투고일: 2011년 6월 15일, 심사일: 2011년 6월 20일, 게재확정일: 2011년 7월 1일 책임저자:류주석, 경기도 성남시 분당구 야탑동 351
(463-712) 차의과학대학교 분당차병원 재활의학과 Tel: 031) 780-6285, Fax: 031) 780-6206 E-mail: [email protected]
Copyrights ⓒ The Korean Dysphagia Society, 2011.
연하식이의 처방 시 고려해야 할 점과 주의점
류주석
차의과학대학교 분당차병원 재활의학과
Considerations and Problems in the Prescription of Dysphagia Diets
Ju Seok Ryu, M.D.
Department of Rehabilitation Medicine, CHA Bundang Medical Center, CHA University, Seongnam, Korea
Dysphagia refers to all types of anomaly that may occur at all courses of oral cavity, pharyngeal cavity, and esoph- ageal cavity by ingestion of food material. Dysphagia may range from light issues such as delay in meal times, dis- comfort, and coughing when eating to more serious issues such as malnutrition, dehydration, and aspiration pneu- monia, even leading to fatality and thus requires great caution. Therefore the diet provided to dysphagia patients requires extra caution, and efforts should be made to supply an appropriate amount. In order to provide food to dysphagia patients, the viscosity is controlled typically based on the videofluroscopic swallowing test. In order to prescribe the dysphagia diet, it would be necessary to accurately evaluate the deglutition function of the patient, understand the natural progress of basic disorder which led to dysphagia, and provide food of appropriate viscosity and texture. Also, a unified guideline must be prepared for the diet used in videofluroscopic swallowing study, the diet provided to actual patients, and the commercialized deglutition assisting additives to provide safe diet to the patients. Therefore, this report shall examine the points to consider when prescribing dysphagia diet to dysphagia patients and the commonly encountered issues when making such prescription. (JKDS 2011;1:80-84)
Keywords: Dysphagia, Diet, Prescription
서론
연하장애란 음식물을 섭취하여 구강기, 인두기 및 식도 기 전 과정에서 발생할 수 있는 모든 이상을 총칭한다. 연 하장애는 음식을 먹을 때 식사 시간의 지연, 불편감, 기침과 같은 가벼운 문제에서부터 영양장애, 탈수, 흡인성 폐렴과 같은 심각한 문제를 일으킬 수 있으며, 심지어 사망에 이를 수도 있어서 매우 주의를 요한다.
연하장애의 유병률은 급성기 뇌졸중 환자를 대상으로 한
연구에서 약 27-50%로 나타났고, 이 환자들 중 1/5-1/3에 서 연하장애와 관련된 합병증이 발생한다고 보고되었다1-4. 또 연하장애는 급성기 치료기관에서는 약 10%, 요양원에서 는 약 30-60%에서 발생하며, 이들 중 뇌졸중 환자들만을 고려하였을 때 약 75% 이상에 발생한다5. 2006년 Carnaby 등은 뇌졸중 후 고강도의 행동요법 치료와 연하처방을 시행 한 경우 연하 관련 합병증을 유의하게 감소시켰고, 연하 기 능의 호전을 가져왔다고 보고하였고6, 뇌졸중 환자에서 연 하장애를 치료할 경우 영양상태의 호전을 보인다는 보고도
있다7.
그러므로 연하장애 환자들에게 제공하는 식이는 특히 주 의를 요하며, 환자의 상태를 고려하여 더 안전하게, 적절한 양을 공급하기 위한 노력이 필요하겠다. 적절한 영양 공급 이 가능한 경우에만 건강을 유지할 수 있고, 삶의 질도 높아 질 수 있을 것이다.
연하장애 환자들에게 음식을 제공하기 위해서 흔히 비디 오 투시 연하검사에 의거하여 점도를 조절하게 된다. 그러 나 비디오 투시 연하검사가 불가능한 병원도 있고, 단지 환 자의 연하장애의 진단에만 이용되기도 한다. 연하장애 식 이를 처방하기 위해서는 환자의 연하 기능을 정확히 평가하 는 것과 실제 식사를 제공하는 영양사 사이에 충분한 의사 소통과 협력이 있어야만 환자에게 적절한 식이를 제공할 수 있을 것이다8.
그러므로, 본 고에서는 연하장애 환자에서 연하 식이를 처방할 때 고려해야 할 점과 연하식이를 처방할 때 흔히 접하는 문제점에 대해 살펴보고자 한다.
본론
1. 연하장애의 평가
연하장애를 겪고 있는 환자는 다양한 증상과 징후를 보 이게 된다. 식사 중 기침을 하거나 숨이 막힘을 호소할 수 있고, 코로 음식이 나오는 경우도 있다. 식사 중 심장 박동 수가 감소할 수도 또는 증가할 수도 있으며, 연하 후 목소리 가 바뀌기도 한다. 적절한 양을 섭취하지 못하여 체중이 감 소하거나 반복적인 상기도 감염과 흡인성 폐렴 등의 증상을 보이기도 한다. 이러한 증상을 보이는 환자들에게 적절한 식이를 제공하기 위해서는 연하장애의 정확한 진단이 선행 되어야 하겠다. 연하장애의 진단에는 비디오 투시 연하검 사, 굴곡성 내시경 검사, 초음파 검사, 핵의학적 검사, 근전 도 검사, 전기성문검사(electroglottography), 압력측정기 (manometry), 음성 분석 등의 다양한 방법이 이용될 수 있다. 이 중 비디오 투시 연하검사는 평가의 표준 검사로 매우 널리 이용되고 있으며, 다양한 질감과 점도에 따른 연 하상태를 평가할 수 있어서 연하식이를 제공할 때 특히 중 요한 검사이다9.
2. 안전적 측면
1) 기도흡인의 병태생리
연하장애 환자들이 안전하게 음식을 섭취하기 위해서는 점도에 따른 기도흡인의 병태생리를 이해하는 것이 필요 하다. Perlman 등은 비디오 투시 조영 검사를 이용하여
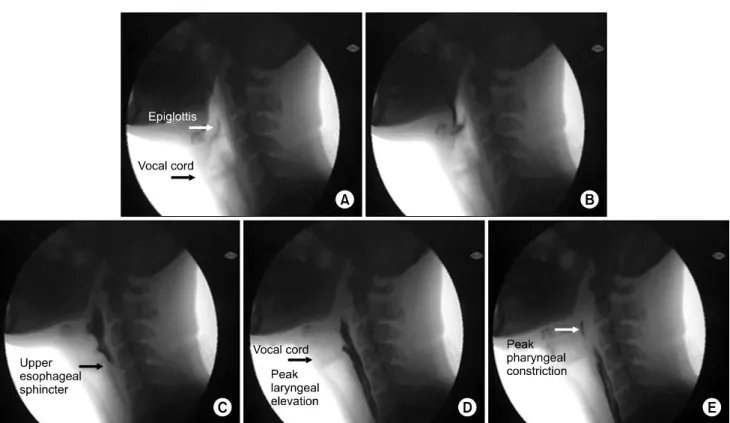
삼킴의 지연(delayed swallow), 하인두의 정체(hypop- haryn geal stasis), 소와의 정체(vallecularstasis), 설골 거상의 제한(reduced hyoid elevation), 후두개 기능의 이상(deviated epiglottic function) 등이 기도흡인의 유 의한 위험인자임을 보고하였고10, Choi 등은 비디오 투시 연하검사를 운동 형상학적으로 분석하여 기도흡인의 병태 생리를 알아보았다.(Fig. 1) 기도흡인의 원인을 식괴의 점 도에 따라 나누어서 분석하였을 때, 고점도 식괴의 경우 상부 식도 괄약근이 열리는 기간과 기도의 상ㆍ하방 이동 거리가 짧은 경우 흡인의 위험이 증가하였고, 저점도 식 괴의 경우 인두기의 시작 후 후두 거상까지의 기간과 인 두 근육의 수축이 일어나는 기간이 지연된 경우와 식괴가 소와 주머니(vallecular pouch)에 닿은 뒤 후두 거상이 일어나는 시간 간격이 지연된 경우에 흡인의 위험이 유의 하게 증가하였다11.
2) 비디오 투시 연하검사
비디오 투시 연하검사는 현재상태의 연하장애를 평가하 는데 가장 널리 이용되는 방법이다. 비디오 투시 조영 검 사는 비용적 측면이나 편리성 등에서 매우 장점이 많으 며, 특히 음식을 다양한 질감과 점도로 나누어 양을 달리 하여 제공하면서 검사를 수행할 수 있어서 연하 식이를 처방하는데 특히 유용한 검사 방법이다. Stowd 등은 비 디오 투시조영검사에서 사용된 식이와 실제 임상에서 상 용화된 제품 들을 현재 표준으로 받아들여지는 National Dysphagia Diet (NDD) guideline과 비교하였을 때 많 은 차이를 보인다는 연구결과를 발표하였다12,13. 또한 연 하보조 첨가제를 만드는 회사마다 점도의 기준이 다르다 는 점도 보고하였다12. 이는 실제 비디오 투시 연하검사 결과를 바탕으로 상용화된 제품을 선택 및 적용할 경우 기도흡인과 같은 위험성이 발생할 가능성이 높음을 의미 한다. 그러므로 비디오 투시 연하검사를 시행하는 의사와 환자에게 식이를 제공하는 영양사, 그리고 연하보조 첨가 제를 만드는 기업간에 통일된 지침을 개발할 필요가 있 고, 이를 위해 상호간의 협력이 필요한 것으로 보인다8,13. Table 1은 2001년 미국 영양학회(American Dietetic Association)에서 제안한 음식 종류에 따른 점도를 나타낸 표이다.
3) 기저질환의 자연경과
연하장애는 다양한 질환에서 발생할 수 있다. 그러나 연하장애 식이를 제공할 때는 병의 자연경과를 파악할 필 요가 있겠다. 예를 들어 뇌졸중의 경우증상 발생 후 24시 간 이내에는 임상적으로 약 51% 환자에서 연하장애의 위 험을 보이나, 약 7일이 경과하면 27% 정도에서만 연하장
Fig. 1. Swallowing processes of a normal person. A. Initiation of pharyngeal phase. B. Latency of epiglottis contact. C. Latency of UES opening. D. Latency of peak laryngeal elevation. E. Latency of peak pharyngeal constriction.
Table 1. Proposed terms and viscosity range for dysphagia diet food (2002, American Dietetic Association).
Liquid Viscosity range, cP
Thin Nectar-like Honey-like Spoon-thick
1-50 51-350 351-1750
>1750 From the National Dysphagia Diet Task Force.
애의 위험을 보이게 된다. 6개월이 경과한 시점에서는 약 11%로 감소하게 된다3,14. 이와 같이 질환이 발생할 당시 부터 연하장애를 호소하다가 신경학적 회복으로 인해 연 하기능이 호전되는 경우도 있겠고, 운동신경원성 질환이 나 치매, 피킨슨씨 병과 같이 속도에서는 차이가 있을 수 있으나 점차 악화되는 경과를 보이는 질환도 있다15. 또한 두경부 암과 같이 수술 후 바로 연하장애가 발생할 수도 있으며, 방사선 치료 후 발생하는 연하장애의 경우 수개 월 후에 처음 발생하여 점차 악화되기도 한다16,17. 그러므 로 현재 상태에서 연하장애의 정도를 파악하는 것 뿐만 아니라 향후 병의 경과에 따라 이에 대비하여 연하 식이 의 처방을 고려하는 것이 더 안전하고 환자의 만족도를
높일 수 있을 것이다.
3. 섭취의 양 1) 질감(Texture)
2002년 미국 영양학회에서는 재활의학과에 종사하는 영양사와 언어치료사, 음식 관련 과학자, 기업 종사자 등 이 모여 National dysphagia diet task force team을 결 성하였고, Dysphagia outcome and severity scale (DOSS)를 이용하여 연하장애의 심각도에 따라 질감의 제 한 정도를 비교하여 NDD 지침을 만들었다. NDD 지침 은 환자의 연하장애의 심각도에 따라 어떤 단계의 연하장 애 식이를 제공하는 것이 적절한지를 안내하기 위함이다.
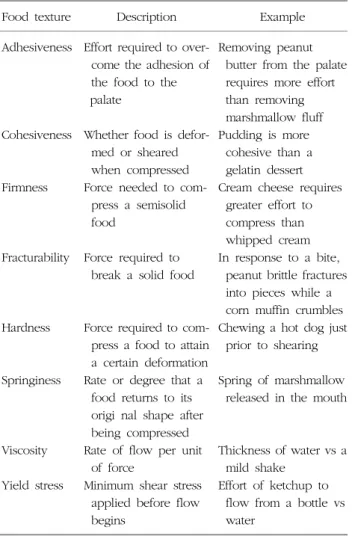
환자에게 고형식을 제공할 때는 질감에 따라 구분하게 되 며, 질감은 부착성(adhesiveness), 응집성(cohesivene- ss), 견고성(firmness), 파쇄성(fracturability), 경도성(ha- rdness), 탄성(springiness), 점성(viscosity), 항복 응력 (yield stress) 등의 특성으로 이루어져있다. Table 2는 질감을 구성하는 특성을 나열하였다.
NDD는 식이의 변형(dietary modification)의 정도를 1 단계에서 4단계로 나눈다. 1단계는 pureed diet이며, 2단 계는 mechanically altered, 3단계는 advanced, 4단계는
Table 2. Food textures that affect the management of dysphagia (National Dysphagia Diet: Felt, P., et al. 2002).
Food texture Description Example
Adhesiveness
Cohesiveness
Firmness
Fracturability
Hardness
Springiness
Viscosity Yield stress
Effort required to over- come the adhesion of the food to the palate
Whether food is defor- med or sheared when compressed Force needed to com-
press a semisolid food
Force required to break a solid food
Force required to com- press a food to attain a certain deformation Rate or degree that a food returns to its origi nal shape after being compressed Rate of flow per unit
of force
Minimum shear stress applied before flow begins
Removing peanut butter from the palate requires more effort than removing marshmallow fluff Pudding is more
cohesive than a gelatin dessert Cream cheese requires
greater effort to compress than whipped cream In response to a bite,
peanut brittle fractures into pieces while a corn muffin crumbles Chewing a hot dog just
prior to shearing Spring of marshmallow
released in the mouth
Thickness of water vs a mild shake
Effort of ketchup to flow from a bottle vs water
Table 3. The levels of dietary modification as defined by the National Dysphagia Diet.
Dietary modification Description Level 1: Pureed
Level 2: Mechanically altered
Level 3: Advanced
Level 4: Regular
Pureed, homogenous, and cohesive (pudding-like) fo ods, not those that require bolus formation, controlled manipulation, or mastication
Moist, soft-textured foods that are easily formed into a bolus, meats that are ground or minced (pieces no larger than one-fourth of an inch) but are moist with some cohesion; level 1 food items are also allowed Nearly all textures except for hard,
sticky, or crunchy food; foods still need to be moist and bite-size All foods
regular diet로 구성된다. 각각의 특징은 Table 3에 기술되 어 있다.
2) 환자의 인지 능력 및 연하의 동기
환자에게 충분한 양의 식이를 공급하기 위해서는 환자 의 인지장애에 대한 평가가 필요하다. 인지기능이 저하된 환자에서는 연하 중 기도흡인이 발생할 가능성이 높으며, 충분한 양의 식이를 공급하는 데에도 어려움이 있겠다.
또한 환자의 먹으려는 의지가 먹는 양에 영향을 미칠 수 있다. 그러므로 환자의 인지 상태와 의욕을 파악하여 이 에 적절한 식이를 제공하는 것뿐만 아니라 약물치료, 재 활의학적 치료를 병행하는 것이 필요하겠다18.
3) 음식 선호도
음식의 질감의 변형은 식괴를 먹기 쉽게 만들고, 흡인 의 위험을 낮추는 것이 안전성의 측면에서 가장 중요한 요소이다. 현재까지 이와 같은 목적을 위해 다양한 연하
첨가물들이 개발되어 사용되고 있어서 많은 연하장애 환 자들에게 삼킴의 즐거움을 되찾아주고 있다. 그러나 향후 에는 연하를 유도하고 촉진하는 등과 같은 다른 목적의 연하보조 첨가물의 개발이 필요할 것으로 기대되고, 이에 대한 연구가 진행되고 있는 상태이다19.
환자에게 적절한 양의 음식을 제공하기 위해서는 환자를 중심으로 가능한 개별적으로 철저히 평가한 후 적절한 식이 를 제공하여야 한다. 환자들에게 식이와 관련하여 선택의 기회를 제공하는 것은 영양의 공급을 가능하게 하고, 환자 에게 음식을 섭취하고 싶은 욕구를 증가시킴과 동시에 먹는 즐거움을 줄 수 있으며, 그 결과 체중의 감소도 줄일 수 있다5. 미국 보건복지부(U.S. Department of health &
human services) 산하 연방 해석 지침(federal interpre tive guidelines)을 보면, 환자가 원하고, 먹을 수 있는 질감 보다 낮은 단계로(downgrading the texture) 음식을 제공 할 경우 음식 섭취량의 감소를 가져오므로, 이를 고려하여 가능한 최대로 환자의 기호를 파악하는 것이 필요하고, 질 감에 관해서는 환자의 연하능력에 맞도록 환자를 재평가하 여 질감을 높게 제공하는 것이 필요하겠다20.
4) 지구력 및 피로도
고령일 경우나 여러 연하 관련 질환을 앓아온 경우, 오 랜 기간 동안 경구 식이를 하지 않은 경우 등에서는 지구 력의 저하가 오게 된다. 이 경우 갑자기 충분한 양을 경 구로 섭취하는 것이 불가능할 수도 있으며, 갑자기 많은 양을 경구로 섭취할 경우 지구력의 저하에 의해 기도 흡 인이 발생할 가능성도 높다. 그러므로 환자의 질환 상태
및 지구력에 대한 파악을 바탕으로 하여 적절한 양의 음 식을 제공해야만 하겠다. 현재까지 이에 대한 연구는 부 족한 상태여서 추가적인 연구가 필요할 것으로 생각된다.
결론
연하장애 환자들에게 식이를 제공할 때에는 특히 주의를 요한다. 환자의 연하 능력을 고려하여 더 안전하게, 또 필 요한 양을 적절히 공급하기 위한 노력이 필요하겠다. 연하 장애 환자들에게 안전하게, 적절한 양의 음식을 제공하기 위해서 흔히 비디오 투시 연하검사에 의거하여 점도를 조절 하게 된다. 그러므로 비디오 투시 조영검사에서 사용되는 식이와 실제 환자들에게 제공하는 식이, 그리고 상용화된 연하보조 첨가제 사이에 충분한 의사소통과 협력을 기반으 로 하여 점도와 질감에 관련된 통일된 지침을 적용하여야만 환자에게 안전한 식이를 제공할 수 있을 것이다.
REFERENCES
1. Mann G, Hankey GJ, Cameron D. Swallowing disorders following acute stroke: prevalence and diagnostic accuracy. Cerebrovasc Dis. 2000;10:380-6.
2. Mann G, Hankey GJ, Cameron D. Swallowing function after stroke: prognosis and prognostic factors at 6 months. Stroke. 1999;30:744-8.
3. Smithard DG, O'Neill PA, England RE, Park CL, Wyatt R, Martin DF, et al. The natural history of dysphagia fol- lowing a stroke. Dysphagia. 1997;12:188-93.
4. Wolfe CD, Taub NA, Woodrow J, Richardson E, Warburton FG, Burney PG. Patterns of acute stroke care in three districts of southern England. J Epidemiol Community Health. 1993;47:144-8.
5. Niedert KC. Position of the American Dietetic Associa- tion: Liberalization of the diet prescription improves qua- lity of life for older adults in long-term care. J Am Diet Assoc. 2005;105:1955-65.
6. Carnaby G, Hankey GJ, Pizzi J. Behavioural intervention for dysphagia in acute stroke: a randomised controlled trial. Lancet Neurol. 2006;5:31-7.
7. Elmstahl S, Bulow M, Ekberg O, Petersson M, Tegner H.
Treatment of dysphagia improves nutritional conditions in stroke patients. Dysphagia. 1999;14:61-6.
8. Fremont K. Unlocking the mystery of dysphagia diets.
Dietary Manager. 2009:22-4.
9. Logemann JA. Manual for the videofluorographic study of swallowing. 2nd ed. Austin, Texas: Pro-Ed, 1993.
10. Perlman AL, Booth BM, Grayhack JP. Videofluoroscopic predictors of aspiration in patients with oropharyngeal dysphagia. Dysphagia. 1994;9:90-5.
11. Choi KH, Ryu JS, Kim MY, Kang JY, Yoo SD. Kinematic analysis of dysphagia: significant parameters of aspira- tion related to bolus viscosity. Dysphagia. 2011;E-pub.
12. Strowd L, Kyzima J, Pillsbury D, Valley T, Rubin B.
Dysphagia dietary guidelines and the rheology of nutri- tional feeds and barium test feeds. Chest. 2008;133:
1397-401.
13. The National Dysphagia Diet Task Force. The National Diet Dysphagia Diet: standardization for optimal care.
Chicago, IL: American Dietetic Association, 2002.
14. Steinhagen V, Grossmann A, Benecke R, Walter U.
Swallowing disturbance pattern relates to brain lesion lo- cation in acute stroke patients. Stroke. 2009;40:1903-6.
15. Higo R, Tayama N, Nito T. Longitudinal analysis of pro- gression of dysphagia in amyotrophic lateral sclerosis.
Auris Nasus Larynx. 2004;31:247-54.
16. Pauloski BR, Rademaker AW, Logemann JA, Lazarus CL, Newman L, Hamner A, et al. Swallow function and per- ception of dysphagia in patients with head and neck cancer. Head Neck 2002;24:555-65.
17. Logemann JA, Pauloski BR, Rademaker AW, Lazarus CL, Gaziano J, Stachowiak L, et al. Swallowing disorders in the first year after radiation and chemoradiation. Head Neck. 2008;30:148-58.
18. van der Maarel-Wierink CD, Vanobbergen JN, Bronkhorst EM, Schols JM, de Baat C. Risk factors for aspiration pneumonia in frail older people: a systematic literature review. J Am Med Dir Assoc. 2011;12:344-54.
19. Yamamura K, Kitagawa J, Kurose M, Sugino S, Takatsuji H, Mostafeezur RM, et al. Neural mechanisms of swal- lowing and effects of taste and other stimuli on swallow initiation. Biol Pharm Bull. 2010;33:1786-90.
20. CMS. Interpretive Guideline for F325. Assessed at http://
www.cms.gov