Received: December 12, 2015 Revised: December 18, 2015 Accepted: December 24, 2015
Corresponding Author: Dong-Ju Lim, Department of Orthopaedic Surgery, Seoul Spine Institute, Sanggye Paik Hospital, Inje University College of Medicine, Dongil-ro 1342, Nowon-gu, Seoul 01757, Korea
Tel: +82-2-950-1288, Fax: +82-2-950-1287, E-mail: [email protected]
골다공증성 척추 골절 환자에서 생존 분석을 통한 골다공증 약물 복용 지속률과 복용 인자
인제대학교 상계백병원 정형외과 척추센터1, 인제대학교 해운대백병원 정형외과 척추센터2
김성수2․임동주1․김진혁1․김순규1․오승렬1․석세일1
Medication Persistence for Osteoporosis and Its Related Factor in Patients with Osteoporotic Compression Vertebral Fracture
Sung-soo Kim2, Dong-Ju Lim1, Jin-Hyok Kim1, Sun-kyu Kim1, Seung-yeol Oh1, Se-il Suk1
1Department of Orthopaedic Surgery, Seoul Spine Institute, Sanggye Paik Hospital, Inje University College of Medicine, Seoul,
2Department of Orthopaedic Surgery, Spine Institute, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea
Introduction: Osteoporotic vertebral fractures, which account for the largest part of the disease has become important and common diseases. We studied persistence for osteoporosis medication and its related factor in patients with osteoporotic compression vertebral fracture.
Methods: A total of 458 patients that visited our outpatient clinic with osteoporotic vertebral fractures and were prescribed with osteoporosis medication at the Seoul Spine Center from January 2010 to February 2014 and were analyzed retrospectively. The male to female ratio was 403: 55 and the mean age was 75 years. Survival analysis was used with the Kaplan-Meier method. Related factor analysis was performed with the log rank test and Cox regression test.
Results: The survival rate at 6 months was 52%, 12 months was 40%, 24 months was 28%, and at 3 years it was 25%. There was no difference between the persistent rate according to age. Women demonstrated higher persistent rate than men in significantly. It showed a significant difference between some of the groups in accordance with the dose rate and duration of the drug dose interval. Especially, medication change group had significant higher persistence rate than not changing group.
Conclusions: Persistence rate of osteoporosis drugs, decreased rapidly with the passage of time. The patients with changing medication during follow-up had significantly higher persistence ratio than those without it. The persistence rate of osteoporosis medication could be increased through actively solving the problems of the patients, which are associated with taking medication.
Key Words: Osteoporosis compression vertebral fracture, Osteoporosis medication, Persistence, Osteoporosis
급속한 노령화로 인한 우리나라 전체 인구 비율 중 노인 인구가 차지하는 비율은 급속도로 증가하고 있으며 만성 질환 특히 폐경기의 여성에서 발생하는
질환에 대한 치료와 연구에 많은 발전이 있어 왔다.
이에 따라 골다공증은 가볍게 여길 수 없는 중요한 질환의 하나로 자리잡게 되었으며 이와 동반한 많은
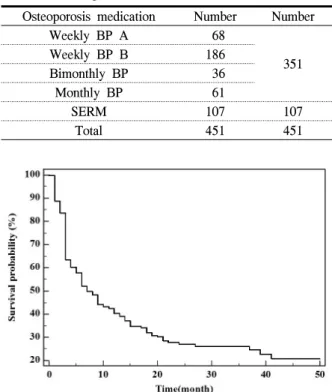
Table 1. Osteoporosis medication distribution Osteoporosis medication Number Number
Weekly BP A 68
Weekly BP B 186 351
Bimonthly BP 36
Monthly BP 61
SERM 107 107
Total 451 451
Fig. 1. Survival rate of osteoporosis medication persistence 질병의 부분을 차지하고 있는 골다공증성 척추 골절
은 중요하며 흔한 질환이 되었다.1 골다공증성 척추 골절은 고관절 골절과는 달리 발생시 즉각적으로 병 원을 찾지 않는 경우가 흔하고, 골절의 치료와 동시 에 골다공증의 치료가 같이 이루어져야 하기 때문에 더욱 치료하기 쉽지 않은 질환이다. 또한 골절이 발 생되기 이전에 골다공증 악화가 서서히 이루어지며, 타 골절에 비교하여 증상이 비교적 경미한 골다공증 성 척추 골절에서 처방 약물 복용 시에는 장기간의 약물 복용 지속성(adherenece)이 중요하다고 할 수 있다. 하지만 골다공증성 척추 골절의 치료 약제의 복용 지속률을 지속시킬 수 있는 방법에 대한 연구 를 진행한 논문은 국내에서는 찾아 볼 수 없는 실정 이다.
이에 저자들은 골다공증성 척추 압박 골절로 내원 하여 골다공증 약물 치료를 받는 환자의 골다공증성 약제 간의 생존 분석을 통한 골다공증 약물 복용 지 속률과 복용 인자의 분석을 통하여 골다공증약의 복 용 지속률을 높일 수 있는 방법을 찾아보고자 하였 다.
대상 및 방법
본 연구는 2010년 1월부터 2014년 2월까지 본원 척추센터에 골다공증성 척추골절(osteoporotic com- pression fracture)로 외래에 내원한 458명의 환자 중 골다공증 약(osteoporosis medication)을 처방 받은 환 자를 후향적으로 분석하여 약물의 복용 지속률에 대 한 생존분석을 하였다. 여자는 403명이었으며, 남자 는 55명, 평균 연령은 75세(range: 50-95)였다. 추시 기간은 골다공증 약물 복용을 개시한 시점에서 지속 한 기간으로 하였으며 평균 13.8개월(3개월-50개월) 이었다. 외래에 내원한 척추 골절 환자에게 골다공 증약을 처방한 일수를 따져 마지막 약물을 처방 받 아간 이후 3개월 이상 외래 추시 관찰이 되지 않거 나, 약물을 처방 받지 않은 환자에 대해서는 약물 지 속 중단으로 판단 하였다. 각각의 환자에 대해서 통 계적 처리는 MedCalc version 14.8.1 (MedCalc Software, Mariakerke, Belgium)를 이용하여 생존 분석 은 Kaplan-Meier법을 사용하였으며, 단일 인자 분석
은 Log-rank검정, 그리고 다중인자분석으로는 Cox proportional hazard regression을 시행하여 골다공증약 복용 지속률, 연령별, 성별에 따른 차이, 약물 복용 간격 및 약물 종류, 복용약 변경 유무, 처방의사에 따른 차이를 분석하였다. P값이 0.05보다 작은 경우 에 유의한 것으로 평가하였다.
결 과
본원에 골다공증성 척추 골절로 최초 내원 후에 처방된 약제는 제제별로는 비스포스포네이트 제제 가 351예, 선택적 에스트로겐 수용체 조절제가 107 예로 관찰되었으며, 비스포스포네이트 제제별로는 주1회 투여 제제가 254예, 월 2회 투여 제제가 36예, 월 1회 투여 제제가 61예, 선택적 에스트로겐 수용 체 조절제 제제는 107예였다(Table 1).
골다공증 약물 복용 지속률에 있어서 전체적 복용 지속률은 6개월 52%, 12개월 40%, 24개월 28%, 36 개월에 25%로 급격한 감소를 보였다(Fig. 1). 평균 연령인 75세의 전후로의 연령별에 따른 복용 지속률
Fig. 2. Survival rate of age difference (P=0.139)
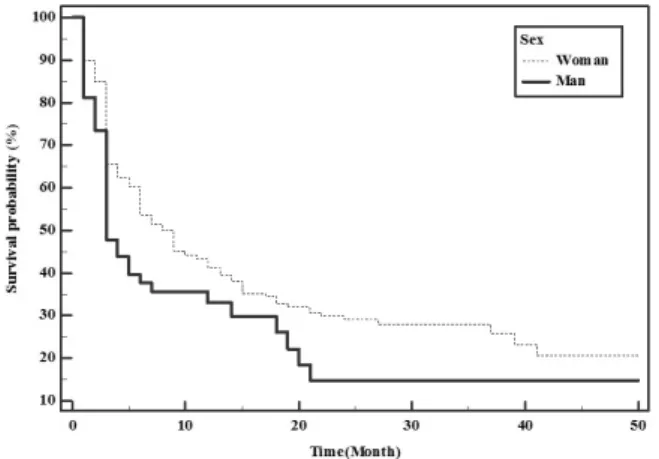
Fig. 3. Survival rate according to Gender difference (P=0.038)
Fig. 4. Survival rate according to osteoporosis medication (P=0.014)
Fig. 5. Difference of survival rate between Bisphosphonate and SERM medication (P=0.008)
Fig. 6. Difference of survival rate between weekly bisphos- phonate and monthly Bisphosphonate (P=0.139) 의 차이(P=0.1393, Fig. 2)는 없었으나 성별에 따른
복용 지속률은 여성환자에서 남성보다 복용 지속률 이 의미 있게 높음을 알 수 있었다(P=0.038, Hazard ratio=1.39, CI=0.9503 to 2.0499, Fig. 3).
약물에 따른 복용 지속률과 복용 간격에 따른 일 부 그룹 간에 의미 있는 차이(Fig. 4)를 보였는데 선 택적 에스트로겐 수용체 조절제 제제가 비스포스포 네이트 제제보다 복용 지속률이 높았으며(P=0.008, Fig. 5), 주 1회 복용하는 비스포스포네이트 제제와 월 1회 복용하는 비스포스포네이트 제제 사이에는 차이가 없었다(P=0.139, Fig. 6). 약물 변경을 하였던 경우는 총 45예에서 관찰되었고 바꾸기 전 약물은 선택적 에스트로겐 수용체 조절제 제제 1예를 제외 한 모든 경우에서 비스포스포네이트 제제였다. 변경 약제 중 처방 빈도가 가장 많았던 것은 주 1회 투여 하는 3세대 비스포스포네이트 제제와 매일 투여하
는 선택적 에스트로겐 수용체 조절제 제제가 각각 15례로 같았다. 특히 복용약 변경 유무에 따른 복용
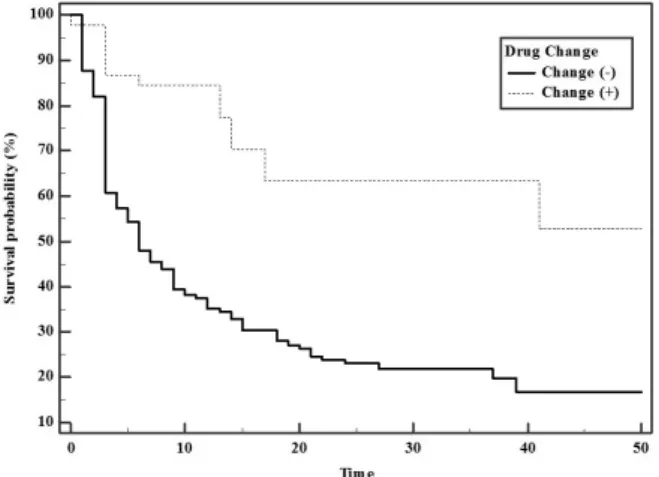
Fig. 7. Difference of survival rate between drug change group and no change group (P<0.0001)
지속률은 변경을 해주었던 그룹에서 변경을 해주지 않았던 그룹보다 지속률이 월등히 높았다(P<0.0001, Fig. 7).
고 찰
약물 복용 부착(adherence), 즉 순응(compliance)은 같은 말로 환자가 제대로 정해진 약을 용량과 용법, 간격에 맞게 잘 복용되었는지 아는 것이고 복용 지 속(persistence)은 환자의 복용 지속률로 환자의 복용 지속 정도를 파악하는 것이다.2-4 이를 알아내기 위 해서 Medication Possetion Ratio (MPR) 등 여러 가지 방법들이 개발되어 있지만 이는 자본과 시간, 인력 에 비해 정확하지도 않고 효율적이지도 못하다.5 대 신 외래에서 정기적으로 약을 복용하기 위해서 내원 하는 환자들을 대상으로 최소 3개월 이상 약물을 중 단하지 않고 지속적으로 약제 처방을 받는다면 지속 적인 복용을 한다고 판단하여 이를 이용하여 생존 분석을 하여 약물들 간의 지속률 차이, 복용 간격에 따른 지속률 차이, 환자의 복용인자 등에 따른 차이 를 생존 분석을 이용한 통계적 분석을 통해 골다공 증성 척추 골절 환자들의 치료에 적극 적용하고자 본 연구를 진행 하였다. 골다공증 약제를 복용하는 환자에서 약제 복용률과 지속률이 떨어짐에 따라 골 절의 위험률이 유의하게 증가하고 의료 비용이 증가 하는 것에 대한 결과는 이미 여러 연구에서 밝혀져 질환에 대한 골다공증 약제의 지속적인 복용이 2차
골절 예방에 중요한 것은 이미 알려 있는 사실이다.6-9 골다공증을 가지고 있으면서 치료하지 않아 골절이 발생한 뒤 6개월째부터 골다공증의 치료를 시행하 게 되더라도 환자에게 상당한 비용의 절감뿐만 아니 라 수명의 연장이라는 진전을 보였다는 연구 결과는 이를 뒷받침하는 것이다.10
골다공증 약제를 중단하게 되는 원인 인자에 대해 서 여러 연구가 진행되어 왔는데 환자는 대부분 임 의로 비스포스포네이트 제제를 중단하지 않으며, 중 단을 하는 이유는 부작용11과 다른 요소들, 예를 들 면 증상의 자각 정도가 경미한 경우, 제대로 된 치료 를 받았을 경우에 얻을 수 있는 잠재적인 위험 대비 이익과 결과에 대한 무지, 교육의 부족함, 약제에 의 한 경제적인 부담, 부작용 등에 대한 두려움 등 여러 가지가 있을 수 있다고 보고되고 있다.4
그러나 의료인의 적극적인 교육, 정보, 일관된 치 료가 이를 지속률을 높일 수 있는 중요한 부분을 차 지한다는 여러 보고가 있는데6,11-14 본 연구에서도 외 래에서 환자에게 적극적인 상호 작용을 통한 약제 교환군에서 더 높은 복용 지속률을 확인 할 수 있었 다. 통상적인 만성 질환에 대한 약물 복용의 지속성 에서도 환자에게 진단에 대한 교육과 장기 치료 및 지속성의 중요성, 용량의 정확한 용법에 대한 교육 이 중요하다는 것은 이미 밝혀졌으며 골다공증의 약 제 복용에도 이는 마찬가지인 것으로 여러 논문에서 연구 되었다.3,15-17 Jackie 등은 생존분석을 통하여 간 호사를 이용한 골다공증 환자 모니터링을 시행하였 을 때 모니터링을 전혀 시행하지 않은 군과 표지자 를 이용한 모니터링을 시행하였을 때보다 57% 높은 약물 복용 지속률을 보였다고 하였으며18 부갑상선 호르몬의 투여 시 등록 관리 및 교육을 시행한 환자 에서 1년 약물 지속률이 87%에나 달하는 보고가 있 는 것은 역시 환자에 대한 관심이 필요하다는 것을 시사하는 점이다.19 본 연구에서도 약제 변경을 통한 환자관리를 했던 경우에 복용률이 그렇지 않았던 군 에 비해 3.8배 높았던 것으로 분석되었다(P<0.0001, Hazard ratio=3.8140, CI=2.7033 to 5.3812).
골다공증 약제 복용의 지속률을 높이기 위해서 여 러 가지 검사를 통한 관리 역시중요하다고 알려져 있는데, 그 중 폐경기 여성의 골다공증 환자의 진료
시 골 대사 표지자(bone turnover maker)를 사용하여 약제 반응률에 따른 처방은 약제 복용의 지속률을 강화하는 것으로 알려져 있다.20 본 연구에서는 척추 골절로 인하여 외래에서 골다공증약을 처방을 받는 모든 환자에게 우리나라의 보험 규정에 따라 1년에 1번씩 고관절 경부 또는 척추 부위에 대한 골밀도 검사(BMD)를 시행하여 현재 골밀도에 대한 판단을 하면서, 환자 약물 복용시의 문제점 등에 대한 관리 및 환자에 대한 약물 복용과 관련한 문제점을 적극 적으로 확인하고, 진료시 환자 교육을 하였다.
약물 복용 지속률을 높이기 위해 복용 간격과 약 물 용량에 따른 연구도 많이 진행되고 있는데 주 1 회 비스포스포네이트 제제의 복용 지속률이 월 1회 비스포스포네이트 제제의 복용 지속률보다 더 우위 에 있어 골절 예방에 더욱 도움이 될 것이라 보고한 몇몇 연구2,21,22가 있었으나 본 연구에서는 이와는 상 반되게 차이를 보이지 않았고(P=0.139), 매일 투여하 는 약제보다는 일주일에 한번 투여하는 약제의 약물 복용 지속률이 더 높다고 보고되어 빈번히 투여되는 약제보다는 간격을 두고 투여하는 약물이 더 높은 것으로 보고되어 있으나2 이번 연구에서는 위의 연 구와는 상반된 결과를 보였는데 주간 투여 또는 월 간 투여를 하는 비스포스포네이트 제제를 투여한 군 이 매일 선택적 에스트로겐 수용체 조절제 제제를 투여한 군에서 보다 지속률(persistence)이 오히려 떨 어지는 현상을 보였다(P=0.0008, Fig. 5).
미국의 대량 연구에서 고관절 골절의 남자 환자에 게 골다공증약제 처방률은 상당히 낮은 것으로 알려 져 골다공증을 가지고 있는 남자 환자의 약 1/3이하 에서 처방이 되는 것으로 보고되고 있으며, 골절이 있었던 경우에는 이후 약제를 매일 처방하는 선택적 에스트로겐 수용체 조절제 제제나 주 단위로 투여하 는 비스포스포네이트 제제 계열의 약제로 시작한 경 우에 지속률의 향상이 있었다는 연구 결과가 있었 다.23 본 연구에서는 남자의 골다공증 복용률과 지속 률은 여자에 비해서 현저히 떨어지는 것으로 관찰 되어 아직까지 남성의 골다공증에 대한 경각심이나 사회적 관심도는 떨어지는 것으로 생각된다(P<
0.05, Fig. 3)
결 론
골다공증환자에서 조사한 골다공증약의 복용 지 속률은 시간이 소요됨에 따라 급격히 저하됨을 관찰 하였고, 복용약을 변경해주었던 경우에 그렇지 않는 경우에 비해 약물 지속률이 의미있게 높았음을 알 수 있었다. 본 연구에서 저자들은 처방의사가 복용 약과 관련한 환자의 문제점을 외래 추시에서 단순히 같은 골다공증 약물을 반복하여 처방하는 것뿐만 아 니라 약물 복용하는 과정에 불편함이 없는지, 부작 용이 없는지 등을 꼼꼼하게 환자에게 묻고 그것을 적극적으로 피드백을 통한 교육 등으로 상호 행동을 한다면 골다공증 약물의 지속성을 의미 있는 높일 수 있다는 것을 보여 주는 중요한 부분으로 환자의 요구에 대한 적극적 해소를 통해 골다공증 약물 복 용의 지속률을 높일 수 있을 것으로 생각되며 이를 실제 임상에 잘 적용할 수 있을 것으로 생각된다.
참 고 문 헌
1. Choi YJ, Oh HJ, Kim DJ, Lee Y, Chung YS. The prevalence of osteoporosis in Korean adults aged 50 years or older and the higher diagnosis rates in women who were beneficiaries of a national scree- ning program: the Korea National Health and Nutrition Examination Survey 2008-2009. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research 2012;27:1879-86.
2. Cramer JA, Amonkar MM, Hebborn A, Altman R.
Compliance and persistence with bisphosphonate dosing regimens among women with postmeno- pausal osteoporosis*. Current Medical Research and Opinion 2005;21:1453-60.
3. Barbosa CD, Balp M-M, Kulich K, Germain N, Rofail D. A literature review to explore the link between treatment satisfaction and adherence, com- pliance, and persistence. Patient Prefer Adherence 2012;6:39-48.
4. Lars Osterberg, Terrence Blaschke. Adherence to
medication. The new england Journal of Medicine 2005.
5. Andrade SE, Kahler KH, Frech F, Chan KA.
Methods for evaluation of medication adherence an persistence using automated databases. Pharmaco- epidemiology and Drug Safety 2006;15:565-74.
6. Sunyecz JA, Mucha L, Baser O, Barr CE, Amonkar MM. Impact of compliance and persis- tence with bisphosphonate therapy on health care costs and utilization. Osteoporosis International 2008;19:1421-9.
7. Rabenda V, Mertens R, Fabri V, Vanoverloop J, Sumkay F, Vannecke C, et al. Adherence to bisphosphonates therapy and hip fracture risk in osteoporotic women. Osteoporosis International 2008;19:811-8.
8. Siris ES, Harris ST, Rosen CJ, Barr CE, Arvesen JN, Abbott TA, et al. Adherence to bisphosphonate therapy and fracture rates in osteoporotic women:
relationship to vertebral and nonvertebral fractures from 2 US claims databases. Mayo Clinic Proceedings: Elsevier 2006:1013-22.
9. Siris ES, Selby PL, Saag KG, Borgström F, Herings RMC, Silverman SL. Impact of Osteo- porosis Treatment Adherence on Fracture Rates in North America and Europe. American Journal of Medicine The 2009;122:S3-S13.
10. Majumdar SR, Johnson JA, Lier DA, Russell AS, Hanley DA, Blitz S, et al. Persistence, repro- ducibility, and cost-effectiveness of an intervention to improve the quality of osteoporosis care after a fracture of the wrist: results of a controlled trial.
Osteoporos Int 2007;18:261-70.
11. Ettinger B, Pressman A, Schein J, Chan J, Silver P, Connolly N. Alendronate use among 812 women:
prevalence of gastrointestinal complaints, noncom- pliance with patient instructions and discontinu- ation. J Managed Care Pharm 1998;4:488-92.
12. Carr AJ, Thompson PW, Cooper C. Factors asso- ciated with adherence and persistence to bisphos-
phonate therapy in osteoporosis: a cross-sectional survey. Osteoporosis International 2006;17:1638-44.
13. Penning-van Beest FJA, Goettsch WG, Erkens JA, Herings RMC. Determinants of persistence with bisphosphonates: A study in women with postme- nopausal osteoporosis. Clinical Therapeutics 2006;
28:236-42.
14. Gleeson T, Iversen MD, Avorn J, Brookhart AM, Katz JN, Losina E, et al. Interventions to improve adherence and persistence with osteoporosis medi- cations: a systematic literature review. Osteoporosis International 2009;20:2127-34.
15. Emkey RD, Ettinger M. Improving Compliance and Persistence with Bisphosphonate Therapy for Osteoporosis. Am J Med 2006 Apr;119(4 Suppl 1):
S18-24.
16. Cramer JA, Gold DT, Silverman SL, Lewiecki EM.
A systematic review of persistence and compliance with bisphosphonates for osteoporosis. Osteoporosis International 2007;18:1023-31.
17. Li L, Roddam A, Ferguson S, Feudjo-Tepie M, Taylor A, Jick S. Switch patterns of osteoporosis medication and its impact on persistence among postmenopausal women in the UK General Practice Research Database. Menopause 2014.
18. Clowes JA, Peel NFA, Eastell R. The Impact of Monitoring on Adherence and Persistence with Antiresorptive Treatment for Postmenopausal Osteoporosis: A Randomized Controlled Trial. The Journal of Clinical Endocrinology & Metabolism 2004;89:1117-23.
19. Arden N, Earl S, Fisher D, Cooper C, Carruthers S, Goater M. Persistence with teriparatide in patients with osteoporosis: the UK experience.
Osteoporosis International 2006;17:1626-9.
20. Delmas PD, Vrijens B, Eastell R, Roux C, Pols HAP, Ringe JD, et al. Effect of Monitoring Bone Turnover Markers on Persistence with Risedronate Treatment of Postmenopausal Osteoporosis. The Journal of Clinical Endocrinology & Metabolism
2007;92:1296-304.
21. Brankin E, Walker M, Lynch N, Aspray T, Lis Y, Cowell W. The impact of dosing frequency on compliance and persistence with bisphosphonates among postmenopausal women in the UK: evidence from three databases. Current Medical Research and Opinion 2006;22:1249-56.
22. Cotté F-E, Fardellone P, Mercier F, Gaudin A-F,
Roux C. Adherence to monthly and weekly oral bisphosphonates in women with osteoporosis.
Osteoporosis International 2009;21:145-55.
23. Roerholt C, Eiken P, Abrahamsen B. Initiation of anti-osteoporotic therapy in patients with recent fractures: a nationwide analysis of prescription rates and persistence. Osteoporosis International 2009;
20:299-307.