Vol. 11, No. 4, December, 2004
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
<접수일:2004년 7월 2일, 심사통과일:2004년 11월 17일>
※통신저자:박 태 수
경기도 구리시 교문동 249-1
한양대학교 의과대학 구리병원 정형외과학교실
Tel:031) 560-2314, Fax:031) 557-8781, E-mail:[email protected]
류마티스 질환 환자와 비류마티스 환자에 있어 요추부 후측방 유합술의 결과 비교
-류마티스 질환 환자에서의 척추 유합술-
한양대학교 의과대학 구리병원 정형외과학교실, 한양대학교 의과대학 정형외과학교실*
박예수․황규태․박태수․최충혁*․성일훈*․조재림*
= Abstract =
Comparative Analysis between Rheumatic and Non-rheumatic Disease Patients after Posterolateral Fusion of the Lumbar Spine
-Spinal Fusion in Rheumatic Disease Patients-
Ye-Soo Park, M.D., Kyu-Tae Hwang, M.D., Tae-Soo Park, M.D., Cheong-Hyeok Choi, M.D.*, Il-Hoon Sung, M.D.*, Jae-Lim Cho, M.D.*
Department of Orthopaedic Surgery, Kuri Hospital Hanyang University College of Medicine Department of Orthopaedic Surgery, Hanyang University College of Medicine*
Objective: To evaluate the clinical and radiological results and to compare the results of posterolateral lumbar fusion in rheumatic and non-rheumatic disease.
Methods: A retrospective review of results was carried out in 20 patients who had posterolateral lumbar fusion with rheumatic disease from Jul. 1996 to Aug. 2002. And same cases of non-rheumatic disease were compared. The diagnosis of rheumatic disease was confirmed by the ARA revised criteria. Bony union was evaluated by Lenke's criteria and the clinical results by Katz's satisfaction degree. Statistical analysis was performed by paired T-test and ANOVA test.
Results: In rheumatic disease group, there were 7 males and 13 females. Mean age was
서 론
류마티스 질환자의 경우 경추부 이환에 대해서는 많은 보고가 있으며1-5), 이러한 경추부 이환 시에는 동통이나 신경근병증으로 인한 증상으로 일상 생활 에 지장을 받는 경우가 많다. 그러나 상대적으로 요 추부의 이환율은 적으며 남자의 경우 5%, 여자의 경우 3% 정도로 요추부 이환율이 보고되어 있다6). 이처럼 낮은 이환율을 보이는 요추부의 경우 병변 자체와 류마티스 질환과의 연관성을 확인하기가 쉽 지 않으며 요추부 질환에 동반된 류마티스 환자들에 있어서의 수술적 치료 결과의 분석 또한 많지 않은 실정이다.
또한 류마티스 질환 환자의 경우 과도한 스테로이 드의 사용 등으로 인해 수술적 치료 시 골질이 불량 하고, 술 후 상처 치유가 지연되며 감염률이 높은 것으로 알려져 있으며 술 전 투여한 소염 진통제의 사용으로 인한 술 후 혈소판 응집 현상의 방해로 출 혈이 비 류마티스 질환 환자에 비해 높은 것으로 보 고되어 있다7-9).
이에 본 저자들은 요추부 질환의 수술적 치료에 있어 가장 보편적으로 많이 시행되고 있는 후측방 유합술을 통해 류마티스 질환 환자와 비류마티스 질 환 환자를 대상으로 유합술 시행 후 추시 결과를 임
상적, 방사선학적으로 분석하고, 두 군 간의 결과를 비교해 보고자 하였다.
대상 및 방법
1996년 7월부터 2002년 8월까지 류마티스 질환 환 자 중 요추부 후측방 유합술을 시행한 환자 20예를 대상으로 하여 추시 관찰하였으며, 같은 시기에 후 측방 유합술을 시행한 동일한 수의 류마티스 질환이 없는 환자군을 무작위로 선별하여 결과를 비교 분석 하였다. 류마티스 질환의 감별은 ARA revised cri- 56.6 (20∼68) years and mean fused segments were 2.7 (1∼7). Mean follow-up period was 41 months (12∼80) after surgery. In non-rheumatic group, there was 6 males and 14 females. Mean age was 57.1 (35∼71) years and mean fusion segments were 2.9 (1∼4), Mean follow-up period was 40.2 (12∼88) months. In age and fusion segments between two group, there was no statistical difference. In rheumatic disease group, the diagnosis were rheumatoid arthritis in 18 patients, ankylosing spondylitis in 1, and systemic lupus erythematosus in 1 patient. The other operations for combined disease were 8 total knee arthroplasty and 3 total hip arthroplasty. There were no statistical differences in operation time (p=0.527), perioperative bleeding (p=0.653) and postoperative (p=0.830) bleeding between two group. In radiological bony union, all patients of two groups showed A and B grade by Lenke's criteria. Bony union was complete at 5.5 (5∼8), 5.1 (4∼7) months after surgery. There was no significant difference in clinical satisfaction (p=0.756).
Conclusion: There were no significant differences in clinical and radiological results between the rheumatic and non-rheumatic patients with disease of the lumbar spine.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: Rheumatic disease, Spine, Posterolateral fusion
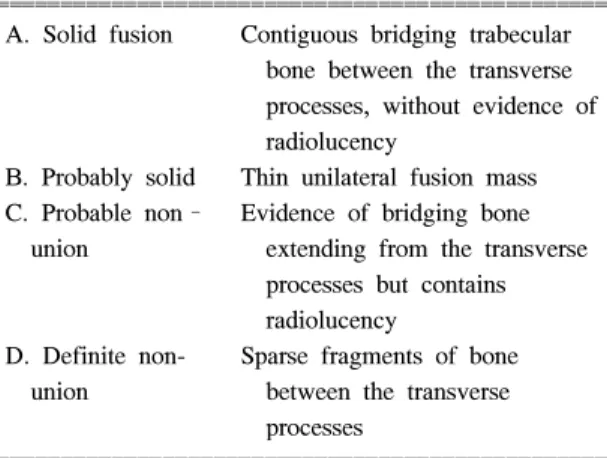
Table 1. Lenke’s classification
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
A. Solid fusion Contiguous bridging trabecular bone between the transverse processes, without evidence of radiolucency
B. Probably solid Thin unilateral fusion mass C. Probable non– Evidence of bridging bone union extending from the transverse
processes but contains radiolucency
D. Definite non- Sparse fragments of bone union between the transverse
processes
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
teria를 이용하였으며, 방사선학적으로는 골유합의 확 인을 위해 Lenke 등10)의 판정 기준(Table 1)을 이용 하여 평가하였으며, 임상적으로는 매우 만족(1), 만 족(2), 불만족(3), 매우 불만족(4)으로 분류한 Katz 등
11)의 기준을 이용하여 환자의 주관적 만족도를 측정 하였다. 또한 둔부, 대퇴부, 하퇴부에 대한 동통의 정도를 평가하였으며 보행 능력에 대해서는 일상 생 활의 활동 범위가 어느 정도까지 가능한지를 전화 설문과 직접 내원의 방법을 통하여 조사하였다.
두 군 간의 결과는 SPSS for windows 11.0을 이용 하여 paired sample T-test와 ANOVA를 통하여 분석 하였다.
결 과
류마티스 질환군의 경우 남자 7예, 여자 13예이었 으며, 평균 연령은 56.6세(20∼68), 평균 유합 분절은 2.7분절(1∼7), 평균 추시 기간은 41개월(12∼80)이었 다. 류마티스 질환이 없는 환자군에서는 남자 6예, 여 자 14예이었으며, 평균 연령은 57.1세(35∼71), 평균 유합 분절은 2.9분절(1∼4), 평균 추시 기간은 40.2개 월(12∼88)이었다. 두 군 간 연령(p=0.853), 유합 분 절(p=0.059)에 있어서 유의한 차이가 없는 것으로 나 타났다. 류마티스 질환군의 경우 18예가 류마티스 관절염이었으며, 강직성 척추염 1예, 전신성 홍반성 루프스가 1예이었다. 또한 동반된 질환으로 시행한 수술은 슬관절 치환술 8예, 고관절 치환술 3예이었 다. 후측방 유합술을 시행하게 된 대상 질환으로는 류마티스 질환군의 경우 척추관 협착증이 16예, 척 추 전방 전위증이 3예, 추간판 탈출증이 1예 이었으 며 비류마티스 질환군의 경우 척추관 협착증이 17 예, 척추 전방 전위증이 2예, 추간판 탈출증이 1예이 었다. 각 군의 수술 시 소요된 시간은 233.7분(135∼
395), 225.7분(145∼390)으로 두 군 간에 유의한 차이 는 없었다(p=0.527). 수술 중 출혈량은 1732.5 mL (550∼3,000), 1825 mL (800∼4,500)이었으며, 술 후 출혈량은 909.5 mL (120∼2210), 939.5 mL (290∼
1950)이었다. 각 군에 있어서 술 중 출혈량(p=0.653) 과 술 후 출혈량(p=0.830)에서 유의한 차이는 없었다.
1. 방사선학적 평가
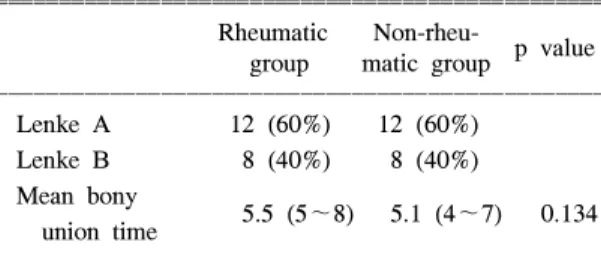
방사선 소견상 골 유합은 두 군 모두 전례의 환자 에서 Lenke A, B 등급을 보여 주었으며, 류마티스 환자의 경우 Lenke A, B 등급이 각각 12예, 8예였으 며 비류마티스 환자군의 경우도 각각 12예, 8예에서 Lenke A, B 등급을 보여주었다(Table 2). 가관절증은 두 군 모두에서 보이지 않았다. 각 군의 평균 골유 합까지의 기간은 각각 5.5개월(5∼8)과 5.1개월(4∼7) 로 유의한 차이를 보이지 않았다(p=0.134).
2. 임상적 평가
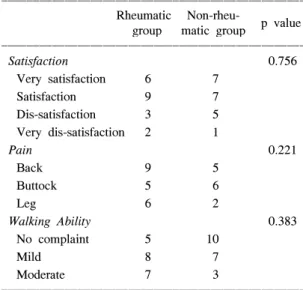
임상적 결과는 Katz 등11)의 주관적 만족도에 대한 평가 분류법을 이용하여 만족도, 동통, 보행 능력, 재수술 여부를 평가하였다. 류마티스 질환 환자의 평균 만족 등급 2.05점(1∼4점)이었으며, 15예(75%) 에서 ‘만족’ 이상의 결과를 보여 주었다. 비류마티스 질환 환자의 경우 평균 만족 등급 2점(1∼4점)으로 14예(70%)에서 ‘만족’ 이상의 결과를 보여 유의한 차이를 보이지 않았다(p=0.756). 술 후 동통에 대한 평가는 각각 요추부와 둔부, 하퇴부에 대해 조사하 였으며 류마티스 환자의 경우 요추부 동통을 호소한 환자 중 경도의 동통이 6예, 중등도의 동통이 3예 있었다. 둔부에 대한 동통은 경도의 동통이 3예, 중 등도 동통이 2예 있었으며 하퇴부에 경도의 동통을 호소한 경우가 4예, 중등도의 동통을 호소한 경우가 2예 있었다. 비류마티스 환자의 경우 요추부 동통을 호소한 환자 중 경도의 동통이 4예, 중등도의 동통 이 1예 있었다. 둔부에 대한 동통은 경도의 동통이 5예, 중등도 동통이 1예 있었으며 하퇴부에 경도의 동통을 호소한 경우가 2예 있었다. 각 부위별 동통 의 비교 결과 요추부(p=0.069), 둔부(p=0.545), 하퇴부
Table 2. Radiologic evaluation
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Rheumatic Non-rheu-
p value group matic group
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Lenke A 12 (60%) 12 (60%)
Lenke B 8 (40%) 8 (40%) Mean bony
5.5 (5∼8) 5.1 (4∼7) 0.134 union time
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
(p=0.049)로 요추부와 둔부의 동통에 대해서는 유의 한 차이를 보이지 않았으나 하퇴부의 동통에 대해서 는 유의한 차이를 보였다.
보행 능력의 평가는 집안에서의 일상 생활의 범위 와 외출 시 보행 거리와 동통의 발생과의 상관 관계 에 대해 전화 설문과 직접 내원의 방법으로 시행하 였다. 류마티스 환자의 경우 5예에서 생활의 불편을 호소하지 않았으며 8예에서 외출 시 경도의 동통을 호소하였다. 7예에서는 외출 시 중등도의 동통을 호 소하였으나 이들은 수술 전 외출을 할 수 없었던 경 우의 환자였다. 비류마티스 환자의 경우 10예에서 생활의 불편함을 호소하지 않았으며 7예에서 집 밖 으로 외출 시 경도의 동통을 호소하였다. 3예에서 중등도의 동통이 외출 시 동반된다고 호소하였다.
보행 능력에 있어서 두 군 간 비교 역시 유의한 차 이를 보이지 않았다(p=0.383)(Table 3).
고 찰
류마티스 질환 환자들의 경우 사지의 관절에 대한 증상과 경추부 이환에 의한 신경학적 증상을 동반하 는 경우가 많아 이에 대한 보고는 많지만 상대적으 로 적은 이환율을 보이는 요추부에 대해서는 보고가 많지 않다12-17). 그러나 일부에서는 류마티스 질환 환
자의 경우 요추부의 이환에 대한 방사선학적 검사 결과 57% 정도의 환자에서 요추부 이환을 보고하고 있으며 이 중 경추부의 이환과 동반된 경우는 42%
에 이른다는 보고도 있다18). 또한 Yoshiharu 등19)의 연구 결과에 따르면 류마티스 환자 중 요추부 동통 을 호소하는 경우가 40% 정도 있다고 보고하고 있 다. 그러나 저자들의 경우에서는 요추부 질환으로 수술을 시행한 류마티스 질환 환자의 경우 요추부에 서 발생한 병변이 류마티스 질환에 의한 것이라는 확진은 할 수 없었다.
이러한 류마티스 질환의 경우 질병의 치료를 위한 과도한 스테로이드의 사용, 장기간의 소염 진통제의 사용 등으로 인해 수술적 치료 시 그 결과가 좋지 않으며 부작용의 발생 빈도 또한 높은 것으로 알려 져 있다7,9). 특히 혈소판 수치가 감소되고 이로 인해 출혈량이 많을 것으로 예측되었으나 본 연구의 결 과, 술 중 출혈량(p=0.653)과 수술 시간(p=0.527)에서 유의한 차이는 없는 것으로 나타났다. 또한, 술 후 출혈량에 있어서도 두 군 간에 유의한 차이는 보이 지 않았다(p=0.830).
이들 모두는 척추 수술을 시행 받기 전 평균 6.9 년의 기간 동안 소염 진통제 및 스테로이드의 장기 복용을 하고 있는 상태였으나 이로 인한 절개 부위 의 염증이나 치유 지연 소견은 보이지 않았다.
이러한 결과는 저자들의 경우 류마티스 환자군의 수술 시 수술 2주 전 메토트렉세이트(methotrexate) 의 복용을 중지시켰으며 진통 소염제의 경우 환자의 통증 양상을 보아 가능하면 수술 1주 전 복용을 중 지시켜 약물에 의한 술 후 위험성을 감소시킨 결과 로 판단되며 또한 요추부의 경우 타 수술 부위에 비 해 혈액 순환이 풍부한 근육이 많아 상대적으로 혈 액 순환이 좋은 점이 한 요인으로 작용하였다고 판 단되는 바이다.
또한 다량의 스테로이드 등의 사용으로 발생 가능 한 합병증으로는 골다공증을 들 수 있으며 저자들은 이로 인해 술 후 골 유합의 정도에서 차이를 보일 것으로 생각하였으나, 두 군 모두 Lenke A, B 등급 의 양호한 골 유합 소견을 보여 두 군 간에 유의한 차이를 볼 수 없었다. 특히 평균 골 유합 기간에서 도 각각 5.5 (5∼8)개월과 5.1 (4∼7)개월로 유의한 차이가 없는 것으로 나타났다(p=0.134)(Fig. 1, 2).
Table 3. Clinical evaluation
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Rheumatic Non-rheu-
p value group matic group
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Satisfaction 0.756
Very satisfaction 6 7
Satisfaction 9 7
Dis-satisfaction 3 5 Very dis-satisfaction 2 1
Pain 0.221
Back 9 5
Buttock 5 6
Leg 6 2
Walking Ability 0.383
No complaint 5 10
Mild 8 7
Moderate 7 3
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
이는 저자들이 술 후 환자의 통증 조절을 위해 소 염 진통제를 사용하지 않은 점과 충분한 자가골을 이식한 결과라 생각되어 진다. 또한 골밀도 검사 후 T score가 -2.5점 이하인 경우 골 형성을 위해 사용 한 골다공증 치료제의 영향도 고려할 수 있겠다.
술 후 환자의 주관적 만족도는 두 군에서 각각 평 균 2.05점, 2.0점으로 나타났으며 75%와 70%의 환자 에서 ‘만족’ 이상의 결과를 보여주었다. 이 결과 역 시 유의한 차이를 보이지 않았다(p=0.756). 하지만 류마티스 환자군에서 술 후 보행 시 비류마티스 환 자군보다 다소 많은 수의 환자에서 동통을 호소하였
으며 특히 하퇴부 동통에 대해서는 의미가 있는 차 이를 보였다. 이는 류마티스 질환이 전신적 질환으 로 하지의 다른 관절을 이환하여 발생되었던 결과라 저자들은 판단하였다.
결 론
결론적으로 요추부 질환이 동반된 류마티스 환자 군의 후측방 유합술 치료에 있어서 임상적, 방사선 학적 결과를 비교 분석한 결과 류마티스 질환이 없 는 군과 비교하여도 양호한 결과를 얻을 수 있었다.
Fig. 1. Preoperative anteriorposte- rior (A) and lateral rent- genograms (B) of 62-year- old man who had me- dicated with immunosup- pressants and NSAIDs for rheumatoid arthritis. Posto- perative anteriorposterior (C) and lateral rentgenograms (D) showing solid fusion mass at both sides.
A B
C D
그러나 류마티스 질환에 의해 직접적으로 유발된 요 추 질환의 치료 결과를 추가적으로 연구하여 비교한 다면 보다 정확한 결과를 보여줄 수 있다고 사료되 는 바이다.
REFERENCES
1) Boden SD, Dodge LD, Bohlman HH, Rechtine GR.
Rheumatoid arthritis of the cervical spine: a long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg 1993;75A:1282-97.
2) Gorden DA, Hastings D. Rheumatoid arthritis: clinical features of early, progressive and late disease. In:
Klippel JH, Dieppe PA, eds. Rheumatology. p. 1-14, London, Mosby, 1998.
3) Linquist PR, McDonnell DE. Rheumatoid cyst causing extradural compression: a case report. J Bone Joint Surg Am 1970;52:1235-40.
4) Paimela L, Laasonnen L, Kankaanpaa E, Leirisalo- Repo M. Progression of cervical spine changes in patients with early rheumatoid arthritis. J Rheumatol 1997;24:1280-4.
5) Yonezawa T, Tsuji H, Matsui H, Hirano N. Subaxial Fig. 2. Preoperative anteriorposte-
rior (A) and lateral rentge- nograms (B) of 55-year- old woman who was diag- nosed as spondylolisthesis and degenerative spinal ste- nosis. Postoperative anteri- orposterior (C) and lateral rentgenograms (D) show- ing solid fusion mass at both sides.
A B
D
C
lesions in rheumatoid arthritis: radiological factors suggestive of lower cervical myelopathy. Spine 1995;
20:208-15.
6) Lawrence JS, Sharp J, Ball J, Bier F. Rheumatoid arthritis of the lumbar spine. Ann Rheum Dis 1964;
23:205-17.
7) Beyer CA, Hanssens AD, Lewallen DG, Pittelkow MR. Primary total knee arthroplasty in patients with psoriasis. J Bone Joint Surg Br 1991;73:258-9.
8) Robinson CM, Christie J, Malcolm-smith N. Non- steroidal anti-inflammatory drugs, perioperative blood loss and transfusion requirements in elective hip arthroplasty. J Arthro 1993;8:607-10.
9) Stern SH, Insall JN, Windsor RE, Inglis AE, Dines DM. Total knee arthroplasty in patients with psoriasis.
Clin Orthop 1989;248:108.
10) Lenke LG, Bridwell KH, Bullis D, Betz RB, Baldus C, Achoenecker PL. Results of in situ fusion for isthmic spondylolisthesis. J Spinal Disord 1992;5:
433-42.
11) Katz JN, Lipson SJ, Chang LC, Levine SA, Fossel AH, Liang MH. Seven-to 10 year outcome of decom- pressive surgery for degenerative lumbar spinal steno- sis. Spine 1996;21:92-8.
12) Ball J. Enthesopathy of rheumatoid and ankylosing spondylitis. Ann Rheum Dis 1971;30:213-23.
13) Biasi D, Caramaschi P, Carletto A, Pacor ML, Bam- bara LM. A case of rheumatoid arthritis with lumbar spine involvement. Rheumtol Int 1995;15:125-6.
14) Helliwell PS, Zebouni LN, Porter G, Wright V. A clinical and radiological study of back pain in rheu- matoid arthritis. Br J Rheumatol 1993;32:216-21.
15) Heywood AW, Meyers OL. Rheumatoid arthritis of the thoracic and lumbar spine. J Bone Joint Surg Br 1986;68:362-8.
16) Kuwahara S, Kimura C, Tajima N, Aso K, Sugano T. Radiological findings of the lumbar spine in rheumatoid arthritis. Jpn J Rheumatol 1989;2:13-24.
17) Shichikawa K, Matsui K, Oze K, Ota H. Rheumatoid spondylitis. Int Orthop 1978;2:53-60.
18) Sims WH, Jayson MI, Baddeley H. Rheumatoid in- volvement of the lumbar spine. Ann Rheum Dis 1977;36:524-31.
19) Yoshiharu K, Hiroaki M, Masahiko K, Hirokazu I, Kazuo O, Tomoatsu K. Radiologic findings of the lumbar spine in patients with rheumatoid arthritis and a review of pathologic mechanisms. J Spinal Disor- ders & Tech 2003;16:38-43.