© 2016 The Korean Ophthalmological Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses /by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
108
Original Article
Short-term Clinical Outcomes after Transscleral Fixation Using the Intrascleral Pocket Technique: A Retrospective Cohort Study Analysis
Yong-Wun Cho1, Woong-Sun Yoo1, Inyoung Chung1,2, Seong-Wook Seo1,2, Ji-Myong Yoo1,2, Seong-Jae Kim1,2
1Department of Ophthalmology, Gyeongsang National University College of Medicine, Jinju, Korea
2Gyeongsang Institute of Health Science, Gyeongsang National University, Jinju, Korea
Purpose: To compare the two transscleral fixation (TSF) techniques of intrascleral pocket and conventional scleral flap with conjunctival division techniques in terms of short-term clinical effects.
Methods: This retrospective cohort study included all consecutive patients with aphakia in Gyeongsang Nation- al University Hospital in Jinju, Korea, who underwent TSF between January 2012 and December 2014. The medical records of all patients were retrospectively reviewed, and the endothelial cell count (ECC), refraction, best-corrected visual acuity (BCVA), intraocular pressure, slit lamp, and fundus examination results before and 1 day and 6 months after surgery were recorded. The postoperative complications and visual outcomes were also recorded.
Results: The intrascleral pocket and conventional-flap groups did not differ significantly in terms of demograph- ics, presurgical BCVA, or ECC. However, the intrascleral pocket group had a significantly lower BCVA at 1 day and 6 months after surgery compared to the conventional-flap group. The two groups did not differ in terms of ECC 6 months after surgery. The intrascleral pocket group had no postoperative complications, but five patients in the conventional-flap group complained of irritation. In both groups, the intraocular lens was well positioned without tilting or subluxation, and astigmatism was significantly reduced at 1 day and 6 months after surgery.
Conclusions: The intrascleral pocket technique of TSF does not involve conjunctival dissection and is a suc- cessful method of sulcus fixation. It stably corrects the intraocular lens and is easy to perform, which helps to reduce operation time. It also reliably yields rapid visual acuity recovery without complications.
Key Words: Aphakia, Intrascleral pocket technique, Transscleral fixation
Transscleral fixation (TSF) of posterior chamber intraoc- ular lenses (PCIOLs) allows implantation in the absence of sufficient capsular support. There are various methods for
secondary intraocular lens (IOL) TSF at the ciliary sulcus or pars plana [1-6]. TSF technique usually needs conjuncti- val dissections to create a scleral bed for the route of fixa- tion sutures and to conceal the knot [7-9]. However, knot exposure remains one of the most common complications of this procedure. To avoid this complication, scleral flaps that cover the knots are often used. Scleral tunnels or scler- al pockets are also sometimes used to avoid knot exposure [2,6,8]. However, these procedures still cannot completely
Received: March 24, 2015 Accepted: July 15, 2015
Corresponding Author: Seong-Jae Kim, MD, PhD. Department of Oph- thalmology, Gyeongsang National University Hospital, #79 Gangnam- ro, Jinju 52727, Korea. Tel: 82-55-750-8468, Fax: 82-55-758-4158, E-mail:
prevent knot exposure. Moreover, scleral flaps require con- siderable technical skills and thus are associated with pro- longed operation time. In addition, when there is adhesion of the sclera and conjunctiva or if there is a corneal wound at the flap site, it is difficult to generate the scleral flap.
To overcome these problems, the intrascleral pocket technique was introduced for TSF of IOL in previously vitrectomized eyes [10]. The present retrospective cohort study compared the intrascleral pocket and conventional scleral flap techniques with conjunctival division tech- niques in terms of short-term clinical results.
Materials and Methods
Patient selection and outcome variables
The institutional review board of Gyeongsang National University Hospital approved the study protocol (no. 2015- 06-031), and the protocol complied with the tenets of the Declaration of Helsinki. All consecutive patients in a ter- tiary referral hospital, Gyeongsang National University Hospital in Jinju, Korea, who underwent TSF for aphakia due to various causes, including IOL dislocation, retinal detachment, trauma, zonulysis, endophthalmitis, phaco- morphic, and acute angle closure glaucoma, between Janu- ary 2012 and December 2014 were identified by a review of the medical records. Before surgery and 1 day and 6 months after surgery all patients underwent examinations to measure refraction, best-corrected visual acuity (BCVA), intraocular pressure, and specular microscopy, as well as slit lamp and fundus examinations. The power of IOL was calculated using the Sanders-Retzlaff-Kraff II formula.
The postoperative complications were recorded.
Surgical techniques
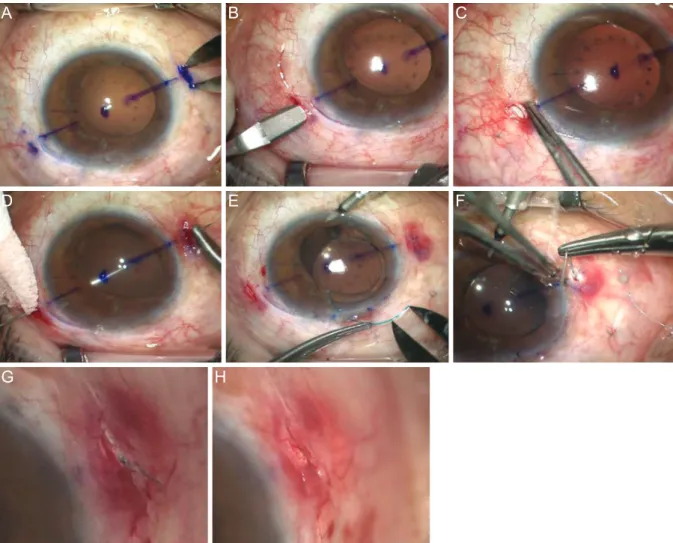
The intrascleral pocket technique for TSF was conducted by one surgeon (KSJ), and the surgical procedures were as follows: at the limbus, two points 180° from each other were marked (Fig. 1A). To make a 2-mm-sized pocket, lamellar dissection without conjunctival dissection was performed with a crescent blade, then the blade was ad- vanced about 1 to 1.5 mm (Fig. 1B and 1C). A straight nee- dle attached to 10-0 polypropylene was passed through the transconjunctival transcleral passage, which was located
1.5 mm posterior from the limbus. A prolene suture was then docked using a 26-gauge needle (Fig. 1D). Anterior to the limbus, a clear corneal incision (CCI) was made using a keratome, and the prolene sutures were exteriorized through the CCI pocket. An ophthalmic viscosurgical de- vice was inserted into the anterior chamber. A three-piece foldable acrylic IOL (SENSAR Soft Acrylic IOL; Abbott Medical Optics, Santa Ana, CA, USA) was injected through the CCI, and the prolene sutures for each haptic were tied (Fig. 1E). The IOL was placed in the anterior chamber, and its orientation was adjusted by pulling the prolene sutures. The IOL was centralized, and the ends of the prolene were sutured in the intrascleral pocket (Fig.
1F). To avoid exposure, knots were buried under the sclera flaps (Fig. 1G and 1H). The CCI and other paracentesis wounds were then hydrated, and the conjunctival edges were joined without suture.
The scleral flap with conjunctival division technique was as follows: after conjunctival dissection, a triangu- lar-shaped scleral flap was made, a 2.8-mm CCI was gen- erated at the anterior limbus using a keratome, and a three- piece foldable acrylic IOL was injected. The haptic ends were exteriorized through the CCI, after which each haptic was tied. After IOL centration, the scleral flap ends and conjunctiva were sutured.
Statistics
Continuous data were presented as mean ± standard de- viation, and categorical variables were presented as num- ber (%). The two surgical groups were compared in terms of BVCA, endothelial cell count (ECC), spherical equiva- lent, and astigmatism using the paired t-test. All statistical analyses were performed using IBM SPSS ver. 19.0 (IBM Co., Armonk, NY, USA). A p-value less than 0.05 was considered to indicate statistical significance.
Results
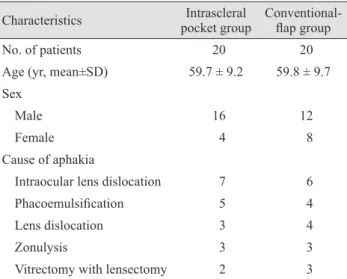
In total, 40 consecutive patients with aphakia underwent TSF in our hospital between January 2012 and December 2014. The mean age of the cohort was 59.8 ± 4.1 years, and there were 28 males and 12 females. The mean age of the intrascleral pocket and conventional-flap groups was 59.7 ± 9.2 and 59.8 ± 9.7 years, respectively. In both groups, the
110
main cause of aphakia was IOL dislocation. Other causes were phacoemulsification, lens dislocation, zonulysis, and vitrectomy with lensectomy, which occurred in the two groups with similar frequencies (Table 1). The two groups did not differ significantly in terms of preoperative BCVA and ECC or ECC at 6 months after surgery (Table 2). How- ever, the intrascleral pocket group had significantly better BCVA at 1 day and 6 months after surgery compared to the conventional-flap group (p = 0.03 and 0.04, respective- ly). The intrascleral pocket group did not experience any postoperative complications. In contrast, five of the 20 pa- tients in the conventional-flap group complained of irrita- tion after surgery (Table 2). One day and 6 months after surgery, the intrascleral pocket group exhibited significant
decrease in spherical diopter (p = 0.018 and 0.005 com- pared to preoperative values, respectively) and astigmatism (p = 0.027 and 0.028, respectively). This was also observed for the conventional-flap group for spherical diopter (p = 0.000 and 0.007, respectively) and astigmatism (p = 0.009 and 0.007, respectively) (Fig. 2A and 2B).
Discussion
TSF of an IOL is widely used for aphakic patients with poor support of the posterior chamber or ciliary body.
Many recent studies have reported modifications of the TSF technique that was first introduced by Malbran et al.
Fig. 1. Intrascleral pocket technique. (A,B) Two points were marked at 180° apart at the limbus. To create a 2-mm-sized pocket, lamellar dissection without conjunctival dissection was performed with a crescent blade. (C) The constructed pocket was visualized. (D) A 9-0 straight needle was passed through the transconjunctival transcleral passage. (E) A three-piece foldable acrylic intraocular lens was in- serted via clear corneal incision, and then each haptic end was exteriorized through clear corneal incision and tied with prolene suture. (F) The suture was placed in the intrascleral pocket with forceps opening one part of the pocket. (G,H) Each knot was buried under scleral flaps to prevent exposure, and the conjunctiva was joined without suture.
A
D
G
B
E
H
C
F
111 in 1986 [11-13]. However, all of these methods can cause
suture-related complications, including knot exposure or
IOL dislocation due to suture decomposition or breakage.
Of these complications, knot exposure is one of the most common and can have deleterious outcomes as it can act as a pathway for bacterial invasion into the eye, thereby causing endophthalmitis [14].
When Szurman et al. [12] retrospectively analyzed the results of 45 eyes that underwent TSF of PCIOL using Z-sutures and 22 eyes that underwent TSF of an iris pros- thesis, they found one case of ciliary body hemorrhage during the 22.4 months of follow-up, but no complications such as knot exposure, suture looseness, conjunctival atro- phy, or chronic inflammation. Ma et al. [5] also analyzed the clinical outcomes of a knotless external fixation tech- nique of PCIOL TSF in five patients who had to undergo this technique because of adhesion between the conjuncti- va and cornea or because the location of the conjunctival flap was near a corneal wound caused by trauma. There- fore, this study introduced the sutureless intrascleral pock- et technique and compared the effects and complications
Table 2. Clinical results of the two groups before and 1 day and 6 months after the operation
Characteristics Intrascleral pocket group Conventional-flap group p-value*
Preoperative BCVA† 0.23 ± 0.3 0.26 ± 0.4 0.152
Preoperative ECC 2,010 ± 53 2,045 ± 62 0.082
BCVA at 1 day postoperative† 0.45 ± 0.24 0.53 ± 0.42 0.030
BCVA at 6 months postoperative† 0.24 ± 0.31 0.35 ± 0.28 0.040
ECC at 6 months postoperative 2,013 ± 73 2,056 ± 51 0.237
Postoperative complications (type) 0 5 (irritation) -
BCVA = best-corrected visual acuity; ECC = endothelial cell count.
*Paired t-test comparing the two groups; †Logarithm of the minimum angle of resolution.
Table 1. Comparison of the two groups in terms of patient de- mographics and clinical features
Characteristics Intrascleral
pocket group Conventional- flap group
No. of patients 20 20
Age (yr, mean±SD) 59.7 ± 9.2 59.8 ± 9.7 Sex
Male 16 12
Female 4 8
Cause of aphakia
Intraocular lens dislocation 7 6
Phacoemulsification 5 4
Lens dislocation 3 4
Zonulysis 3 3
Vitrectomy with lensectomy 2 3
Fig. 2. The intrascleral pocket group and conventional-flap group demonstrated significant decrease in spherical diopter (A) and astigma- tism (B) at 1 day and 6 months after the operation. *Paired t-test.
Spherical equivalent (diopter)
Preoperative 1 day 6 mon
Intrascleral pocket group Conventional-flap group 7
6 5 4 3 2 1 0 -1 -2
-3 p = 0.018*
p = 0.005* p = 0.000*
p = 0.007*
Astigmatism (diopter) Preoperative
1 day 4
3 2 1
p = 0.007*
p = 0.009*
p = 0.027*
p = 0.028*
Spherical equivalent (diopter)
Preoperative 1 day 6 mon
Intrascleral pocket group Conventional-flap group 7
6 5 4 3 2 1 0 -1 -2
-3 p = 0.018*
p = 0.005* p = 0.000*
p = 0.007*
Astigmatism (diopter) Preoperative
1 day 6 mon Intrascleral pocket group Conventional-flap group 4
3 2 1 0
p = 0.007*
p = 0.009*
p = 0.027*
p = 0.028*
A B
112
including astigmatism or postoperative visual prognosis.
Compared with conventional techniques, this technique resulted in less irritation and astigmatism since knots were buried in the intrascleral pocket, and vertical and regular wounds were formed without a gap of wound. In addition, this technique led to rapid visual recovery and return to daily life, since the visual acuity the day after the opera- tion was comparable to the BCVA before the surgery.
During the follow-up period, there were no complications except for mild ciliary body hemorrhage in one case and IOL tilting immediately after the operation due to exces- sive knot tightness in another case. The BCVA in 16 of 20 cases (80%) improved, while the remaining case did not exhibit a change in BCVA. Thus, the outcomes of the in- trascleral pocket technique in the present study were gen- erally as successful as those of the knotless external fixa- tion technique of PCIOL in a previous study [6].
The intrascleral pocket technique of TSF is especially useful for patients who previously underwent vitrectomy.
Patients after vitrectomy, especially those who underwent surgery with a 20-gauge needle, usually have a relatively thin conjunctiva or conjunctiva-Tenon-scleral complex due to previous conjunctival dissection. This makes conjuncti- val dissection more difficult and increases the possibility of conjunctival defects and scleral injury. Thus, the intras- cleral pocket technique will be particularly useful for such patients. In addition, since this technique does not involve conjunctival dissection, the operation time and bleeding risk are reduced. Moreover, subsequent glaucoma surgery can improve the success rate of the intrascleral pocket technique because the conjunctiva and Tenon’s space maintain their native integrity [10]. The intrascleral pocket technique also allows for rapid visual acuity recovery and return to daily life because the associated irritation is low.
In addition, the vertical and regular wound without a gap helps to reduce astigmatism. In a previous study using the sutureless intrascleral pocket technique [10], there was no specific finding from photographs 1 day after the surgery.
This prompted us to reassess patients at 6 months after the surgery in this study, and the wounds were found to be clean without dehiscence or knot exposure (Fig. 3A and 3B).
Unlike the reverse pocket technique, the intrascleral pocket technique leaves the corneal limbus intact, which reduces the chance of injury to the corneal nerve. More- over, it is possible to perform the intrascleral pocket tech-
nique with topical anesthesia because it is associated with less pain than other techniques. In addition, the intrascleral pocket technique is quite similar to glaucoma or flap-mak- ing procedures, which means that surgeons can rapidly be- come proficient in this technique. There is also no possibil- ity of angle injury or anterior chamber puncture [10].
In conclusion, the present study showed that the intras- cleral pocket technique of TSF had better clinical results than the conventional scleral flap with conjunctival divi- sion technique, as determined by ophthalmological exam- inations before and 1 day and 6 months after the operation.
The improvement in BCVA was more marked in the in- trascleral pocket group, and no postoperative complica- tions were observed. These observations, together with the fact that this technique is relatively easy, suggest that this technique is a good method of TSF.
This study has some limitations. First, the sample size was small. Second, the patients were only followed up for 6 months. Further studies with longer-term clinical fol- low-up are required. However, the simplicity and good outcomes of this technique suggest that it is a good method of TSF.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This research was supported by Basic Science Research Program through the National Research Foundation of Ko- Fig. 3. (A) Anterior segment photography and (B) anterior optical coherence tomography 6 months after the surgery showed a clean wound without dehiscence or knot exposure.
A B
rea (NRF) funded by the Ministry of Science, ICT & Fu- ture Planning (NRF-2015R1C1A1A02037702).
References
1. Wagoner MD, Cox TA, Ariyasu RG, et al. Intraocular lens implantation in the absence of capsular support: a report by the American Academy of Ophthalmology. Ophthalmolo- gy 2003;110:840-59.
2. Lewis JS. Ab externo sulcus fixation. Ophthalmic Surg 1991;22:692-5.
3. Teichmann KD. Pars plana fixation of posterior chamber intraocular lenses. Ophthalmic Surg 1994;25:549-53.
4. Kim DH, Heo JW, Hwang SW, et al. Modified transscleral fixation using combined temporary haptic externalization and injector intraocular lens implantation. J Cataract Re- fract Surg 2010;36:707-11.
5. Ma DJ, Kim MK, Wee WR. Knotless external fixation technique for posterior chamber intraocular lens transscler- al fixation: a 5-case analysis. J Korean Ophthalmol Soc 2012;53:1609-14.
6. Lin CP, Tseng HY. Suture fixation technique for posterior chamber intraocular lenses. J Cataract Refract Surg 2004;
30:1401-4.
7. Solomon K, Gussler JR, Gussler C, Van Meter WS. Inci-
dence and management of complications of transsclerally sutured posterior chamber lenses. J Cataract Refract Surg 1993;19:488-93.
8. Lewis JS. Sulcus fixation without flaps. Ophthalmology 1993;100:1346-50.
9. Kir E, Kocaturk T, Dayanir V, et al. Prevention of suture exposure in transscleral intraocular lens fixation: an origi- nal technique. Can J Ophthalmol 2008;43:707-11.
10. Cho YW, Chung IY, Yoo JM, Kim SJ. Sutureless intras- cleral pocket technique of transscleral fixation of intraocu- lar lens in previous vitrectomized eyes. Korean J Ophthal- mol 2014;28:181-5.
11. Malbran ES, Malbran E Jr, Negri I. Lens guide suture for transport and fixation in secondary IOL implantation after intracapsular extraction. Int Ophthalmol 1986;9:151-60.
12. Szurman P, Petermeier K, Aisenbrey S, et al. Z-suture: a new knotless technique for transscleral suture fixation of intraocular implants. Br J Ophthalmol 2010;94:167-9.
13. Stewart MW, Landers MB 3rd. Transscleral intraocular lens fixation with a “homemade” needle and hook. J Cata- ract Refract Surg 2006;32:200-2.
14. Heilskov T, Joondeph BC, Olsen KR, Blankenship GW.
Late endophthalmitis after transscleral fixation of a poste- rior chamber intraocular lens. Arch Ophthalmol 1989;
107:1427.