환축추체 후방 나사고정술 후 생긴 동정맥루
대구파티마병원 신경외과, 경북대학교 의과대학 진단방사선과학교실*
이혁기·조재훈·이성락·강동기·김상철·김용선*
= Abstract =
Arteriovenous Fistula after C1-2 Posterior Transarticular Screw Fixation
- --
- Case Report ----
Hyuk Gi Lee, M.D., Jae Hoon Cho, M.D., Sung Lak Lee, M.D., Dong Gee Kang, M.D., Sang Chul Kim, M.D., Yong Sun Kim, M.D.*
Department of Neurosurgery, Fatima Hospital, Taegu, Korea Department of Radiology,* Kyungpook National University, Taegu, Korea
osterior transarticular screw fixation for atlantoaxial instability due to trauma or rheumatoid arthritis provides immediate rigid fixation of the C1-2 vertebral segment while preserving motion between the occiput and C1.
This technique provides more resistance to translational and rotational forces than wiring technique. However, the technique of transarticular screw fixation is inherently demanding because of the complex anatomy of the occipitocervical region and vertebral artery(VA) at risk for arterial damage. VA injury may lead to serious subsequent neurological deficits and possibly death from bilateral VA injury. We report a case of a vertebral artery-to-epidural venous plexus fistula after posterior transarticular screw fixation which was treated with balloon occlusion.
KEY WORDS:Transarticular screw fixation・Arteriovenous fistula・Balloon occlusion.
서 론
경부의 굴곡, 신전, 측부 굴곡 및 축회전을 허용하는 환축 추체의 독특한 구조 때문에 환축추체 전위의 치료로서 외고 정술 및 내고정술에는 많은 어려움이 있다. Margel15)에 의 해 시행된 후방 나사고정술은 환축추체의 즉각적인 고정을 허용하며 생체 역학적으로 기존의 철사 고정술에 비해 견고 하여 류마티스성 관절염, 선천성 및 외상성 환축추체 전위 에 널리 쓰이고 있는 방법이다2)5-7)9)11-13)17)18)20)23)
. 그러나 환축추체의 해부학적 다양성, 즉 추골동맥의 경로와 환추와 축추의 횡돌공의 위치에 의하여 나사고정의 제약과 기술적 숙련이 필요하다9)23). 최근의 문헌 보고에서 환축추체 전위 환자의 20%에서 안전한 후방 나사고정술이 어려우며14)22), 수술 예 중 4.1%에서 추골동맥의 손상이 보고되었다24). 추 골동맥손상에 따른 후유증으로 1레의 사망, 1례의 동정맥루 및 2례의 소뇌경색이 보고되었으며, 그 외 합병증으로 불유
합, 경막 손상, 나사의 골절 및 변위, 감염, 후두하신경통, 설하신경통 등이 있다1)3)10)12)21)23)24)
. 저자들은 환축추체 후 방 나사고정술 후에 추골동맥에서 생긴 동정맥루를 치험하 였기에 문헌고찰과 함께 보고하는 바이다.
증 례
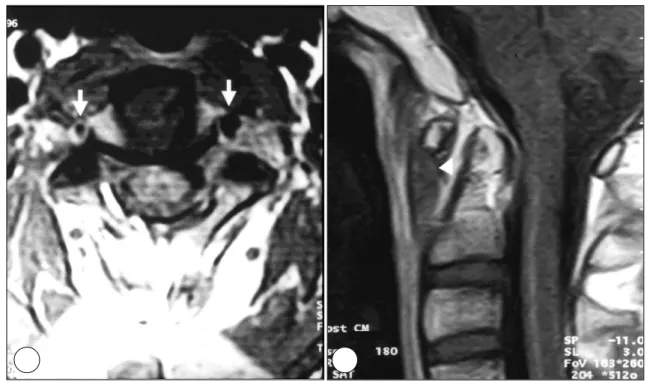
자동차 수리공인 28세의 건강한 남자 환자로 특이한 병 력이 없는 4개월 동안의 경부통증과 왼쪽 어깨부위의 저림 증세로 보전적인 치료를 시행하였으나 호전이 없어 내원하 였다. 신경학적 검사 상 사지의 운동 및 감각장애는 없었으 며, 류마티스성 질환을 의심할 만한 이학적 소견 및 혈액학 적 소견은 없었다. 경부방사선촬영 및 역동상촬영 상 환축 추돌기 간격이 굴곡 시 7mm, 신전 시 2mm인 환축추체 전 위를 보였으나(Fig. 1), 자기공명촬영에서 환축추 부위의 횡 인대와 양쪽 추골동맥의 이상은 없었다(Fig. 2).
Gardner-Wells tongs 견인을 이용한 경부 견인 후 Ha-
PPPP
이혁기 · 조재훈 · 이성락 · 강동기 · 김상철 · 김용선
lovest 견인을 3개월 동안 착용하였으나 경부 통증이 지속 되고, 경부방사선촬영 상 환축추체 전위가 지속되어 수술을 시행하였다. 수술 전 후두부에서 제3경추 상부까지 1mm 간 격의 나선형 전산화단층촬영으로 추골동맥의 경로와 횡돌공 의 위치를 확인한 뒤19) 방사선촬영 하에 오른쪽 후방 나사
고정술1)10)22)을 시행하였다. 왼쪽 나사고정술 시행 중 추골
동맥의 손상이 의심되는 출혈이 있어 나사고정술을 포기하 고 골랍으로 지혈시킨 뒤24), 극돌기간 철사고정술과 후방 골이식술5)을 시행하였다. 수술 후의 경부방사선촬영 상 오 른쪽 나사는 적절하게 위치하였다(Fig. 3). 2주일간의 입원
Fig. 2. A:Preoperative MR image showing relationship of C2 to vertebral artery(arrows). B:Preoperative MR image showing increased atlantodental interval(arrowhead).
Fig. 1. Lateral radiographs showing C1-2 instability. Atlanto-dental interval is 2mm during neck extension(A) and 7mm during neck flextion(B).
A A A
A BBBB
AA
AA BBBB
기간 중 후두 하부의 저림 증상을 호소하였으나 소뇌경색 증상은 보이지 않았고, 사지의 운동 및 감각 이상은 없었다.
수술 후 15주째 시행한 이학적 검사 상 경부통증은 완화 되었으며 경부방사선촬영 및 역동상촬영 상 이전 소견과 동 일하여 Philadelphia cervical collar의 착용을 중지하였다13). 이 후 경부통증이 악화되고 왼쪽 팔의 거상제한 및 운동장
애(3/5)를 보여 시행한 방사선촬영 상 나사의 골절이 있었 으며(Fig. 4), 근전도 검사 상 제3경추신경에서 제8경추신 경까지의 신경근병증이 의심되었다. 자기공명혈관촬영으로 제 2 경추체 하방에서 생긴 동정맥루와 척추강내 외경막 정 맥종괴가 확인되었다(Fig. 5). 선택적 혈관조영술로 동적맥 루와 정맥종괴를 확인하고(Fig. 6A), 15분 동안 추골동맥 패색검사를 하여 뇌혈관의 후방순환이 정상임을 확인한 뒤 (Fig. 6B), 왼쪽 추골동맥의 근위부와 동정맥루의 근위부 두 곳에 풍선색전술4)을 시술하였다(Fig. 6C).
시술 후 2주일 째 시행한 자기공명영상촬영에서 왼쪽 추 골동맥의 패색과 외경막 정맥종괴의 소멸이 있었으며(Fig.
7) 이학적 검사 상 경부통증과 왼쪽 어깨의 운동제한이 많 이 좋아져 팔의 거상 및 내·외전의 호전(4/5)을 보였다.
고 찰
환축추체의 독특한 구조 때문에 후방 나사고정술에는 해 부학적 구조의 확인 및 기술적 숙련이 필요하다. 1991년에 Grob 등7)은 161명의 환자에서 후방 나사고정술 후 아무런 합병증도 생기지 않았다고 보고하였다. Stillerman과 Wil- son23)도 22례의 후방 나사고정술 시행 후 추골동맥과 경추 신경의 손상은 없었다고 보고하였다. 그러나 Apfelbaum1) 은 1례의 양쪽 추골 동맥손상에 의한 사망을 보고하였고 Mar-
Fig. 3. Postoperative lateral(A) and anteroposterior(B) radiographs showing right unilateral screw placement with cable and bone fixation of the C1-2 spinous process.
AA
AA BB BB
Fig. 4. Lateral radiograph showing screw fracture(arrow).
이혁기 · 조재훈 · 이성락 · 강동기 · 김상철 · 김용선
Fig. 5. MR image(A) and MR angiography(B) showing left vertebral artery-anterior epidural vein fistula(arrow) and epidural venous mass(arrowheads).
Fig. 6. A:Angiography showing left vertebral artery-anterior epidural vein arteriovenous fistula(arrow). B:Occlusion test angiography showing left upper vertebral artery filling via right vertebral artery(arrowheads). C:Postinterventional angiography showing balloon occlusion of left vertebral artery(double arrow).
AA
AA BBBB
A A A
A BBBB CCCC
cotte 등16)은 2례의 경막손상을 보고하였으며 Coric 등14) 은 1례의 추골동맥손상에 의한 동정맥루를 보고하였다. 최 근의 해부학적 연구에서 20%의 환자에서 높이 위치한 횡 돌공 때문에 안전한 후방 나사고정술이 어렵다고 보고하였
으며9)21), 김 등10)과 송 등22)은 양쪽 후방 나사 고정술이 어
려울 경우 한쪽의 고정술로도 견고한 고정을 얻을 수 있다 고 보고하였다.
Wright와 Lauryssen24)은 후방 나사고정술을 시행한 환 자의 4.1%에서 추골동맥의 손상이 동반되며 0.2%에서 신 경손상이 생긴다고 보고하였다. 환축추체의 후방 나사고정 술 시행 시 추골동맥의 손상 및 신경손상을 피하기 위해 몇 가지 주의할 점이 있다. 수술 전 모든 환자에서 1mm 간격 의 전산화단층촬영을 환축추체 부위에 시행한 후 영상의 관 상면 및 시상명 재구성을 통하여 추골동맥의 주행과 축추의 관절간부와의 해부학적 관계를 밝혀야 한다. 수술 중에는 축추의 관절간부를 반드시 박리하여 나사가 환축추체의 관 절돌기를 지나 축체의 외측괴로 향하는지 확인하여야 하며 방사선촬영으로 나사의 정확한 궤도를 얻어야 한다. 만약 나사고정술 중 추골동맥의 손상이 생기거나 의심되는 경우 에는 골랍으로 지혈을 시키고 손상된 혈관의 복구 또는 결 찰을 고려할 수 있다.
또한 양쪽 추골동맥의 손상이 생기지 않도록 반대쪽 나
사의 고정은 시도하지 말아야 한다. 수술 후에는 일단 경과 를 관찰하다가 환자의 임상경과에 따라 치료하거나, 혈관조 영술을 시행하여 혈관손상을 확인하고 풍선색전술을 시도할 수 있다. 본 증례에서는 후방 나사고정술 후 경과를 관찰하 던 중 추골동맥에서 생긴 신경증상을 유발하는 동정맥루를 선택적 혈관조영술 및 추골동맥의 풍선색전술로 치료하였다.
결 론
환축추체의 전위에 대한 치료로서 후방 나사고정술은 즉 각적인 고정을 허용하는 생체 역학적으로 우수한 방법이나, 추골동맥의 주행경로와 횡돌공의 해부학적 다양성에 의해 시술의 제약과 기술적 숙련이 필요하다. 저자들은 후방 나 사고정술 후 추골동맥의 손상으로 생긴 1례의 외경막 정맥 종괴를 동반한 동정맥루를 풍선색전술로 치험하였기에 문헌 고찰과 함께 보고하는 바이다.
•논문접수일:1999년 7월 5일
• 심사완료일:1999년 9월 10일
•책임저자:이 혁 기
701-600 대구광역시 동구 신암동 302-1 대구 파티마병원 신경외과
전화:053) 940-7114, 전송:053) 954-7417 E-mail:[email protected]
Fig. 7. A:MR image showing balloon occlusion of left vertebral artery(arrow). B:MR angiography showing left upper vertebral filling via right vertebral artery(arrowheads).
AA
AA BBBB
이혁기 · 조재훈 · 이성락 · 강동기 · 김상철 · 김용선
References
1) Apfelbaum RI:Screw fixation of the upper cervical spine: Indication and technique. Contemp Neurosyrg 16(7):1-8, 1994 2) Brooks AL, Jenkins EB:Atlanto-axial arthrodesis by wedge compression method. J Bone Joint Surg(Am) 60:179-284, 1978
3) Cooper PR, Cohen A, Rosiello A, et al:Posterior of cervical spine fractures and subluxations using plates and screws. Ne- urosurgery 23:300-306, 1998
4) Coric D, Branch Jr CL, Wilson JA, et al:Arteriovenous fistula as a complication of C1-2 transarticular screw fixation.
J Neurosurg 85:340-343, 1996
5) Dickman CA, Sonntag VKH, Papadopoulos SB, et al:The interspinous method of posterior atlantoaxial arthrodesis. J Neurosurg 74:190-198, 1991
6) Grob D, Crisco JJ III, Panjabi MM, et al:Biomechanical evaluation of four different posterior atlantoaxial fixation tech- niques. Spine 17:480-490, 1992
7) Grob D, Jeannert B, Aebi M, et al:Atlato-axial fusion with transarticular screw fixation. J Bone Joint Surg(Br) 73:972- 976, 1991
8) Hanson PB, Montesano PX, Sharkey NA, et al:Anatomic and biomechanical assessment of transarticular screw fixa- tion for atlantoaxial instability. Spine 16:1141-1145, 1991 9) Jun BY:Anatomic study for ideal and safe posterior C1-2
transarticular screw fixation. Spine 23:1703-1707, 1998 10) Kim YS, Oh SH, Kim YS, et al:Transarticular screw fixa-
tion in atlantoaxial instability. J Korean Neurosurg 26:401- 406, 1997
11) Lee CH, Kim ES, Whang SH, et al:Surgical treatment of instability of upper cervical spine associated with trauma. J Korean Neurosurg 26:1659-1666, 1997
12) Lee GS, Oh SH, Kim SY, et al:Surgical management of atlantoaxial instability due to rheumatoid arthritis. J Korean
Neurosurg 26:934-939, 1997
13) Lee SH, Sung JK, Kim DH, et al:Posterior C1-2 tran- sarticular screw fixation on atlantoaxial instability. J Korean Neurosurg 26:1231-1236, 1997
14) Madawi AA, Casey ATH, Solanki GA, et al:Radiological and anatomical evaluation of the atlantoaxial transarticular screw fixation technique. J Neurosurg 86:961-968, 1997 15) Magerl F, Seemann PS:Stable posterior fusion of the atlas
and axis by transarticular screw fixation, in Kehr P, Weidner A(eds):Cervical Spine I. vienna:Springer-Verlag, 1987, pp322-327
16) Marcotte P, Dickmann CA, Sonntag VKH, et al:Posterior atlantoaxial facet screw fixation. J Neurosurg 79:234-237, 1993
17) Montesano PX, Juach EC, Anderson PA, et al:Biomechanics of cervical spine internal fixation. Spine 16(Suppl 3):S10- S16, 1991
18) Papadopoulos SM, Dickman CA, Sonntag VKH:Atlanto- axial stabilization in rheumatoid arthritis. J Neurosurg 74: 1-7, 1991
19) Paramore CG, Dickman CA, Sonntahg VKH:The anatomic suitability of the C1-2 complex for transarticular screw fixation.
J Neurosurg 85:221-224, 1996
20) Park HK:Posterior C1-2 transarticular screw fixation in at- lantoaxial instability. J Korean Neurosurg 23:310-315, 1994 21) Smith MD, Phillips WA, Hensinger RN:Complications of
fusion to the upper cervical spine. Spine 16:702-705, 1991 22) Song GS, Theodore N, Dickman CA, Sonntag VKH:Unila-
teral posterior atlantoaxial transarticular screw fixation. J Ne- urosurg 87:851-855, 1997
23) Stillerman CB, Wilson JA:Atlantoaxial stabilization with posterior transarticular screw fixation:technical description and report of 22 cases. Neurosurgery 32:948-955, 1993 24) Wright NM, Lauryssen C:Vertebral artery injury in C1-2 tr-
ansarticular screw fixation:results of a survey of the AANS/
CNS Scetion on Disorders of the Spine and Peripheral Nerves.
J Neurosurg 88:634-640, 1998