서 론
자살은 공중보건의 중요한 주제이며 매우 심각한 사회 문제 중 하나이다.1,2)
2017
년 기준 국내 자살 사망자수는12
,463
명이며10
만 명당 자살률로는24
.3
명으로5
번째 높은 사망원인이다.10
만명당 자 살률이 연령에 비례해 증가하여60
대는30
.2
명,70
대는48
.8
명,80
대 는70
.0
명이다. 한국의60
세 이상 자살률은 경제협력개발기구 (Organi zation for Economic Co-operation and Development
,OECD
) 가입 국가 중 가장 높고
70
세 이상 자살률은OECD
회원국 평균보다3
배 이상 더 높다.3)자살생각 위험요인을 알게 되면 자살을 예방할 수 있다.4) 자살은 대체로 자살생각과 계획을 거쳐 일어나게 된다.5-7) 자살생각을 경험 한
34
%가 자살계획을 수립하며 자살을 계획한 경우72
%가 자살을 시도한다. 하지만 자살을 계획하지 않고 자살생각을 하고 자살을 시 도하는 경우도26
%에 이른다.6) 이러한 경향성은 노인에서 더욱 두드 러진다.8)Received October 12, 2019 Accepted November 22, 2019 Corresponding author Jun-Hyun Yoo
Tel: +82-2-3410-2440, Fax: +82-2-3410-0388 E-mail: [email protected]
ORCID: http://orcid.org/0000-0002-0344-5123
Copyright © 2019 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Original Article
https://doi.org/10.21215/kjfp.2019.9.6.546 eISSN 2233-9116
Korean J Fam Pract. 2019;9(6):546-553
Korean Journal of Family Practice
KJFP
한국 노인에서 다중이환과 자살생각의 연관성
한요한
1,2, 유준현
1,*, 조인영
11
성균관대학교 의과대학 삼성서울병원 가정의학과,
2충북대학교 의과대학 의생명융합대학원
Association between Multimorbidity and Suicidal Ideation in Korean Elderly
Yo Han Han1,2, Jun-Hyun Yoo1,*, In Young Cho1
1Department of Family Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul; 2Graduate School of Biomedical Convergence, College of Medicine, Chungbuk National University, Cheongju, Korea
Background: Recent studies have reported that multimorbidity is associated with suicidality. The objective of this study was to evaluate the association
between physical multimorbidity and suicidal ideation (SI) among the elderly.Methods: A total of 6,712 subjects aged over 65 years without depression were analyzed from the Korea National Health and Nutrition Examination
Survey databases (2010–2013, 2015). In our study, multimorbidity was defined as being diagnosed with two or more chronic diseases. The association between multimorbidity and SI was evaluated through multiple logistic regression analysis.Results: Through our analysis, 40.7% of participants had multimorbidity and the 14.6% had SI. Multimorbidity was associated with suicidal ideation
when adjusting for sociodemographic and health behavior covariates (odds ratio [OR], 1.33; 95% confidence interval [CI], 1.14–1.55). However, no association between multimorbidity and SI existed after adjusting for additional health status factors. In subgroup analyses performed according to education level and health status, the risk of SI was high in subjects with multimorbidity only in those with below elementary school education level (OR, 1.36; 95% CI, 1.14–1.63). Further subgroup analysis indicated that the group without stress and the group without depressiveness both showed association of multimorbidity with SI (OR, 1.27; 95% CI, 1.02–1.59; OR, 1.28; 95% CI, 1.05–1.56).Conclusion: The study findings suggest that elderly with multimorbidity must be identified, evaluated, and managed for SI with special attention to
those with education levels below elementary school. Physicians should also focus on assessing mental health status in the case of multimorbidity in the elderly without depression.Keywords: Suicidal Ideation; Multimorbidity; Aged; Korea
한요한 외. 신체질환의 다중이환과 자살생각
Korean Journal of Family PracticeKJFP
최근 여러 질환을 가진 환자의 건강 수준과 삶의 질에 미치는 포 괄적인 영향에 관심을 가지고자 다중이환(
multimorbidity
)이라는 표 현을 사용한다.9) 다중이환의 정의는2
개 이상의 만성질환에 이환 된 경우10) 또는 다양한 질환의 임상적 복합성을 평가하는 경우(예,Charlson comorbidity index
11)) 또는 노인포괄평가(comprehensive geriatric assessment
)와 같이 노화에 따른 전반적인 건강문제를 포함 하여 만성적 문제가2
개 이상인 경우12)로 한다. 역학적 평가가 용이 한 방법인2
개 이상의 만성질환에 이환 된 것으로 다중이환을 정의 하여 시행한 연구에서65
세 이상 노인 절반 이상이 다중이환된 것 으로 확인되었다.10)1999
년 고령화 사회로 진입한 한국은2018
년 기 준65
세 이상 인구가 전체 인구의14
.3
%로2060
년에는41
.0
%가 될 것 으로 예상된다.13) 노인인구가 증가하는 한국에서 다중이환은 중요한 보건 문제이며14) 노인의 다중이환을 잘 이해하는 것이 필요하다.15)Read
등16)은 다중이환된 경우, 그렇지 않은 경우보다2–3
배 더 우 울증이 발생한다고 보고하였다. 잘 알려진 것과 같이 우울증은 자 살과 연관된 가장 흔하며 핵심적인 질환이다.6,7) 다중이환은 우울증 뿐 아니라 다양한 정신질환과 증상의 위험요소다.17) 이전 연구에서 신체 및 정신질환에 다중이환된 경우 자살생각 위험도가 매우 높다 고 보고하였다. 그러나 신체질환만 다중이환된 경우의 자살생각과 연관성은 연구들 간에 서로 일치하지 않는 결과를 보였다.17,18) 하지 만 개별 질환별로 평가한 자살생각 위험도에서는 유의미한 결과를보였다.19,20)
노인은 다른 연령대에 비하여 자살생각 경험률과 다중이환율이 모두 높다. 이러한 노인을 대상으로 한 신체질환의 다중이환과 자살 생각의 관계에 대해 살펴볼 필요가 있을 것으로 보인다. 이전 연구 결과에서 신체 및 정신질환 모두 다중이환된 경우 우울증과 자살생 각 위험도를 높였으나 신체질환만 다중이환된 경우와 자살생각 간 의 연관성은 서로 다른 결과를 보였다. 이에 신체질환만 다중이환 된 경우 자살생각과 어떠한 연관성을 보이는지 살펴보는 것이 필요 한 것으로 생각된다.
이에 본 연구는 이전에 우울증을 진단받지 않은
65
세 이상 노인 을 대상으로 신체질환의 다중이환과 자살생각 사이의 연관성을 평 가하기 위해 수행되었다.방 법
1. 연구 대상자 및 자료 수집
국민건강영양조사
5
기1–3
차(2010–2012
년)와6
기1
차(2013
년),3
차 (2015
년) 조사에 참여한 만65
세 이상 노인 자료를 이용하였다.2010
년1
,419
명,2011
년1
,543
명,2012
년1
,595
명,2015
년1
,484
명으로 총7
,370
명이었으며 이 중 건강설문조사에 참여하지 않은281
명과 이전 에 우울증을 진단받은377
명을 제외한 총6
,712
명을 분석 대상으로 하였다. 본 연구는 성균관대학교 의과대학 삼성서울병원 기관윤리Original Article
Korean Journal of Family Practice
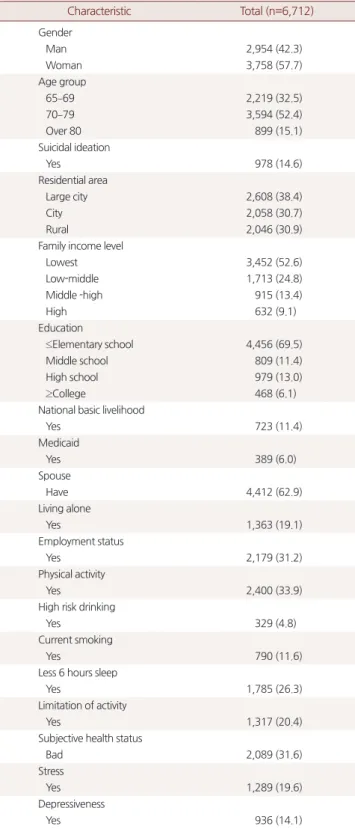
Table 1. Characteristics of the participants
Characteristic Total (n=6,712) Gender
Man 2,954 (42.3)
Woman 3,758 (57.7)
Age group
65–69 2,219 (32.5)
70–79 3,594 (52.4)
Over 80 899 (15.1)
Suicidal ideation
Yes 978 (14.6)
Residential area
Large city 2,608 (38.4)
City 2,058 (30.7)
Rural 2,046 (30.9)
Family income level
Lowest 3,452 (52.6)
Low-middle 1,713 (24.8)
Middle -high 915 (13.4)
High 632 (9.1)
Education
≤Elementary school 4,456 (69.5)
Middle school 809 (11.4)
High school 979 (13.0)
≥College 468 (6.1)
National basic livelihood
Yes 723 (11.4)
Medicaid
Yes 389 (6.0)
Spouse
Have 4,412 (62.9)
Living alone
Yes 1,363 (19.1)
Employment status
Yes 2,179 (31.2)
Physical activity
Yes 2,400 (33.9)
High risk drinking
Yes 329 (4.8)
Current smoking
Yes 790 (11.6)
Less 6 hours sleep
Yes 1,785 (26.3)
Limitation of activity
Yes 1,317 (20.4)
Subjective health status
Bad 2,089 (31.6)
Stress
Yes 1,289 (19.6)
Depressiveness
Yes 936 (14.1)
Values are presented as number (%).
Yo Han Han, et al. Multimorbidity and Suicidal Ideation
Korean Journal of Family Practice
KJFP
심의위원회의 심사면제 심의(
IRB File No
.2019-07-081
)를 통과하였다.2. 연구변수
다중이환은 통상 개인이
2
개 이상의 질환에 동시에 이환 된 현상 을 말한다.21) 본 연구에서는 다음20
개의 질환 중2
개 이상의 질환 을 가진 경우를 다중이환으로 정의하였다.12
개의 만성질환과8
개 의 암(고혈압, 이상지질혈증, 뇌졸증, 심근경색증, 협심증, 천식, 간경 변증, 골관절염, 류마티스성 관절염, 신부전, 당뇨, 갑상선질환, 위 암, 대장암, 간암, 유방암, 자궁경부암, 폐암, 갑상선암, 기타암)을 대 상으로 하였다. 만성질환은 의사의 진단을 받았으며 현재 유병 중인 경우로, 암은 의사의 진단을 받은 경우로 정의하였다. 자살생각 경 험여부는 자기 기입식으로 설문조사한 건강행태조사 항목 중 지난1
년 동안 자살생각 경험 여부를 묻는 문항에 ‘예’로 답한 경우 자살 생각을 경험한 것으로 정의하였다. 인구사회학적변수는 연령, 성별, 거주지역, 가구소득, 교육 정도, 기초생활수급여부, 건강보험종류, 배우자유무, 독거여부, 취업상태를 포함하였다. 연령은65–69
세,70–79
세,80
세 이상의3
군으로 분류하였다. 거주지역은 광역시는 대 도시, 그 외 동지역은 도시로 분류하였다. 단, 읍ㆍ면에 거주하는 경 우 농촌으로 분류하였다. 건강관련 변수에 대해서는 건강행동(신체 활동, 고위험 음주, 현재 흡연과6
시간 미만 수면여부)과 건강상태 (활동 제한, 주관적 건강상태, 스트레스와 우울감)를 포함하였다.걷기를
1
주일 동안 주5
일 이상,1
회30
분 이상 한 경우 신체활동을 한 것으로 분류하였으며 고위험 음주 여부는 연간1
회 평균 음주량 이 남자는7
잔(여자는5
잔) 이상이고, 주2
회 이상 음주한 경우로 하Table 2. Suicidal ideation by disease, multimorbidity and the cumulative number of diseases
Total Suicidal ideation
P-value
No Yes
Total 6,712 (100.0) 5,734 (85.4) 978 (14.6)
Chronic disease
Angina 290 (4.1) 237 (80.7) 53 (19.3) 0.068
Asthma 231 (3.6) 179 (77.6) 52 (22.4) 0.007
Diabetes mellitus 1,221 (18.4) 1,034 (84.6) 187 (15.4) 0.514
Dyslipidemia 1,038 (15.7) 911 (87.5) 127 (12.5) 0.078
Hypertension 3,376 (50.5) 2,843 (83.9) 533 (16.1) 0.003
Liver cirrhosis 26 (0.4) 23 (81.4) 3 (18.6) 0.667
Myocardial infarction 127 (1.9) 106 (86.2) 21 (13.8) 0.825
Osteoarthritis 1,700 (25.8) 1,356 (79.7) 344 (20.3) <0.001
Renal failure 29 (0.3) 25 (88.5) 4 (11.5) 0.652
Rheumatoid arthritis 182 (2.7) 147 (78.8) 35 (21.2) 0.053
Stroke 264 (4.0) 213 (83.3) 51 (16.7) 0.375
Thyroid disease 138 (1.9) 118 (84.8) 20 (15.2) 0.873
Cancer
Breast cancer 44 (0.6) 36 (87.0) 8 (13.0) 0.739
Cervix cancer 56 (0.9) 47 (87.7) 9 (12.3) 0.661
Colon cancer 85 (1.4) 73 (83.9) 12 (16.1) 0.754
Liver cancer 14 (0.2) 13 (95.1) 1 (4.9) 0.232
Lung cancer 27 (0.4) 24 (92.3) 3 (7.7) 0.290
Stomach cancer 136 (2.1) 125 (93.5) 11 (6.5) 0.015
Thyroid cancer 36 (0.5) 36 (100.0) 0 (0.0) -
Others 132 (2.0) 112 (82.6) 20 (17.4) 0.467
Multimorbiditya <0.001
No 4,008 (59.3) 3,482 (87.0) 526 (13.0)
Yes 2,704 (40.7) 2,252 (83.0) 452 (17.0)
No. of disease <0.001
0 1,831 (27.1) 1,622 (88.9) 209 (11.1)
1 2,177 (32.3) 1,860 (85.5) 317 (14.5)
2 1,587 (23.7) 1,330 (83.5) 257 (16.5)
3 755 (11.4) 625 (81.9) 130 (18.1)
Over 4 362 (5.5) 297 (83.0) 65 (17.0)
Values are presented as number (%).
aTwo or more diseases in the same person.
P-value were obtained by chi-square test.
한요한 외. 신체질환의 다중이환과 자살생각
Korean Journal of Family PracticeKJFP
였다. 현재 흡연 여부는 평생 담배
100
개비 이상 피웠고 현재 담배를 피우는 경우로 하였다. 활동 제한 여부는 신체 혹은 정신적 장애로 일상생활 및 사회 활동에 제한을 받는 경우 활동 제한이 있는 경우 로 분류하였다. 우울감은2
주 연속 우울감 여부에 대한 응답을 이 용하였으며 모름, 무응답은 우울감이 없는 것으로 분류하였다.3. 통계 분석
국민건강영양조사 원시자료 분석지침에 따라 통합하였고, 복합 표본설계로 구성된 자료이므로 분산추정층, 층화변수 및 표본가중 치를 적용하여 분석하였다. 대상자의 특성에 따른 빈도와 백분율을 산출하였고, 자살생각 경험여부에 따른 각 질환별과 다중이환 그리 고 누적질환개수에 따른 변인의 차이는 카이 제곱 검정을 이용하여 두 군 간의 변수 분포를 비교하였다. 다중이환과 자살생각, 누적질 환개수와 자살생각 간의 연관성을 평가하기 위해 자살생각 경험 여 부를 종속변수로 한 다변량 로지스틱 회귀분석을 시행하여 다중이 환, 누적질환개수에 대한 교차비(
odd ratio
,OR
)와95
% 신뢰구간 (confidence interval
,CI
)을 구하였다. 분석은3
단계로 수행되었다. 분 석모형1
에서는 인구사회학적변수를 보정하여 분석하였다. 분석모 형2
에서는 건강행동변수를 추가하여 보정하였으며 분석모형3
에서 는 건강상태변수를 더 추가하여 보정하였다.모든 통계분석은
SAS 9
.2
프로그램(SAS Institute
,Cary
,NC
,USA
) 을 이용하였으며 통계학적 유의 수준은P
값이0
.05
미만인 경우로 정의하였다.결 과
Table 1
에서는 대상자의 인구사회학적변수와 건강관련변수의 빈도와 퍼센트를 제시하였다. 전체
6
,712
명 중978
명(14
.6
%)이 자살생 각을 경험하였다. 남자는2
,954
명(42
.3
%), 여자가3
,758
명(57
.7
%)이었 다.65–69
세는2
,219
명(32
.5
%),70
대는3
,594
명(52
.4
%),80
세 이상은899
명(15
.1
%)이었다.Table 2
에서는 자살생각 경험 여부와 신체질환, 다중이환과 누적질환개수의 빈도와 퍼센트를 제시하였다. 다중이환된 노인은
2
,704
명(40
.7
%)이었으며 이들 중452
명(17
.0
%)이 자살생각을 경험하였다.다중이환된 경우와 누적질환개수에 따른 자살생각 경험여부는 유 의한 차이를 보였다.
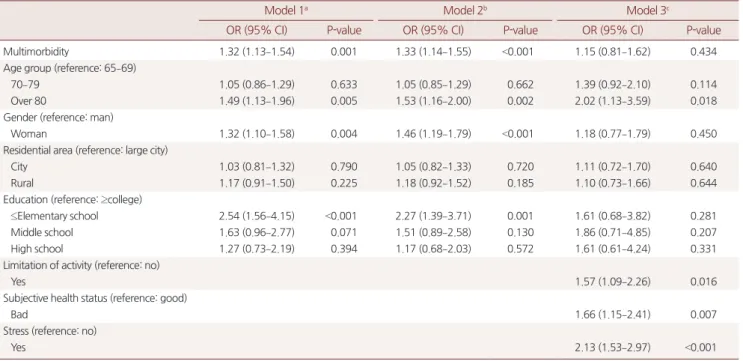
Table 3
은 다중이환의 자살생각에 대한 교차비와95
% 신뢰구간 을 보여준다. 인구사회학적변수만을 보정했을 때, 다중이환된 경우 자살생각 위험도는 유의하게 높았다(Model 1
,adjusted OR
,1
.32
;95
%CI
,1
.13–1
.54
). 건강행동변수를 추가적으로 보정하여도 다중이Table 3. The association between multimorbidity and suicidal ideation
Model 1a Model 2b Model 3c
OR (95% CI) P-value OR (95% CI) P-value OR (95% CI) P-value
Multimorbidity 1.32 (1.13–1.54) 0.001 1.33 (1.14–1.55) <0.001 1.15 (0.81–1.62) 0.434
Age group (reference: 65–69)
70–79 1.05 (0.86–1.29) 0.633 1.05 (0.85–1.29) 0.662 1.39 (0.92–2.10) 0.114
Over 80 1.49 (1.13–1.96) 0.005 1.53 (1.16–2.00) 0.002 2.02 (1.13–3.59) 0.018
Gender (reference: man)
Woman 1.32 (1.10–1.58) 0.004 1.46 (1.19–1.79) <0.001 1.18 (0.77–1.79) 0.450
Residential area (reference: large city)
City 1.03 (0.81–1.32) 0.790 1.05 (0.82–1.33) 0.720 1.11 (0.72–1.70) 0.640
Rural 1.17 (0.91–1.50) 0.225 1.18 (0.92–1.52) 0.185 1.10 (0.73–1.66) 0.644
Education (reference: ≥college)
≤Elementary school 2.54 (1.56–4.15) <0.001 2.27 (1.39–3.71) 0.001 1.61 (0.68–3.82) 0.281
Middle school 1.63 (0.96–2.77) 0.071 1.51 (0.89–2.58) 0.130 1.86 (0.71–4.85) 0.207
High school 1.27 (0.73–2.19) 0.394 1.17 (0.68–2.03) 0.572 1.61 (0.61–4.24) 0.331
Limitation of activity (reference: no)
Yes 1.57 (1.09–2.26) 0.016
Subjective health status (reference: good)
Bad 1.66 (1.15–2.41) 0.007
Stress (reference: no)
Yes 2.13 (1.53–2.97) <0.001
OR, odds ratio; CI, confidence interval.
aModel 1: adjustments for age group, gender, residential area, national basic livelihood, education level, living status and employment status. bModel 2: same as model 1+adjustments for physical activity, high risk drinking, current smoking and less than 6 hours sleep. cModel 3: same as model 2+adjustments for limitation of activity, subjective health status and stress.
Yo Han Han, et al. Multimorbidity and Suicidal Ideation
Korean Journal of Family Practice
KJFP
환의 자살생각 위험도는
1
.33
배 높게 나타났다(Model 2
,adjusted OR
,1
.33
;95
%CI
,1
.14–1
.55
). 그러나 건강상태변수를 추가 보정 시 통계적 연관성은 소실되었다(Model 3
,adjusted OR
,1
.15
;95
%CI
,0
.81–1
.62
). 누적질환개수가 많아질수록 활동의 제약이 더 생기고 주 관적 건강상태는 나빠지며 우 울감도 유의하게 증가하였다 (Supplement 1
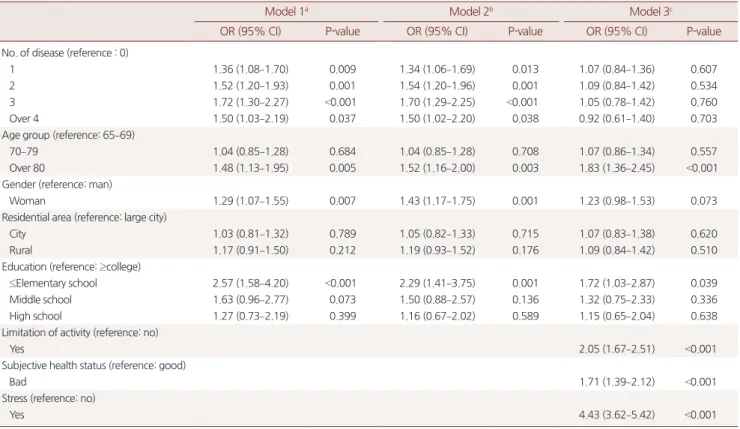
).Table 4
는 누적질환개수의 자살생각에 대한 교차비와95
% 신뢰구간을 보여준다. 누적질환이
3
개인 군의 분석모형1
과2
에서 자살생 각 위험도가 유의하게 높았다(Model 1
,adjusted OR
,1
.72
;95
%CI
,1
.30–2
.27
;Model 2
,adjusted OR
,1
.70
;95
%CI
,1
.29–2
.25
). 분석모형1
과2
에서 누적질환개수가 증가할수록 위험도도 증가하나 누적질 환이3
개와4
개 이상에서는 역전된 결과를 보였다. 분석모형3
에서 는 누적질환개수와 자살생각 연관성은 다중이환의 경우와 같이 연 관성이 없었다.Table 4. The association between the cumulative number of diseases and suicidal ideation
Model 1a Model 2b Model 3c
OR (95% CI) P-value OR (95% CI) P-value OR (95% CI) P-value
No. of disease (reference : 0)
1 1.36 (1.08–1.70) 0.009 1.34 (1.06–1.69) 0.013 1.07 (0.84–1.36) 0.607
2 1.52 (1.20–1.93) 0.001 1.54 (1.20–1.96) 0.001 1.09 (0.84–1.42) 0.534
3 1.72 (1.30–2.27) <0.001 1.70 (1.29–2.25) <0.001 1.05 (0.78–1.42) 0.760
Over 4 1.50 (1.03–2.19) 0.037 1.50 (1.02–2.20) 0.038 0.92 (0.61–1.40) 0.703
Age group (reference: 65–69)
70–79 1.04 (0.85–1.28) 0.684 1.04 (0.85–1.28) 0.708 1.07 (0.86–1.34) 0.557
Over 80 1.48 (1.13–1.95) 0.005 1.52 (1.16–2.00) 0.003 1.83 (1.36–2.45) <0.001
Gender (reference: man)
Woman 1.29 (1.07–1.55) 0.007 1.43 (1.17–1.75) 0.001 1.23 (0.98–1.53) 0.073
Residential area (reference: large city)
City 1.03 (0.81–1.32) 0.789 1.05 (0.82–1.33) 0.715 1.07 (0.83–1.38) 0.620
Rural 1.17 (0.91–1.50) 0.212 1.19 (0.93–1.52) 0.176 1.09 (0.84–1.42) 0.510
Education (reference: ≥college)
≤Elementary school 2.57 (1.58–4.20) <0.001 2.29 (1.41–3.75) 0.001 1.72 (1.03–2.87) 0.039
Middle school 1.63 (0.96–2.77) 0.073 1.50 (0.88–2.57) 0.136 1.32 (0.75–2.33) 0.336
High school 1.27 (0.73–2.19) 0.399 1.16 (0.67–2.02) 0.589 1.15 (0.65–2.04) 0.638
Limitation of activity (reference: no)
Yes 2.05 (1.67–2.51) <0.001
Subjective health status (reference: good)
Bad 1.71 (1.39–2.12) <0.001
Stress (reference: no)
Yes 4.43 (3.62–5.42) <0.001
OR, odds ratio; CI, Confidence interval.
aModel 1: adjustments for age group, gender, residential area, national basic livelihood, education level, living status and employment status. bModel 2: same as model 1+adjustments for physical activity, high risk drinking, current smoking and less than 6 hours sleep. cModel 3: same as model 2+adjustments for limitation of activity, subjective health status and stress.
Table 5. Subgroup analysisa
by education level
Education level
≤Elementary school
P-value Middle school
P-value High school
P-value ≥College
P-value
OR (95% CI) OR (95% CI) OR (95% CI) OR (95% CI)
Multimorbidity 1.36 (1.14–1.63) 0.001 1.23 (0.70–2.15) 0.478 1.27 (0.68–2.37) 0.462 0.67 (0.23–1.77) 0.419 No. of disease (reference: 0)
1 1.40 (1.07–1.83) 0.014 1.10 (0.51–2.34) 0.809 1.00 (0.79–2.03) 0.992 1.79 (0.47–6.77) 0.391
2 1.65 (1.24–2.19) 0.001 1.40 (0.61–3.21) 0.424 1.03 (0.45–2.36) 0.942 0.37 (0.07–2.14) 0.267
3 1.80 (1.30–2.51) 0.015 1.21 (0.44–3.32) 0.717 1.27 (0.45–3.61) 0.648 1.95 (0.48–7.85) 0.349
Over 4 1.42 (0.93–2.17) 0.103 1.09 (0.32–3.77) 0.890 2.78 (0.70–11.1) 0.148 2.71 (0.22–34.04) 0.440
OR, odds ratio; CI: confidence interval.
aSame as Model 2, with adjustments for age group, gender, residential area, national basic livelihood, education level, living status, employment status, physical activity, high risk drinking, current smoking and less than 6 hours sleep.
한요한 외. 신체질환의 다중이환과 자살생각
Korean Journal of Family PracticeKJFP
Table 5
는 인구사회학적변수와 건강행동변수로 보정하여 시행한교육수준에 대한 하위그룹분석결과를 보여준다. 초등학교 졸업 이 하의 군에서만 다중이환과 자살생각 위험도가 유의하게 나타났다 (
adjusted OR
,1
.36
;95
%CI
,1
.14–1
.63
). 누적질환이3
개인 경우 자살 생각 위험도가 가장 높게 나타났다(adjusted OR
,1
.80
;95
%CI
,1
.30–
2
.51
). 학력이 높아질수록 누적질환개수가 유의하게 낮아졌다 (Supplement 2
).Table 6
은 인구사회학적변수와 건강행동변수를 보정하여 시행한건강상태변수에 대한 하위그룹분석결과를 보여준다. 활동제한과 주관적 건강상태 여부에 대한 하위그룹분석에서는 다중이환 또는 누적질환개수와 자살생각 사이의 연관성이 없었다. 반면, 스트레스 가 없는 군은 추가 보정 전보다는 비교위험도가 감쇠하였지만 누적 질환이
2
개 이상일 경우, 즉, 다중이환 시 자살생각 위험도가 높았 다(adjusted OR
,1
.27
;95
%CI
,1
.02–1
.59
). 마찬가지로 우울감이 없는 군에서 다중이환된 경우와 누적질환3
개까지 유의한 증가를 보였으 나(adjusted OR
,1
.28
;95
%CI
,1
.05–1
.56
) 누적질환이4
개 이상인 경 우 자살생각과 연관성이 없었다.고 찰
본 연구에서는 노인을 대상으로 신체질환의 다중이환과 자살생 각 사이에 인구사회학적변수와 건강행동변수를 보정한 경우 유의 한 연관성이 관찰되었으나 건강상태변수를 추가 보정한 경우 연관 성을 보이지 않았다. 교육수준과 건강상태변수에 대해 시행한 하위 그룹 분석에서는 다중이환되었으나 스트레스나 우울감이 없는 경 우와 초등학력 이하인 경우에서만 유의한 연관성이 있었다. 이러한 결과는 누적질환개수가 많아질수록 활동의 제약이 더 생기고 주관 적 건강상태는 나쁘다고 느끼며 우울감을 더 호소하는 등 다중이환 과 건강상태변수간의 유의한 상관관계(
Supplement 1
)로 인한 것으로 보인다. 이러한 다중이환과 정신건강상태의 연관성은 이전 연구에 서 관찰되었다.2,16,22-24) 교육수준이 낮을수록 다중이환율이 높다는 보고25)와 교육수준이 낮을수록 자살생각 경험율이 증가하는 경향 이 있다는 이전 연구3)와 같이 본 연구에서도 교육수준이 낮을수록 누적질환개수가 유의하게 증가하였으며(Supplement 2
) 낮은 교육수 준에서 다중이환된 경우 자살생각의 위험도가 높았다.신체질환과 자살생각의 연관성에 대하여 상반된 연구 결과들2,17,18,20,25,26)
이 있어 본 연구는 자살생각의 위험도가 매우 높은 우울증을 진단 받은 노인은 제외하여 신체질환의 다중이환과 자살생각 연관성을 분석하였다. 청소년 자살이 대게 단일 요인에 의해 발생하는데 반하
여 노인 자살은 연령, 성별, 교육수준, 직업유무, 경제적 어려움, 스 Table 6.
Subgroup analysisa by limitation of activity, subjective health status, stress and depressiveness Limitation of activitySubjective health statusStressDepressiveness Yes P-valueNo P-valueGood P-valueBad P-valueYes P-valueNo P-valueYes P-valueNo P-value OR (95% CI)OR (95% CI)OR (95% CI)OR (95% CI)OR (95% CI)OR (95% CI)OR (95% CI)OR (95% CI) Multimorbidity1.18 (0.89–1.58)0.2541.15 (0.93–1.42)0.1971.20 (0.94–1.54)0.1420.95 (0.75–1.20)0.6501.21 (0.93–1.58)0.1541.27 (1.02–1.59)0.0321.31 (0.95–1.82)0.1021.28 (1.05–1.56)0.016 No. of disease (reference: 0) 11.48 (0.94–2.31)0.0901.15 (0.87–1.52)0.3241.14 (0.85–1.53)0.3901.21 (0.83–1.77)0.3311.15 (0.78–1.70)0.4851.26 (0.92–1.72)0.1471.05 (0.68–1.63)0.8211.40 (1.04–1.89)0.028 21.48 (0.90–2.41)0.1191.34 (1.01–1.78)0.0461.25 (0.90–1.74)0.1881.13 (0.77–1.67)0.5291.36 (0.91–2.03)0.1361.38 (1.01–1.89)0.0451.36 (0.85–2.17)0.1941.53 (1.13–2.08)0.006 31.85 (1.09–3.14)0.0221.08 (0.74–1.57)0.7021.29 (0.82–2.04)0.2741.19 (0.78–1.83)0.4191.22 (0.75–2.00)0.4221.65 (1.13–2.40)0.0101.59 (0.91–2.77)0.1051.59 (1.12–2.25)0.009 Over 41.25 (0.72–2.19)0.4291.12 (0.67–1.88)0.6711.59 (0.80–3.17)0.1870.76 (0.46–1.28)0.3051.46 (0.76–2.79)0.2531.38 (0.81–2.34)0.2360.97 (0.45–2.08)0.9321.57 (0.99–2.49)0.056 OR, odds ratio; CI: confidence interval. aSame as Model 2, with adjustments for age group, gender, residential area, national basic livelihood, education level, living status, employment status, physical activity, high risk drinking, current smoking and less than 6 hours sleep.
Yo Han Han, et al. Multimorbidity and Suicidal Ideation
Korean Journal of Family Practice
KJFP
트레스와 우울, 사회적 배제, 고독과 사별, 삶의 만족도, 활동제한, 신체질환 유무, 신경인지장애, 신체질환과 통증, 심리적 아픔 등 여 러가지 요인들이 다양하고 복합적으로 작용하여 발생한다.8,27,28) 노 인 자살위험인자에 대한 연구에서 건강에 대한 주관적 인식이 진단 받은 질환 유병보다 더 중요한 요소로 평가된다.3) 본 연구에서는 다 중이환 시
56
.4
%가 누적질환개수4
개 이상 시39
%가 주관적 건강상 태가 좋다고 응답하였다. 주관적 건강상태에 대한 하위그룹분석에 서는 다중이환과 자살생각 간 통계적으로 유의미한 결과는 보이지 않았다. 또한 다중이환 시 우울감과 스트레스가 없는 경우 다중이 환과 자살생각과 연관성이 있었으나 우울감과 스트레스가 있다면 연관성이 없었다. 이전 연구에서 다중이환 시 인지된 스트레스가 많 을수록 사망률이 높고29) 이환 질환에 주관적 평가가 나쁜 경우 자살 생각 위험이 높다고 한다.2) 다중이환된 노인의 자살생각에는 사회 인구학적변수와 건강행동변수보다 건강상태에 대한 주관적인 평가 가 유의미하게 영향을 미친다고 볼 수 있겠다.본 연구에는 몇 가지 제한점이 있다. 첫째, 단면 연구로 진행되어 다중이환과 자살생각 간의 시간적 선후관계를 파악하는 데에는 한 계가 있으므로 원인적 연관성 평가에 주의가 필요할 것으로 보인다.
둘째, 연령이 증가할수록 신체 기능이 떨어지고 노쇠(
fragility
)하게 되어 노화와 만성 질환에 따른 변화로 인하여 스트레스에 적절히 대응하지 못하는 상태가 된다. 최근 제시되는 다중이환 정의를 보면 노쇠를 포함하여 인지, 감각장애와 만성통증까지 만성적인 건강 상 태를 평가하도록 한다.12) 노인을 대상으로 하는 본 연구에서 협소한 범위로 다중이환을 정의하여 다중이환율이 과소 또는 과대평가되 었을 수가 있겠다. 셋째, 조사연도별 자살생각 경험을 묻는 설문 문 항 차이가 있다.6
기2
차(2014
년)는 자살생각 경험 기간이 ‘지난2
주’로 ‘최근
1
년’인 다른 연도와 달라 분석에서 제외하였으나5
기는 “최 근1
년 동안 죽고 싶다는 생각을 해본 적이 있습니까?”,6
기1
차 (2013
년) “최근1
년 동안 진지하게 자살을 생각한 적이 있습니까?”,6
기3
차(2015
년) “최근1
년 동안 심각하게 자살을 생각한 적이 있습니 까?”로 조사연도마다 문항 문구 변경이 있어 조사 결과 차이가 있을 수가 있겠다.결론적으로 다중이환된 노인은 자살생각의 확인, 평가와 관리가 필요하며, 특히 초등학교 졸업 이하의 학력을 가진 경우 관심이 더 필요하고, 우울증을 진단받지 않은 다중이환된 노인에서도 정신건 강상태 평가에 집중해야 함을 시사한다.
요 약
연구배경: 최근 다중이환과 자살경향 사이의 연관성에 대해 보고
되었고, 본 연구는 신체질환의 다중이환과 자살생각 간의 연관성을 평가하기 위해 수행되었다.
방법: 연구 대상자는 국민건강영양조사 제
5
기, 제6
기(1
,3
차)에서 이 전에 우울증을 진단받지 않은65
세 이상의 노인6
,712
명이었다. 다 중이환은 한 개인이2
개 이상의 만성질환을 가진 것으로 정의하였 다. 다중이환과 자살생각 간의 연관성을 평가하기 위하여 다변량 로지스틱 회귀분석을 시행하였다.결과:
2
,704
명,40
.7
%가 다중이환되었고978
명,14
.6
%가 자살생각을 경험하였다. 다중이환과 자살생각은 사회인구학적 변수와 건강행동 변수를 보정하였을 때 연관성을 보였다(교차비:1
.33
,95
% 신뢰도:1
.14–1
.55
). 하지만 건강상태에 대한 변수를 추가 보정한 경우 다중 이환과 자살생각의 연관성은 없었다. 교육수준에 따른 하위그룹분 석에서는 초등학교 졸업 이하인 군에서 자살생각 위험도가 높았으 며(교차비,1
.36
;95
% 신뢰구간,1
.14–1
.63
) 건강상태에 따른 하위그 룹분석에서는 스트레스가 없는 군과 우울감이 없는 군에서 다중이 환과 유의한 연관성을 보였다(교차비,1
.27
;95
% 신뢰구간,1
.02–
1
.59
; 교차비,1
.28
;95
% 신뢰구간,1
.05–1
.56
).결론: 본 연구 결과는 다중이환된 노인은 자살생각의 확인, 평가 및 관리가 필요하며 특별히 초등학교 졸업 이하의 학력을 가진 경우 특 별한 관심이 필요하며 또한 의료인들은 우울증을 진단받지 않은 다 중이환된 노인의 정신건강상태 평가에 집중해야 함을 시사한다.
중심단어: 자살생각; 다중이환; 노인; 한국 CONFLICT OF INTEREST