tism classification criteria for rheumatoid arthritis (ACR/EULAR criteria)가 발표되었다[1]. 이 분류 체계는 류마티스인자(rheuma- toid factor)와 anti-citrullinated peptide/protein antibody (ACPA) 검사를 통해 환자의 혈청학적 특성을 평가하도록 하였으며 그 정 량적 결과에 따라 각기 다른 점수를 부여하여 진단에 도움이 되도 록 하고 있다.
ACPA의 검출을 위해 여러 검사 방법이 시도되었으나 오늘날 대 부분의 검사실에서는 anti-cyclic citrullinated peptide antibody (anti-CCP) 검사를 류마티스관절염의 진단에 활용하고 있다. 반면 ACPA 검사의 시초라고 할 수 있는 항핵주변인자(antiperinuclear factor) 검사는 류마티스관절염에 대한 높은 진단 특이도를 가지고 있음에도 불구하고[2-4] 검사 표준화 및 기질 확보의 문제로 인하 여 널리 사용되지는 않았다. 그러나 국내에서 상품화 된 항핵주변 인자검사 키트(IT-APF)[5]가 개발되면서 일반검사실에서도 항핵주 변인자를 검사할 수 있는 길이 열렸다.
서 론
지난 2010년도에 류마티스관절염의 새로운 분류 체계인 Ameri- can College of Rheumatology/European League against Rheuma-
2010 ACR/EULAR 류마티스관절염의 분류 체계에 대한 항핵주변인자 검사의 적용에 관한 예비 연구
A Preliminary Study for Applying Antiperinuclear Antibody Test to 2010 ACR/EULAR Classification Criteria for Rheumatoid Arthritis
최종문1·김신규2
Jong-Moon Choi, M.D.1, Think-You Kim, M.D.1,2
한양대학교의료원 진단검사의학과1, 조기 관절염과2
Departments of Laboratory Medicine1, Early Arthritis2, Hanyang University Medical Center, Seoul, Korea http://dx.doi.org/10.3343/lmo.2013.3.1.29
Corresponding author: Think-You Kim, M.D.
Department of Early Arthritis and Laboratory Medicine, Hanyang University Medical Center, 222 Wangsimri-ro, Seongdong-gu, Seoul 133-792, Korea Tel: +82-2-2290-8975, Fax: +82-2-2298-1735, E-mail: [email protected] Received: September 27, 2012
Revision received: October 8, 2012 Accepted: October 8, 2012
This article is available from http://www.labmedonline.org 2013, Laboratory Medicine Online
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: The American College of Rheumatology/European League against Rheumatism classification criteria for rheumatoid arthritis (ACR/EULAR criteria) include the rheumatoid factor (RF) test and the anti-citrullinated peptide/protein antibody (ACPA) test as serologic makers for rheumatoid arthritis. Antiperinuclear factor (APF) test, an originator of ACPA, is highly specific for rheumatoid arthritis and can be detected in RF or anti-cyclic citrullinated peptide (anti-CCP) negative rheumatoid arthritis, but it is not included in the serologic criterion of ACR/EULAR criteria.
In this study, we investigated the way for applying the APF test to ACR/EULAR criteria.
Methods: We analyzed clinical symptoms and laboratory findings of 53 patients who were suspected having rheumatoid arthritis. All patients were negative for the RF and anti-CCP and positive for APF. We classified these patients into 4 groups according to the fluorescence intensity of APF test, and gave 1-4 points for APF positivity. The proportion of patients who scored 6 or greater in ACR/EULAR criteria in relation to APF scores was evaluated.
Results: Median scores of ACR/EULAR criteria showed a tendency to increase as the level of fluorescence intensity of APF rises, but ACR/EULAR scores of 4 groups were not different significantly from each other ( P
>0.05). The proportion of patients who scored 6 or greater in ACR/EULAR criteria were 39.6% and 77.4%, when scores of APF positivity were 2 and 3 points, respectively.
Conclusions: We think it is reasonable to include APF test in the ACPA of ACR/EULAR criteria and give 3 points for APF positivity, regardless of its fluorescence intensity.
Key Words: Antiperinuclear factor, Rheumatoid arthritis, 2010 ACR/EULAR criteria
항핵주변인자검사는 류마티스관절염의 관절 손상을 조기에 예 측할 수 있는 지표 중 하나로서[6] 저자들은 대규모 연구를 통해 항핵주변인자 검사가 anti-CCP 및 류마티스인자 음성인 류마티스 관절염의 진단에 보완적 역할을 수행할 수 있음을 밝힌 바 있다[7, 8]. 하지만 항핵주변인자의 진단적 가치에도 불구하고 이를 ACR/
EULAR criteria에 적용하여 류마티스 관절염을 진단할 수 있는 지 침은 아직 없는 실정이다.
이에 저자들은 류마티스관절염 의심 환자를 대상으로 시행한 항핵주변인자검사, anti-CCP 검사 및 류마티스인자 검사 결과를 평 가하여 항핵주변인자의 ACR/EULAR criteria에 대한 적용 방안에 대해 연구하고자 본 연구를 시행하였다.
대상 및 방법
1. 대상
류마티스관절염이 의심되어 본원에 내원한 환자 중 항핵주변인 자 검사 양성, anti-CCP 및 류마티스인자 음성인 환자 53명을 대상 으로 임상증상 및 검사 결과를 평가하였다. 환자들은 남성 11명, 여성 42명, 평균 연령은 53.9세였으며 질환의 이환 기간은 모두 6개 월 이상이었다. ACR/EULAR criteria상 점수가 6점 이상인 류마티 스관절염 환자 및 전신성홍반성루프스, 섬유근육통 등 다른 류마 티스 질환으로 관절 부위의 통증이 발생한 환자는 본 연구에서 제 외되었다 .
2. 검사 방법
환자 선별 시 사용한 anti-CCP 검사와 류마티스인자 검사는 각 각 2세대 ELISA 검사 키트(ImmuLisa CCP ELISA, Immco Diagnos- tics, Buffalo, USA)와 nephelometry (BN II nephelometer, Simens Healthcare Diagnostics Inc., Newark, USA) 검사장비를 이용해 시 행하였으며 음성 기준은 제조사의 권고에 따라 각각 25 U/mL 및 15 IU/mL 이하인 경우로 하였다.
항핵주변인자 검사는 환자의 혈청을 1:20으로 희석하여 상품화 된 검사 키트(IT-APF, ImmunoThink Co., Seoul, Republic of Korea) 를 이용해 간접면역형광법으로 시행하였으며 형광현미경(Nikon Eclipse E80i, Nikon, Tokyo, Japan)으로 관찰했을 때 핵 주변부에 위치하는 원형 입자가 관찰되는 경우 그 형광 강도에 따라 아래와 같이 1+에서 4+까지 구분하여 보고하였다.
4+: Maximal fluorescence, brilliant yellow-green 3+: Less brilliant yellow-green fluorescence 2+: Less brilliant, but definite fluorescence 1+: Very subdued fluorescence
3. ACR/EULAR criteria 점수 평가 및 항핵주변인자 검사의 점수 체계 설정
대상 환자의 임상증상 및 검사 결과를 조사하고 이를 통해 ACR/
EULAR criteria의 점수를 계산하였다. 통증 및 부종이 있는 관절의 수와 종류 및 위치를 조사하고 ACR/EULAR criteria에서 제시하는 기준 [1]에 따라 관절의 종류를 대관절(large joint)과 소관절(small joint)로 분류하였으며 0에서 5점까지 점수를 측정하였다. 적혈구 침강속도(erythrocyte sedimentation rate, ESR), C 반응성단백(C- reactive protein, CRP) 검사를 통해 급성기반응물질에 대한 점수 를 평가하였으며 두 검사 중 하나 이상 양성인 경우 1점, 둘 다 음성 인 경우 0점을 부여하였다. 질병의 이환 기간에 따른 점수는 본 연 구에서 조사한 환자 모두 질병 이환 기간이 6주 이상이었으므로 전부 1점을 부여하였다. 이를 관절 이환 정도를 평가한 점수 및 급 성기반응물질 검사의 점수를 합산하여 혈청학적 검사를 제외한 ACR/EULAR criteria의 전체 점수를 평가하였다.
항핵주변인자 검사의 형광 강도(1+, 2+, 3+, 4+)에 따라 환자를 4 개의 그룹으로 분류하고 ACR/EULAR criteria의 점수를 평가한 후 그룹 간에 점수 부여 방식에 따라 총점이 6점 이상이 되는 환자의 비율 양상이 어떻게 변하는지 조사하였다.
4. 통계 분석
항핵주변인자 검사 결과에 따른 이환된 관절의 수, 급성반응기 물질 검사, ACR/EULAR criteria 점수를 비교하기 위하여 Kruskal- Wallis 검정을 시행하였다. 통계 분석 도구로는 SPSS 12.0 (SPSS Inc., Chicago, IL, USA)를 이용하였으며, 통계적 유의수준은 P
<0.05로 하였다.
결 과
1. 항핵주변인자 검사 결과 및 환자의 임상적 특성 비교
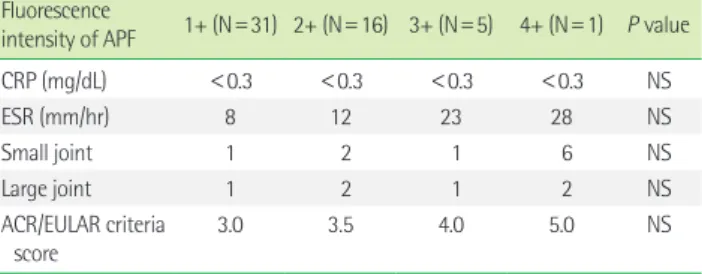
조사 대상이 된 53명의 환자 중 31명이 항핵주변인자 검사상 1+, 16명이 2+, 5명이 3+, 1명이 4+였다. ESR 및 전체 ACR/EULAR crite- ria 점수의 중앙값(median)을 비교했을 때 항핵주변인자 검사의 형광 염색 강도에 따라 그 수치가 증가하는 양상을 보였으나 통계 적으로 유의한 차이는 없었다(Table 1).
2. 항핵주변인자 검사의 점수 부여에 따른 ACR/EULAR criteria 점수 변화 비교
53명 전체의 APF 결과와 이에 따른 ACR/EULAR criteria 점수의 분포 및 APF에 점수를 부여할 경우 점수 변화 양상은 다음과 같았 다(Tables 2, 3).
형광 염색 강도와 상관없이 양성일 때 1점을 부여한 경우 전체
13.2%, 2점 부여 시 39.6%, 3점 부여 시 77.4%, 4점 부여 시 98.1%
의 환자가 6점 이상의 ACR/EULAR criteria 점수를 받을 수 있었다.
항핵주변인자 검사의 형광 강도가 1+인 경우와, 2+, 3+, 4+인 경 우에 각각 1점과 2점을 부여했을 때는 28.3%, 2점과 3점을 부여했
을 때 49.1%, 3점과 4점을 부여했을 때에 86.8%의 환자가 ACR/
EULAR criteria에서 6점 이상을 받았다.
항핵주변인자 검사의 형광 강도가 1+, 2+인 경우와 3+, 4+인 경 우 각각 1점과 2점을 부여했을 때에 18.9%, 2점과 3점을 부여했을 때에 43.4%, 3점과 4점을 부여했을 때 77.4%의 환자가 ACR/EU- LAR criteria상 6점 이상이었다(Table 3).
고 찰
본 연구 결과 항핵주변인자 검사의 형광 강도에 따른 ACR/EU- LAR criteria 점수의 유의한 차이는 없었으나 항핵주변인자 검사의 형광강도 등급의 증가에 따라 전반적으로 ACR/EULAR criteria의 점수가 증가하는 양상이 관찰되었다. 저자들이 시행한 이전연구 [9]에서도 항핵주변인자 검사의 형광 강도에 비례하여 류마티스관 절염으로 진단되는 환자의 비율이 증가하는 결과를 얻은 바 있다.
ACR/EULAR criteria의 점수가 통계적으로 유의한 차이가 없었
Table 1. Median values of CRP, ESR, number of joint involvement andscore of ACR/EULAR criteria according to the fluorescence intensity of APF test
Fluorescence
intensity of APF 1+ (N=31) 2+ (N=16) 3+ (N=5) 4+ (N=1) P value CRP (mg/dL) <0.3 <0.3 <0.3 <0.3 NS
ESR (mm/hr) 8 12 23 28 NS
Small joint 1 2 1 6 NS
Large joint 1 2 1 2 NS
A CR/EULAR criteria score
3.0 3.5 4.0 5.0 NS
Abbreviations: CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; ACR/
EULAR criteria, American College of Rheumatology/European League against Rheumatism classification criteria for rheumatoid arthritis; APF, antiperinuclear factor; NS, not significant.
Table 2. ACR/EULAR criteria scores and modified scores of 53 patients according to level of the fluorescence intensity of APF test Case No. APF ACR/EULAR
criteria score Plus 1* Plus 2† Plus 3‡ Plus 4§ Case No. APF ACR/EULAR
criteria score Plus 1* Plus 2† Plus 3‡ Plus 4§
1 1+ 1 2 3 4 5 28 1+ 4 5 6 7 8
2 1+ 2 3 4 5 6 29 1+ 5 6 7 8 9
3 1+ 2 3 4 5 6 30 1+ 5 6 7 8 9
4 1+ 2 3 4 5 6 31 1+ 5 6 7 8 9
5 1+ 2 3 4 5 6 32 2+ 2 3 4 5 6
6 1+ 2 3 4 5 6 33 2+ 2 3 4 5 6
7 1+ 2 3 4 5 6 34 2+ 2 3 4 5 6
8 1+ 3 4 5 6 7 35 2+ 2 3 4 5 6
9 1+ 3 4 5 6 7 36 2+ 2 3 4 5 6
10 1+ 3 4 5 6 7 37 2+ 3 4 5 6 7
11 1+ 3 4 5 6 7 38 2+ 3 4 5 6 7
12 1+ 3 4 5 6 7 39 2+ 3 4 5 6 7
13 1+ 3 4 5 6 7 40 2+ 4 5 6 7 8
14 1+ 3 4 5 6 7 41 2+ 4 5 6 7 8
15 1+ 3 4 5 6 7 42 2+ 4 5 6 7 8
16 1+ 3 4 5 6 7 43 2+ 4 5 6 7 8
17 1+ 3 4 5 6 7 44 2+ 4 5 6 7 8
18 1+ 3 4 5 6 7 45 2+ 5 6 7 8 9
19 1+ 3 4 5 6 7 46 2+ 5 6 7 8 9
20 1+ 3 4 5 6 7 47 2+ 5 6 7 8 9
21 1+ 3 4 5 6 7 48 3+ 3 4 5 6 7
22 1+ 3 4 5 6 7 49 3+ 3 4 5 6 7
23 1+ 4 5 6 7 8 50 3+ 4 5 6 7 8
24 1+ 4 5 6 7 8 51 3+ 4 5 6 7 8
25 1+ 4 5 6 7 8 52 3+ 4 5 6 7 8
26 1+ 4 5 6 7 8 53 4+ 5 6 7 8 9
27 1+ 4 5 6 7 8
*Give 1 point for the positivity of APF test in ACR/EULAR criteria. †Give 2 points for the positivity of APF test in ACR/EULAR criteria. ‡Give 3 points for the positivity of APF test in ACR/EULAR criteria. §Give 4 points for the positivity of APF test in ACR/EULAR criteria.
Abbreviations: ACR/EULAR criteria, American College of Rheumatology/European League against Rheumatism classification criteria for rheumatoid arthritis; APF, antiperinu- clear factor.
던 것은 이 분류 방식의 점수체계가 사용 편의성을 위해 본래 점수 를 반올림하여 정수로 만들어 적용한 점과 관련이 있을 것이라 생 각한다 . 정수화된 점수 체계는 검사의 진단적 가치 차이가 크지 않 은 경우 이를 충분히 반영하지 못하는 경향이 있다. 실제 ACR/EU- LAR criteria에서도 급성기반응물질에 대한 진단적 가치를 평가하 는 초기 설정에서는 검사의 정량적 수치의 차이에 따라 각각 1.2와 1.7의 차등화된 점수가 부여되었으나 점수의 재조정 및 정수화 과 정에서 정량적 수치와 관계없이 1점으로 통합된 바 있다[1].
항핵주변인자 검사의 형광강도에 따른 차등화된 점수를 적용하 는 방안이 진단 정확도의 개선하는 측면에서 더 의미가 있을 것으 로 생각되나 현재의 ACR/EULAR criteria의 진단 틀을 크게 변화시 키지 않는 한도 내에서 항핵주변인자 검사의 점수를 부여하기 위 해서 항핵주변인자 검사 양성인 경우 모두 동일한 점수를 부여하 는 방안이 더 현실적이라고 생각한다.
ACPA 검사에 부여하는 점수인 2점과 3점을 항핵주변인자 검사 에도 동일하게 적용한 경우 각각 39.6%와 77.4%의 환자가 총점 6 점 이상인 “definite rheumatoid arthritis” 그룹으로 변경되었다. 항 핵주변인자 검사가 anti-CCP 검사보다 류마티스 관절염에 대해 특 이도가 높은 점을 고려할 때 3점 이상의 점수를 부여하는 것이 보 다 합당하다고 사료된다. 다만 항핵주변인자 검사 역시 anti-CCP 검사와 마찬가지로 시트룰린(citrulline)을 항원 결정기(antigenic determinant)로서 작용한다는 공통점을 고려할 때[10] ACPA 검사 항목에 부여할 수 있는 최대 점수(3점)를 초과하는 점수를 적용 하는 방안에 대해서는 추가 연구를 통해 이에 대한 타당성 여부를 확인할 필요가 있겠다.
최근 여러 연구에서 류마티스관절염의 진행 과정에서 발생할 수 있는 관절의 영구적 손상을 방지하기 위해 조기진단의 중요성이 강조되고 있다[11-13]. ACR/EULAR criteria를 제창한 미국 및 유럽 의 류마티스 연구 그룹은 anti-CCP 검사를 진단 항목에 포함시켜
개정한 해당 분류 방식이 류마티스 관절염의 조기 진단을 위한 지 표로 주목받고 있는 anti-CCP 검사[14, 15]를 진단 항목에 포함시켜 이전에 사용하던 류마티스관절염 분류체계(1987 revised criteria [16])보다 류마티스 관절염의 조기 진단 면에서 유리하다고 주장한 바 있다[1].
그러나 Yuko 등[17]의 연구에 따르면 류마티스인자 검사 및 anti- CCP 검사 음성인 환자에 대한 ACR/EULAR criteria의 진단 민감도 는 15.8%에 불과하였다. ACR/EULAR criteria가 기존의 분류 체계 보다 혈청학적 검사에 대한 의존도가 높은 점을 고려할 때 anti- CCP 검사 및 류마티스인자 음성인 류마티스관절염의 조기진단에 현재의 ACR/EULAR criteria는 적합하지 않으며 이를 보완할 수 있 는 검사지표가 필요할 것으로 사료된다. 저자들은 항핵주변인자 검사가 이를 어느 정도 보완 가능할 것이라고 생각한다. 또한 보다 정확한 진단을 위해 새로운 류마티스관절염의 지표로 주목받고 있는 autoimmune target (AIT) 검사를 이용한 항 MTOC-MT (mi- crotubule organizing center-microtubule) 항체[7]의 적용 방안에 대해서도 연구해 볼 필요가 있다고 생각한다.
결론적으로 저자들은 현재의 ACR/EULAR criteria를 크게 변화 시키지 않는 범위 내에서 ACR/EULAR criteria의 상기 문제점을 개 선하기 위하여 항핵주변인자 검사를 ACPA에 포함시키고 그 형광 강도 결과와 상관이 없이 양성인 경우 전부 3점을 부여하는 방안 을 제안하는 바이다.
요 약
배경: 류마티스 인자 검사와 ACPA검사는 ACR/EULAR criteria에 서 류마티스관절염의 진단을 위한 혈청학적 검사 항목으로 포함되 어 있다. 항핵주변인자(antiperinuclear antibody) 검사는 ACPA 검 사의 원조에 해당하는 검사로 류마티스관절염에 대한 높은 특이
Table 3. Prevalence of patients who were scored 6 or greater when APF tests were applied in ACR/EULAR criteria systemAPF scoring methods Prevalence of patients who were scored 6 or greater according to APF FI level (%)
1+ 2+ 3+ 4+ Total
1 point for positive APF 9.7 18.8 0.0 100.0 13.2
2 point for positive APF 29.0 50.0 60.0 100.0 39.6
3 point for positive APF 77.4 68.8 100.0 100.0 77.4
4 point for positive APF 96.8 100.0 100.0 100.0 98.1
1 point for 1+ FI/2 point for 2+,3+,4+ FI 9.7 50.0 60.0 100.0 28.3
2 point for 1+ FI/3 point for 2+,3+,4+ FI 29.0 68.8 100.0 100.0 49.1
3 point for 1+ FI/4 point for 2+,3+,4+ FI 77.4 100.0 100.0 100.0 86.8
1 point for 1+, 2+ FI/2 point for 3+,4+ FI 9.7 18.8 60.0 100.0 18.9
2 point for 1+, 2+ FI/3 point for 3+,4+ FI 29.0 50.0 100.0 100.0 43.4
3 point for 1+, 2+ FI/4 point for 3+, 4+ FI 77.4 68.8 100.0 100.0 77.4
Abbreviations: APF, antiperinuclear factor; ACR/EULAR criteria, American College of Rheumatology/European League against Rheumatism classification criteria for rheuma- toid arthritis; FI, fluorescence intensity.
도를 보이면서 류마티스인자 음성/anti-cyclic citrullinated peptide (anti-CCP) 음성인 류마티스관절염에서 자가항체를 검출할 수 있 음에도 불구하고 ACR/EULAR criteria의 혈청학적 검사 항목에 포 함되지 않았다. 저자들은 항핵주변인자 검사를 ACR/EULAR crite- ria에 적용하기 위한 방안을 연구하기 위해 본 연구를 시행하였다.
방법: 류마티스관절염이 의심되는 53명의 환자를 대상으로 임상 증상 및 검사 결과를 조사하였다. 대상 환자들은 전원 류마티스인 자 음성, anti-CCP 검사 음성이면서 항핵주변인자 검사 양성이었 다 . 항핵주변인자 검사의 형광 강도(1+, 2+, 3+, 4+)에 따라 환자를 4개의 그룹으로 구분하였고 항핵주변인자 양성 소견에 대해 1에서 4점까지 점수를 부여했을 때 ACR/EULAR criteria의 점수가 6점 이 상인 환자의 비율을 조사하였다.
결과: 항핵주변인자 검사의 형광 강도가 증가함에 따라 평균 ACR/EULAR criteria 점수가 증가하는 양상을 보였으나 해당 4개 의 그룹의 ACR/EULAR criteria 점수는 유의한 차이가 없었다(P
>0.05). 항핵주변인자 양성에 대해 2점 및 3점을 ACR/EULAR crite- ria에 적용하도록 하였을 때 6점 이상이 된 환자의 비율은 각각 39.6%와 77.4%였다.
결론: ACR/EULAR criteria의 ACPA 검사 항목에 항핵주변인자 항 목도 포함시키고 항핵주변인자 검사 양성인 경우 형광 강도와 관 계 없이 3점을 부여하는 방안이 바람직할 것으로 사료된다.
참고문헌
1. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO 3rd, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism col- laborative initiative. Arthritis Rheum 2010;62:2569-81.
2. Neinhuis RL and Mandema E. A new serum factor in patients with rheumatoid arthritis: the antiperinuclear factor. Ann Rheum Dis 1964;
23:302-5.
3. Youinou P, Le Goff P, Dumay A, Lelong A, Fauquert P, Jouquan J. The antiperinuclear factor. I. Clinical and serologic associations. Clin Exp Rheumatol 1990;8:259-64.
4. Manera C, Franceschini F, Cretti L, Braga S, Cattanec R. Clinical het- erogeneity of rheumatoid arthritis and the antiperinuclear factor. J Rheumatol 1994;21:2021-5.
5. Kim SG, Jung KY, Suh HS, Choe JY, Chung SH, Kim CG, et al. Is it fea- sible to adopt a commercialized APF kit as a routine diagnostic tool for rheumatoid arthritis. Arthritis Rheum 2001;44:S364.
6. van Jaarsveld CH, ter Borg EJ, Jacobs JW, Schellekens GA, Gmelig-
Meyling FH, van Booma-Frankfort C, et al. The prognostic value of the antiperinuclear factor, anti-citrullinated peptide antibodies and rheu- matoid factor in early rheumatoid arthritis. Clin Exp Rheumatol 1999;
17:689-97.
7. Kim DA and Kim TY. Anti-microtubule organizing center with micro- tubule by autoimmune target test is also useful serological marker in rheumatoid arthritis evaluation. Rheumatol Int DOI 10.1007/s00296- 011-2228-9.
8. Kim DA, Jearn LH, Kim TY. Antiperinuclear factor test is more useful than anti-Sa assay when used with anti-cyclic citrullinated peptide test in diagnosis of rheumatoid arthritis. J Rheumatol 2007;34:1944-5.
9. Kim TY, Oh J, Park IK, Yoo DH, Kim SY. Fluorescence intensity scor- ing of antiperinuclear factor at the 1:20 threshold in rheumatoid arthri- tis. Arthritis Rheum 1999;42(S9):S348.
10. Schellekens GA, de Jong BA, van den Hoogen FH, van de Putte LB, van Venrooij WJ. Citrulline is an essential constituent of antigenic de- terminants recognized by rheumatoid arthritis-specific autoantibod- ies. J Clin Invest 1998;101:273-81.
11. Bijlsma JW and Weinblatt ME. Optimal use of methotrexate: the ad- vantages of tight control. Ann Rheum Dis 2007;66:1409-10.
12. Pincus T, Yazici Y, Sokka T, Aletaha D, Smolen JS. Methotrexate as the
“anchor drug” for the treatment of early rheumatoid arthritis. Clin Exp Rheumatol 2003;21(S31):S179-85.
13. Visser K and van der Heijde D. Optimal dosage and route of adminis- tration of methotrexate in rheumatoid arthritis: a systematic review of the literature. Ann Rheum Dis 2009;68:1094-9.
14. Nielen MM, Schaardenburg D, Reesink HW, van de Stadt RJ, van der Horst-Bruinsma IE, de Koning MH, et al. Specific autoantibodies pre- cede the symptoms of rheumatoid arthritis: a study of serial measure- ments in blood donors. Arthritis Rheum 2004;50:380-6.
15. Rantapää-Dahlqvist S, de Jong BA, Berglin E, Hallmans G, Wadell G, Stenlund H, et al. Antibodies against cyclic citrullinated peptide and IgA rheumatoid factor predict the development of rheumatoid arthritis.
Arthritis Rheum 2003;48:2741-9.
16. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 1988;31:315-24.
17. Kaneko Y, Kuwana M, Kameda H, Takeuchi T. Sensitivity and specific- ity of 2010 rheumatoid arthritis classification criteria. Rheumatology (Oxford) 2011;50:1268-74.