443 통신저자:서 중 배
충남 천안시 안서동 16-5
단국대학교 의과대학 정형외과학교실 Tel:041-550-3060․Fax:041-556-3238 E-mail:[email protected]
*본 논문의 요지는 2005년도 대한견주관절학회 춘계학술대회에서 발표되었음.
Address reprint requests to:Joong-Bae Seo, M.D.
Department of Orthopedic Surgery, Dankook University College of Medicine, 16-5, Anseo-dong, Cheonan 330-715, Korea
Tel:82-41-550-3060․Fax:82-41-556-3238 E-mail:[email protected]
건국대학교 의과대학 정형외과학교실, 단국대학교 의과대학 정형외과학교실*
목 적: Y형 금속판을 이용한 상완골 과간 골절의 치료에 있어서 치료의 결과와 그에 영향을 미칠 수 있는 요인을 조사하였다.
대상 및 방법: Y-형 금속판을 이용하여 고정한 상완골 과간 골절 환자 중 1년 이상 추시가 가능하였던 17예를 대상으로 하였다.
C1형이 9예, C2형이 4예, C3형이 4예였다. 11예에서 다른 부위의 동반 골절이 있었다. 평균 연령은 48.8세였으며, 평균 추시 기간은 33개월이었다. 평가는 Cassebaum 분류 (Cassebaum’s classification for elbow range of motion)와 Mayo Elbow Performance Score (MEPS)를 사용하였다.
결 과: 주관절의 운동 범위는 평균 105도 (50∼150도)로 회복되었다. Cassebaum 분류에서 매우 우수 7예, 우수 1예, 보통 4예, 불량이 5예였으며, MEPS에서는 매우 우수 7예, 우수 7예, 보통 2예, 불량이 1예였다. MEPS상 보통 및 불량으로 평가된 3예 중 C3형이 2예였다. 수술 후 결과에 큰 영향을 미칠 만한 합병증은 없었다.
결 론: 상완골 과간 골절에서 Y-형 금속판을 이용한 고정은, 환자의 선택이 적절히 이루어진다면 좋은 치료 방법이 될 수 있을 것으로 생각된다. 결과의 영향을 미치는 요인으로는 골절의 관절내 분쇄 정도라 생각되며 고 에너지 손상 여부 및 연령도 결과에 다소 영향을 미칠 것으로 생각된다.
색인 단어: 상완골 과간 골절, Y-형 금속판
Treatment of Intercondylar Fractures of Humerus with Y-plate
Jin-Young Park, M.D., Joong-Bae Seo, M.D.*, Ji-Yong Chun, M.D.*, Myoung-Ho Kim, M.D.*, Sang-Hyuk Min, M.D.*, Joo-Hong Lee, M.D.*
Department of Orthopedic Surgery, Kunkuk University College of Medicine, Seoul, Department of Orthopedic Surgery, Dankook University College of Medicine*, Cheonan, Korea
Purpose: To evaluate the results of the treatment of intercondylar fractures of the humerus using Y-plate.
Materials and Methods: The subjects were 17 patients with intercondylar fracture of humerus who were treated using the Y-plate.
Nine cases were C1 type, 4 were C2 type, and the remaining 4 were C3 type. 11 subjects had accompanying fractures of another part of the body. The average age was 48.8. The average follow up period was 33 months. We used Mayo Elbow Performance Score and Risborough-Radin’s rating score for each patient as the methods of rating.
Results: The average range of motion of the elbow was 105 degrees (50∼150 degrees). According to Cassebaum’s classification for elbow range of motion, 7 cases were rated very good, 1 cases were good, 4 cases were fair, and 1 cases were poor.
According to Mayo Elbow Performance Score, 7 were excellent, 7 were good, 2 fair, and 1 poor. Of the 3 patients who were fair or poor in Mayo Elbow Performance Score, 2 were type C3 fractures, and all 3 had major accompanying fractures. No significant postoperative complications developed in all cases.
Conclusion: The fixation with Y-plate can still be a relatively good modality of treatment for interconylar fractures of the humerus in selected cases, in spite of the known mechanical weakness of the Y-plate. The patients with severe intra-articular comminution showed relatively poor results. And we think that the age of the patient and the energy of the injury have more or less influence on the results of treatment.
Key Words: Intercondylar fracture of humerus, Y-plate
서 론
상완골 과간 골절은 그동안 수술 기법과 내고정물의 꾸준 한 발전에도 불구하고, 현재도 치료하기 매우 어려운 골절로 알려져 있다7). 그 이유로 상완골 원위부의 복잡한 구조, 골 다공증, 관절내 분쇄, 골간단부의 분쇄, 또는 관련된 손상 등 을 지목하고 있다20).
다른 부위의 관절내 골절에 대한 치료와 마찬가지로 관 절내 골편의 정확한 해부학적 정복, 견고한 내고정 및 수술 후 조기 관절 운동을 가장 중요한 치료 원칙으로 삼고 있
다4,6,11,18). 고정방법으로는 Y-형 금속판 또는 변형된 해부학
적 금속판을 이용하는 방법13), 관절내 골편을 서로 나사못으 로 고정하고 서로 90도 각도로 이중 금속판 (dual plate)4)으 로 내외측 골주를 고정하는 방법 (columnar stabiliza- tion)9,18,19), 그리고 최근에는 두 개의 금속판을 서로 마주보 도록 설치한 후, 서로 교차하는 방식의 나사못 (interdigita- tion screw)을 이용한 고정 방법15) 등이 있다.
저자들은 내고정물로써 Y-형 금속판이 적절한지의 여부와 결과에 영향을 미치는 요인들은 무엇인지를 분석하고, 문제 점이 있다면 어떻게 개선할 수 있을지 알아보고자 본 연구를 시행하였다.
대상 및 방법
2000년 1월부터 2003년 12월까지 본원에서 Y-형 금속판을 이용하여 고정한 상완골 과간 골절 환자 중 1년 이상 추시가 가능하였던 17예를 대상으로 하였다. 남자가 9예, 여자가 8 예였으며, 평균 연령은 48.8세 (16∼74세)였다. 우성측이 11 예였고 비우성측이 6예였다. 수상 후 수술 시까지의 기간은 평균 14일 (0∼30일)이었고, 추시 기간은 평균 33개월(12∼
60개월)이었다.
AO 분류17)상 C1 골절이 9예였고, 골간단부 분쇄가 있는 C2 골절은 4예, 관절내 분쇄가 있는 C3 골절이 4예였다. 3예 는 Gustilo-Anderson 분류 중 II형이 2예, IIIA형이 1예인 개 방성 골절이였고, 11예에서 동반 손상이 있었는데, 비구 골 절 또는 대퇴골 골절 등 하지의 주요 골절이 5예, 요골 골절 등 동측의 상지 골절이 3예에서 동반되었고, 기타 골절이 4 예 동반되었다.
모든 예에서 후방 도달법을 이용하여 골절부를 노출하였 으며, 이 중 14예는 주두 절골술을, 나머지 4예는 Bryan- Morrey의 광범위 도달법1)을 이용하였다. 고정 방법으로써 Fig. 1. (A) Initial radiographs show a type C3 intercondylar fracture of a 30-year-old male patient. He was injured by fall from height.
(B) Radiographs after operation show intra-articular fragments were fixed with an additional screw and k-wires.
(C) Follow-up radiographs 1 year after operation show good fracture healing without complication.
A B C
Table 1. Mayo elbow performance score
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Function Points Definition (points) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Pain 45 None (45)
Mild (30) Moderate (15) Severe (0)
Motion 20 Arc>100 degrees (20)
Arc 50∼100 degrees (15) Arc<50 degrees (5)
Stability 10 Stable (10)
Moderate instability (5) Gross instability (0)
Function 25 Comb hair (5)
Feed (5)
Perform hygiene (5) Don shirt (5) Don shoe (5)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Total 100
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Classification; Excellent: >90, Good: 75∼89, Fair: 60∼74, Poor:
<60.
동을 허용하였다.
결과에 대한 평가는 최종 추시 시 촬영한 전후면 및 측면 방사선 소견과 이학적 진찰을 토대로 하였으며, Mayo El- bow Performance Score (Mayo score, Table 1)14)와 Casse- baum에 의한 관절 운동 범위의 분류 (Cassebaum 분류, Table 2)2)을 모두 사용하였다. Mayo score는 동통 (pain),
나누어져 있다. 또한 단순 방사선 촬영을 통해 골절의 정복 정도 및 골유합 시기와 내고정 소실 등의 합병증들을 조사하 였다. 골유합 시기는 전후방 및 측면 방사선 소견상 가골 형 성과 임상적으로 골절부 압통 및 운동 시 통증유발이 없어진 때를 기준으로 하였다.
결 과
최종 추시상 평균 운동 범위는 105도 (50∼150도)였으며, 굴곡 구축이 평균 10도 (0∼30도), 최대 굴곡이 평균 115도 (50∼150도)였다 (Table 3).
Mayo Score에 의하면 매우 우수 (excellent) 7예, 우수 (good) 7예, 보통 (fair) 2예, 그리고 불량 (poor)이 1예였다 (Fig. 2). 이를 골절의 분류별로 보면 전반적으로 C1 골절 예 에서 높은 점수를 얻은 예가 많았으나 오히려 C1에서 보통
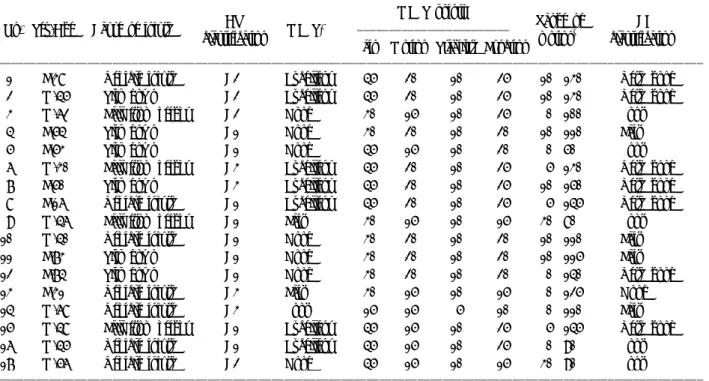
Table 3. Brief data on each patient with intercondylar fractures of humerus
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ MEPS points
AO Range of CB
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
No. Sex/Age Cause of injury MEPS*
classification motion‡ classification†
Pain Motion Stability Function
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
1 F/38 Vehicle injury C2 Excellent 45 20 10 25 10∼130 Very good
2 M/45 Slip down C2 Excellent 45 20 10 25 10∼130 Very good
3 M/62 Fall from height C2 Good 30 15 10 25 0∼100 Poor
4 F/54 Slip down C1 Good 30 20 10 20 10∼110 Fair
5 F/53 Slip down C1 Good 45 15 10 20 0∼50 Poor
6 M/30 Fall from height C3 Excellent 45 20 10 25 5∼130 Very good
7 F/50 Slip down C3 Excellent 45 20 10 25 10∼150 Very good
8 F/16 Vehicle injury C1 Excellent 45 20 10 25 5∼145 Very good
9 M/46 Fall from height C1 Fair 30 15 10 15 30∼80 Poor
10 M/40 Vehicle injury C1 Good 30 20 10 20 10∼110 Fair
11 F/73 Slip down C1 Good 30 20 10 20 10∼115 Fair
12 F/74 Slip down C1 Good 30 20 10 20 0∼140 Very good
13 F/31 Vehicle injury C3 Fair 30 15 10 15 0∼125 Good
14 M/68 Vehicle injury C3 Poor 15 15 5 10 0∼110 Fair
15 M/48 Fall from height C1 Excellent 45 15 10 25 5∼145 Very good
16 M/45 Vehicle injury C1 Excellent 45 15 10 25 0∼90 Poor
17 M/56 Vehicle injury C2 Good 45 15 10 15 30∼90 Poor
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*MEPS: Mayo elbow performance score, †CB classification: Cassebaum’s classification for elbow range of motion, ‡Range of motion:
Flexion contracture-further flexion.
Table 2. Cassebaum’s classification for elbow range of motion ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Classification Range of motion
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Very good Flexion>130 degrees, extension deficit<15 degrees Good Flexion>120 degrees, extension deficit<40 degrees Fair Flexion>110 degrees, any extension deficit Poor Flexion<110 degrees
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
에 그친 경우가 1예 있었다. 보통 및 불량으로 평가된 3예 중 C3형이 2예였으며, 3예 모두 교통사고 또는 추락 사고 등 고 에너지 손상이었고, 비구 또는 대퇴골 골절 등 하지의 주 요 골절을 동반하는 공통점이 있었다.
Cassebaum 분류에 의하면 매우 우수 7예, 우수 1예, 보통 4예, 그리고 불량 5예였다. 보통 및 불량한 결과는 C1 골절 에서 6예, C2에서 2예, C3에서 1예가 있었다 (Fig. 3). 보통 및 불량으로 평가된 9예의 수상 원인은 교통사고 4예와 추락 사 2예의 고 에너지 손상이 6예이며 3예는 실족이었으며, 평 균 나이는 55.2세 (40∼73세)로 매우 우수와 우수의 8예의 평 균 나이 41.1세 (16∼74세)보다 다소 높은 것으로 나타났다.
수술 후 합병증으로서 2예에서 피부 괴사가 발생하였으나, 변연절제술 후 피부이식술을 시행하여 치료하였다. 수상 당 시부터 척골 신경 부분 마비를 보인 1예가 있었으며, 수술 시 신경이전술을 시행하였으며, 최종 추시상 약간의 감각 이 상만이 관찰되었다. 그리고 불유합과 내고정물의 이완 (fi- xation failure) 및 이소성 골화는 없었다.
고 찰
역사적으로 상완골 원위부 골절은 치료 결과가 좋지 않은 대표적인 골절이다. 실제로 오랫동안 상완골 원위부 골절에 대한 수술적 치료와 bag-of-bone 방법을 이용한 비수술적 치 료에 대해 논란이 많이 되어왔다. 그러나, 지난 20여 년간 이 골절은 수술적 정복 및 내고정이 필요하며, 분쇄 골절이 나 골다공증이 있는 경우 견고한 내고정이 어려워 결과가 좋 지 않다고 여러 논문들에서 발표되었다16). 그러나 현재의 상 완골 원위부 골절의 치료에 대한 치료 목표가 동통 없이 만 족스러운 주관절 기능을 회복하기 위해 관절면의 해부학적 인 복원, 상완골 원위부의 전반적인 구조의 복원, 그리고 조 기 관절운동이 가능할 만큼의 견고한 내고정이 반드시 필요 하다는 점에 이견이 거의 없다4,6,11,18). 그러나 이러한 목표를 성취하기에는 기술적인 어려움이 따르며, 특히 골다공증이 심하거나 분쇄가 심할 경우는 더욱 그러하다는 것이 문제점 으로 남아있다15). 심지어 Cobb와 Morrey는 노령의 환자에서 원위 상완골 골절은 일차적으로 주관절 전 치환술로 치료하 Fig. 2. Results assessed by Mayo elbow performance score,
which are sorted according to AO classification.
Fig. 4. (A) Initial radiographs show a low T fracture of the distal humerus by vehicle injury in a 56-year-old woman.
(B) Postoperative radiographs show that low T fracture was properly fixed with single interfragmentary screw and Y-plate. In low T fractures, which have fracture line crossing olecranon fossa, it is difficult to purchase the distal fragments only by Y-plate.
(C) Follow-up radiographs 1 year after operation show good fracture healing without complications.
A B C
Fig. 3. Results assessed by Cassebaum’s classification for elbow range of motion, which are sorted according to AO classification. Five poor results were three cases in C1 fractures and two cases in C2 fractures.
을수록 전반적으로 좋은 결과를 얻었다. 그렇지만 Casse- baum 분류에서는 C1 골절에서 6예, C2에서 2예가 보통 및 불량한 결과를 얻어 관절 운동 범위에 관한 좋은 결과는 분 쇄가 적음과 연결된다고 볼 수 없었다. 또한 관절 운동 범위 에 관한 결과에는 고 에너지 손상 여부와 나이도 다소간 영 향을 미칠 것이라고 생각된다.
Mehne과 Matta는 과간 골절을 6가지로 분류하였는데8,12), 저자들은 그중 골간단부 골절선이 주두와보다 원위부를 통 과하고, 골절편이 작아 Y-형 금속판으로 가장 고정하기가 어 렵다는 하 T-형 골절 (low T-fracture)7)에 해당하는 5예를 별 도로 분석하였다. 모든 예에서 Y-형 금속판 외에 관절 내 골 절편의 고정을 위해 골절편간 나사 (interfragmentary screw) 를 이용한 추가 고정이 필요하였으며, Mayo score 상 매우 우수가 2예, 우수가 3예였으며, Cassebaum’s classification에 의하면 최우수가 2예, 보통이 2예, 그리고 불량이 1예로, 전 체적인 결과와 별 차이가 없었다. 저자들은 하 T-형 골절에 서 낮은 과간 골절편을 Y-형 금속판으로 고정하기 힘들다는 문제점을 추가적인 골절편간 나사를 이용하여 해결할 수밖 에 없었으며, 이 경우 금속판 자체보다는 추가적인 골절편간 나사가 고정에 주요한 역할을 하였다고 생각된다 (Fig. 4).
상완골 원위부 골절의 치료골절의 고정 방법으로 저자들 이 사용한 Y-형 금속판외에 해부학적 Y-형 금속판, 서로 90 도 각도로 설치한 이중 금속판 등이 있는데, 근래에는 일반 적으로 이중 금속판에 의한 방법이 표준 술기로 자리잡고 있 는 추세이다. 최근에는 소두 골편의 후면에 설치하는 금속판 이 주관절 굴곡상태에서 내번 외력에 취약하다는 이유로 서 로 마주보는 형태의 평행 금속판 (parallel plate)을 설치 후 교차 나사못 (interdigitation screw)을 이용한 고정방법이 소 개되기도 하였다15,16).
본 연구를 통하여 저자들은, 분쇄의 정도가 결과에 가장 영향을 미치는 것으로 조사되었으며, 이는 Kim과 Eom의 보 고에서도 뒷바침하고 있다10). 그리고 Y-형 금속판은 역학적 으로 취약한 것으로 지적 받고 있음에도 불구하고 비교적 과 간 골절편이 크고, 골 질 (bone quality)이 좋은 상완골 과간 골절의 경우에 효과적인 내고정물임을 알 수 있었다. 더욱이 나사 (screw) 또는 K-강선을 이용한 보강 고정 (additional fixation)으로 하 T-형 골절에서도 어느 정도 역할을 할 수 있음을 알 수 있었다. 또한 이중 금속판과는 달리 Y-형 금속
때 상완골 원위부 골절 시 금속판의 선택 및 환자의 선택에 신중을 기해야 한다고 생각한다.
결 론
상완골 과간 골절에서 Y-형 금속판을 이용한 고정으로 비 교적 만족스러운 결과를 얻을 수 있었다. 그러나 대부분의 예에서 나사 또는 K-강선을 이용한 보강 고정 (additional fixation)이 필요하였으며, 결과에 영향을 미치는 요인으로 관절내 분쇄 정도가 중요한 것으로 판단되며 고 에너지 손상 의 여부와 나이도 관절 운동 범위에 관한 결과에 다소 영향 을 미칠 것으로 생각된다. 따라서 환자의 선택을 세심하게 하며, K-강선이나 나사못 등에 의한 보강 고정을 적절히 사 용한다면 Y-형 금속판을 이용한 상완골 과간 골절의 치료 결 과를 향상시킬 수 있을 것으로 판단된다.
참 고 문 헌
1) Bryan RS and Morrey BF: Extensive posterior exposure of the elbow. A triceps-sparing approach. Clin Orthop, 166: 188- 192, 1982.
2) Cassebaum WH: Open reduction of T & Y fractures of the lower end of the humerus. J Trauma, 9: 915-925, 1969.
3) Cobb TK and Morrey BF: Total elbow arthroplasty as primary treatment for distal humeral fractures in elderly pa- tients. J Bone Joint Surg, 79-A: 826-832, 1997.
4) Gabel GT, Hanson G, Bennett JB, Noble PC and Tullos HS: Intraarticular fractures of the distal humerus in the adult.
Clin Orthop, 216: 99-108, 1987.
5) Helfet DL and Hotchkiss RN: Internal fixation of the distal humerus: a biomechanical comparison of methods. J Orthop Trauma, 4: 260-264, 1990.
6) Holdsworth BJ and Mossad MM: Fractures of the adult distal humerus. Elbow function after internal fixation. J Bone Joint Surg, 72-B: 362-365, 1990.
7) Jupiter JB: Complex fractures of the distal part of the humerus and associated complications. Instr Course Lect, 44:
187-198, 1995.
8) Jupiter JB and Mehne DK: Fractures of the distal humerus.
Orthopedics, 15: 825-833, 1982.
9) Jupiter JB, Neff U, Holzach P and Allgower M:
Intercondylar fractures of the humerus. An operative approach.
J Bone Joint Surg, 67-A: 226-239, 1985.
10) Kom YK and Eom GS: Operative treatment of intra-articular T or Y. J Korean Fracture Soc, 13: 303-310, 2000.
11) Letsch R, Schmit-Neuerburg KP, Sturmer KM and Walz M: Intraarticular fractures of the distal humerus. Surgical treatment and results. Clin Orthop, 241: 238-244, 1989.
12) Mehne DK and Jupiter JB: Fractures of the distal humerus.
In: Browner BD ed. Skeletal trauma: fractures, dislocations, Ligamentous injuries. Philadelphia, PA, WB Saunders: 1146- 1176, 1991.
13) Moon ES, Rowe SM, Seon JK, Kim MS and Cho SB:
Treatment in distal humerus fracture with anatomical Y plate.
J Korean Fracture Soc, 17: 76-82, 2004.
14) Morrey BF and An KN: Functional evaluation of the elbow.
In: Morrey BF ed. The elbow and its disorders. 3rd ed.
Philadelphia, PA, WB Saunders: 74-83, 2000.
15) O’Driscoll SW: Optimizing stability in distal humeral fracture fixation. J Shoulder Elbow Surg, 14: 186S-194S, 2005.
16) O’Driscoll SW, Jupiter JB, Cohen MS, Ring D and McKee MD: Difficult elbow fractures: pearls and pitfalls. Instr Course Lect, 52: 113-134, 2003.
17) Perren SM: Basic aspects of internal fixation. The compre- hensive classification of fractures of long bones. In: Muller ME ed. Manual of internal fixation. 3rd ed. New York, Springer-Verlag: 118-149, 1990.
18) Ring D and Jupiter JB: Fractures of the distal humerus.
Orthop Clin North Am, 31: 103-113, 2000.
19) Self J, Viegas SF, Buford WL Jr and Patterson RM: A comparison of double-plate fixation methods for complex distal humerus fractures. J Shoulder Elbow Surg, 4: 10-16, 1995.
20) Zagorski JB, Jennings JJ, Burkhalter WE and Uribe JW:
Comminuted intraarticular fractures of the distal humeral con- dyles. Surgical vs. nonsurgical treatment. Clin Orthop, 202:
197-204, 1986.