. Influence of blood-brain barrier opening to proteins on development of post-ischaemic brain injury. Neurol Res. 1986;
8(3):146-51.
32. Klatzo I. Blood-brain barrier and ischaemic brain oedema. Z Kardiol. 1987;76:67-9.
33. Klatzo I. Pathophysiological aspects of brain edema. Acta Neuropathol. 1987;72(3):236-9.
34. Kuroiwa T, Ting P, Martinez H, Klatzo I. The biphasic opening of the blood-brain barrier to proteins following temporary middle cerebral artery occlusion. Acta Neuropathol. 1985;68(2):
122-9.
35. Kuroiwa T, Cahn R, Juhler M, Goping G, Campbell G, Klatzo I. Role of extracellular proteins in the dynamics of vasogenic brain edema. Acta Neuropathol. 1985;66(1):3-11.