Corresponding author: Si-Gyun Roh, Department of Plastic and Reconstructive Surgery, Medical School, Chonbuk National University, Geumam 2-dong, Deokjin-ju, Jeonju 561-712, Korea
Tel: 82-63-250-1314, Fax: 82-63-250-1866 E-mail: [email protected]
마졸린씨 궤양의 치험례
최준영ㆍ오광진ㆍ노시균ㆍ이내호ㆍ양경무 전북대학교 의학전문대학원 성형외과학교실
Clinical Experience of Marjolin's Ulcers
Jun-Young Choi, Gwang-Jin Oh, Si-Gyun Roh, Nae-Ho Lee and Kyung-Moo Yang
Department of Plastic and Reconstructive Surgery, Medical School, Chonbuk National University, Jeonju, Korea
Purpose: Marjolin's ulcer is rare but highly aggressive malig- nant cancer that is associated with chronic, nonhealing wounds such as burn wound. There are no confirmed effec- tive protocols for treatment of this disease. This study was conducted to describe the clinical presentation and treatment modalities of Marjolin's ulcer in our hospital.
Methods: This was a retrospective study of Marjolin’s ulcer.
20 cases were histologically confirmed malignant skin cancer seen at Chonbuk National University Hospital from January 2000 to December 2011. Data were retrieved from patients’
medical records and photographs.
Results: The total 20 cases of Marjolin’s ulcer were studied.
Squamous cell carcinoma was the most common patho- logical type in 20 patients (100%). Lymph node metastasis at the time of diagnosis was recorded in 3 patient (15%). Wide excision was the most common surgical procedure per- formed in 17patients (85%) of cases. The reconstruction mo- dalities were various as free flap 3 patients (15%), skin graft 13 patients (65%), local advancement flap 2 patients (10%) and regional flap 1 patient (5%). Local recurrence was noted in 3 patients (15%) who had surgical treatment. And one pa- tient (5%) expired in hospital.
Conclusion: Marjolin’s ulcer is an infrequent lesion. Unfortu- nately the diagnosis and treatment are often delayed. If the wound was histologically confirmed, aggressive excision and reconstruction is warranted in these highly malignant skin cancer. Early recognition and aggressive treatment of Marjo- lin’s ulcers are essential to improve outcomes. (J Korean Burn Soc 2013;16:1 7-23)
Key Words: Burns, Skin cancer, Excision
INTRODUCTION
Jean-Nicolas Marjolin first described development of skin carcinoma in old burn scar in 1828, and the term of Marjolin’s ulcer has been used to describe malignant transformation mainly from burn wound1). Marjolin's ul- cer is a rare but highly aggressive malignant cancer that is associated with chronic and nonhealing wounds. It de- velops in not only chronic burn wound, but also chronic venous stasis ulcers, pressure sore, snake bites, osteomye- litis, frost bite, skin graft donor site, vaccination site and other ulcers1-4). The exact mechanism of malignant trans- formation of Marjolin’s ulcer is unclear and controversial.
Several theories including the toxin, chronic irritation, traumatic epithelial element implantation, heredity, im- munologic privileged site, co-carcinogen, ultraviolet rays, initiation and promotion and environmental and genetic interaction theories have been reported to explain the ma- lignant transformation5).
Despite these numerous risk factor, this oncologic dis- ease is, however, frequently overlooked and often inade- quately treated. Any suspicious lesions that arise within affected areas should have to perform multiple biopsies as a gold standard1,6). Early recognition and proper stag- ing offers the best chance for cure. Wide excision seems to be the most preferred method. The reconstruction mo- dalities were various as skin graft, local flap, regional flap and free flap. This is studied to describe the clinical pre- sentation and treatment modalities of Marjolin's ulcer in our hospital. There are no confirmed protocol for treat- ment of this disease. So we suggest the strategy of treat- ment and give a presentation on the outcome through ex-
Age/Sex Size of ulcer
Latent period
Duration of illness
Anatomical location
Histological finding
Regional meta
Distant
metastasis Recurrence Reconstruction operation 63/F 5×10 cm2 60 years 1 year Lower
extremity
Squamous cell carcinoma
− − − LD free flap
58/M 1.5×1.5 cm2 50 years 1 year Scalp Squamous cell carcinoma
− − − Rotation flap
64/M 15×10 cm2 57 years 5 month Lower extremity
Squamous cell carcinoma
+ (Inguinal LN
dissection)
− + LD free flap
15/M 2×2 cm2 7 years 1 year Lower extremity
Squamous cell carcinoma
− − − FTSG
85/M 5×2 cm2 60 years 2 months Lower extremity
Squamous cell carcinoma
− − − STSG
72/F 25×25 cm2 1 year 2 months Trunk Squamous cell carcinoma
− − − STSG
42/M 5×5 cm2 40 years 1 year Upper extremity
Squamous cell carcinoma
− − + STSG
80/M 5×10 cm2 40 years 2 months Upper extremity
Squamous cell carcinoma
+ (Axillary LN dissection)
+ (Abdominal cavity)
− Conservative Tx.
20/M 10×10 cm2 1 years 1 month Lower extremity
Squamous cell carcinoma
− − − STSG
51/M 8×4 cm2 45 years 1 month Lower extremity
Squamous cell carcinoma
− − − STSG
51/M 2×2 cm2 25 years 1 year Trunk Squamous cell carcinoma
− − − STSG
36/M 10×10 cm2 16 years 1 month Lower extremity
Squamous cell carcinoma
− − − STSG
64/M 12×7 cm2 60 years 1 year Lower extremity
Squamous cell carcinoma
− − − ALT free flap
46/M 15×15 cm2 16 years 8 years Lower extremity
Squamous cell carcinoma
+ (Inguinal LN dissection)
− − STSG
77/F 7×4 cm2 70 years 2 months Lower extremity
Squamous cell carcinoma
− − − STSG
54/F 5×10 cm2 40 years 1 year Lower extremity
Squamous cell carcinoma
− − − FTSG
73/F 8×4 cm2 10 years 5 years Lower extremity
Squamous cell carcinoma
− − − Local advancement
flap
48/M 10×10 cm2 35 years 1 month Trunk Squamous cell carcinoma
− − − STSG
37/M 13×10 cm2 30 years 1 month Upper extremity
Squamous cell carcinoma
− − − STSG
62/F 35×25 cm2 50 years 1 year Trunk Squamous cell carcinoma
− − − Rotation flap &
STSG LN = lymph node, LD = latissimus dorsi, STSG = split thickness skin graft, FTSG = full thickness skin graft, Tx = treatment Table 1. 20 Patients with Marjolin’s Ulcer
perience of 20 patients in our institute.
PATIENTS AND METHODS
This was a retrospective study of histologically con-
Fig. 1. MRI image: There is Marjoline's ulcer in the left posterior thigh.
Fig. 2. PET-CT: There is metastatic lymph nodes in the left inguinal area.
firmed cases of Marjolin’s ulcer. 20 patients with Marjo- lin’s ulcer were seen a period of 12 years from January 2000 to December 2011 at our institute (Table 1). The di- agnosis was made on the basis of past history, clinical ex- amination and confirmed by biopsy. Patient with in- complete data were excluded from the study. The data of patients were retrieved from patient’s medical records, photographs and histopathologic finding. Information in- cluded age and sex distribution, etiological agent, previ- ous causative lesion, size of ulcers, initial healing, latency period, duration of illness, anatomical location, radio- logical investigations, histological examination, regional metastasis (lymph node), distant metastasis (other organ), treatment modalities and local recurrences7). All patients were evaluated preoperatively with magnetic resonance imaging and computed tomography for recognition of tu- mor invade surrounding tissue. CT and MRI were helpful in determining not only invasion depth and size of cancer but also boundary of wide excision (Fig. 1). High-reso- lution ultrasonography was performed for lymph node.
And PET-CT was performed to find distant metastasis.
RESULTS
During the period under study, a total of 20 patients were studied. Our youngest patient was 15 years and the oldest 85 years of age at the time of diagnosis, the mean age being 57.1 years. Male were 13 patients (65%) and fe- male were seven patients (35%) with male to female ratio of 1.85 : 1. Burn scar was common lesion of Marjolin’s
ulcer, representing 90% of cases. Other 10% of cases were trauma lesions. The latent period calculated from the time of initial injury to the development of a malignant ulcer ranged from one year to 60 years, with a mean of 33.24 years. All the patients' were managed conservatively at the time of initial injury. And all patient were not per- formed skin graft. In one patient, the ulcer did not heal before the development of the malignancy as acute type.
The size of ulcers varied from 2×2 cm2 to 20×21 cm2 and the mean size was 90.3 cm2. The duration of the non- healing ulcer in the scar varied from two months to eight years with a mean duration of 1.4 years. The duration mentioned above started from the occurrence of ulcer- ation and ended with getting a histologic diagnosis for the patient.
13 patients (65%) had ulcerative lesions on the lower extremity, four patients (20%) on trunk, two patient (10%) on upper extremity and one patient (5%) on scalp. This will depend on the position of an initial wound.
All 20 patients were diagnosed of squamous cell carci- noma pathologically. And, lymph node metastasis at the time of diagnosis was recorded in 3 patients (15%). Physi- cal examination on the lymph node is necessary for all the patients who were histologically diagnosed. But this alone cannot accurately detect metastasis and an addi- tional radiological test is indispensable. In the department of surgery, Lymph node dissection was planned based on the results of ultrasonography and PET/CT (Fig. 2).
Resected lymph nodes were confirmed of metastatic lymph nodes after pathologic evaluations. Distant meta-
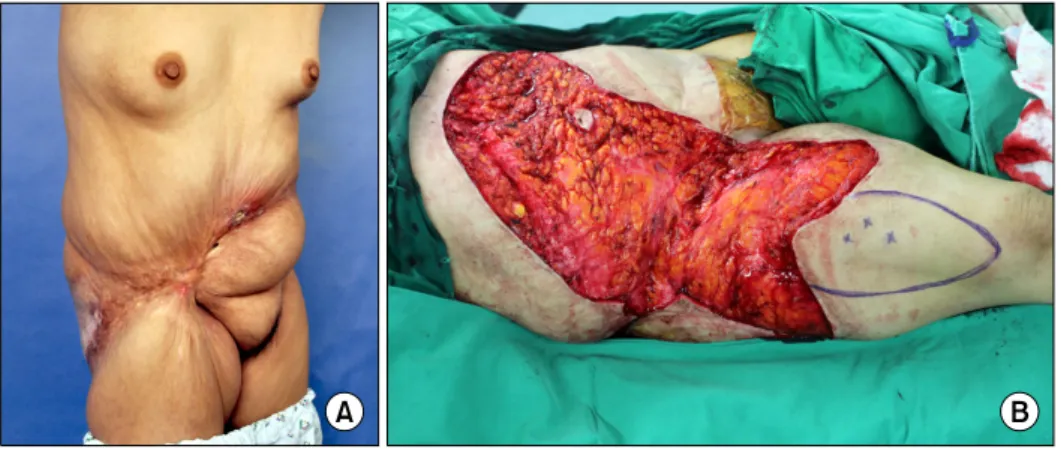
Fig. 3. (A) Patient with previous amputation, (B) Forequarter amputation, (C) Immediate postoperative photo: the STSG was perfor- med.
Fig. 4. (A) Marjolin's ulcer on the scalp, (B) Intraoperative photo: after the ulcer excision, (C) Myocutane- ous rotation flap.
stasis occurred in one patient (5%) and it occurred in the abdominal cavity. The patient underwent conservative treatments and expired four months later.
Surgical treatment can be considered with two catego- ries, (1) resection of cancer and (2) reconstruction of defect. Wide excision was performed for surgical re- section in 17 patients (85%) and amputation was per- formed in 2 patient (10%). Safety margin of 2.0 cm was initially planned and further excision of positive margin was performed based on frozen biopsy8).
Two patients (10%) required the amputation of extremi- ties. One patient had marjolin’s ulcer developed on the forearm. The patient had recurred cancer on axilla and upper arm after previous amputation of the upper arm.
The patient exhibited multiple lesions and metastasis of axillary lymph node and underwent forequarter amputa- tion at department of orthopedic surgery. There haven’t been any recurrences after forequarter amputation (Fig. 3).
The other patient showed 2×2 cm2 sized Marolin’s ulcer on middle finger. MRI revealed deep invasion down to soft tissue. Even with wide excision of the lesions, the function and shape of the affected finger could not be
preserved. Amputation was performed.
For eight patients (40%), spontaneous healing of the wound occurred and it was accompanied by scar con- tracture and remnant scar in surrounding area. Contra- cture release and scar excision were performed simulta- neously with wide excision. After resecting primary can- cer following reconstructive surgeries were performed. 2 patients (10%) underwent wound closure with local ad- vancement flap. In case of 1 patient (5%) whose lesion was developed on scalp have received myocutaneous ro- tation flap (Fig. 4). Skin graft had been performed on 13 patients (65%) which lead complete cure without any complications. Free flap was chosen to be method of re- construction in three patients (15%) (Fig. 5).
After surgery in the follow-up period three patients (15%) recurrence and two patients (10%) underwent wide excision and skin graft again. Until the recurrence occur, it took 12 months - 15 months for each patient. The wound size of recurrence were 20 cm2 and 24 cm2 without diffi- culty to wide excision, currently those patients is under observation through take outpatient treatment. Radiologi- cal test was performed for two patients to find out meta-
Fig. 6. (A) Primary cancer: preope- rative photo, (B) Reccrence of Mar- jolin's ulcer.
Fig. 5. (A) Marjolin's ulcer at lower extremity: about 25×15 cm sized defect is in the right popliteal fossa, (B) Follow up photo: using the LD free flap, the defect was covered.
stasis but there was no indication of metastasis. Recu- rrence occurred in the other one (5%) of the cases who underwent surgery of the primary tumor, Latissimus dor- si free flap. The site of recurrence exists with multiple flap periphery, each of the ulceration size was more than 20 cm2 as well. Cancer was relapsed within three months af- ter surgery. So we planned lower extremity amputation because of its aggressive nature (Fig. 6). The patient who leaves no reoperation because of no consent, maintains chemotherapy in oncology. The patient is also currently receiving outpatient treatment and receiving wound management. The most significant problem is cancer bleeding. Due to low hemoglobin state, the patient is re- ceiving regular transfusion. The type of bleeding was oozing and when receiving electrocauterization, it causes another bleeding. Currently, hemostasis was done by su- ture ligation and compression. But if rupture occurs, due to the invasion of cancer cell into the major vessel, a sud-
den death might happen due to acute bleeding.
DISCUSSION
Marjolin's ulcer is a malignant skin cancer that occurs in chronic nonhealing wound. Burn is the most common cause of the Marjolin's ulcer. Marjolin's ulcer of the ag- gressive and invasive properties were mentioned in many studies9). It occurred in 20 patients for 12 years in our hospital. One of them had expired, three had a recurren- ce. Various pathological subtypes exist, but the squamous cell carcinoma is the only endemic10-12).
The most important thing during the treatment of this disease is doubt that wound is cancer. Marjolin's ulcer has a previous wound history. Time later, wound healing and spontaneous re-ulcer occurs are characterized. Doubt of the cancer when the doctor care for patients with these history is very important.
The second most important thing is the education of patients. The doctor explained that the possibility of skin cancer when patients are in-patient or out-patient treat- ment for primary wound healing. When ulceration occurs in the scar, patients should not overlook this and should visit the hospital. At our hospital, patients who visited the hospital the fastest took two months that starts from the occurrence of ulceration and ends with getting a histo- logic diagnosis. Patients took the average time of 1.4 years. Using the two methods above, if you shorten the time it takes for the diagnosis, faster treatment and heal- ing through a small range of resection are possible.
Reconstructive surgery is not a burden to the patient, if defect size is smaller. Reducing the time that takes for the diagnosis should avoid deepening the stage and grade of tumor. Besides the recurrence rate was reduced because the size of the cancer and metastasis rate is reduced6). The third most important thing, to prevent malignant transformation, the initial wound needs to be treated to prevent its transformation into chronic unstable scar. For a deep second degree wound and more serious ones, rather than spontaneous healing, it is better to perform skin graft after clean excision.
After diagnosis, thorough preoperative evaluation is essential. It is necessary to perform physical exam for sur- rounding lymph node and sonography in order to find out whether lymph node metastasis occurred.
If lymph node metastasis is suspected, radical lymph node dissection or palliative lymph node dissection need to be performed along with wide excision of primary tumor. Apart from radiological test for lymph node, PET-CT to check distant metastasis is also essential. In fact, distant metastasis was found in one patient (5%).
Metastasized area was abdominal cavity which is difficult to diagnose by using only physical exam. Occurrence of metastasis affects the death rate of patients and possibility of complete recovery after the surgery. Due to such is- sues, PET-CT test is a necessary evaluation for Majolin's ulcer patients. MRI shows width and depth of Marjolin's ulcer and provides data to confirm the invasion into sur- rounding tissue, bone, vessel, and muscle. Especially for scalp, the invasion into the skull plays a key role to de- termine an operation plan13).
After evaluation, radical excision method for tumor
needs to be determined. Wide excision or amputation need to be determined while considering the possibility for recurrence and metastasis of cancer. In our case, our hospital had planned to perform lower extremity amputa- tion at pelvis level for one patient after the recurrence, but the procedure is on hold due to the lack of consent of the patient.
The decision of amputation is difficult for plastic sur- geons. It is also difficult to make a standard for amputa- tion while predicting prognosis. But we can consider be- low factors: When ulceration nature is accompanying dis- charge and ulcer has exophytic and resemble granulation tissue, size is bigger than 100 cm2, existence of multiple soft tissue invasion in surrounding area, existence of lym- phatics and vascular invasion, existence of lymph node and distant metastasis, rapid size increase after ulceration occurrence, and existence of scar tissue accompanied by the contracture surrounding the area of ulcer. Further re- search with more patients is required for recurrence and metastasis rate based on its size, depth, and nature, and consequently, a proper operational method needs to be determined.
If the patient is either in inoperable state, has lymph node or distant metastasis, or has serious soft tissue in- vasion, the patient should undergo chemotherapy and ra- diation therapy with the consultation of oncology special- ist8).
After the tumor resection of the different size, re- constructive surgery is needed. The size of ulceration does not equal the size of cancer. And based on the range and depth of invasion, the size of cancer could become bigger than the size of ulcer. Furthermore, if the con- tracture of surrounding tissue is present, the defect size after excision would become much bigger. It is better to perform excision and excisional release procedure simul- taneously to surrounding scar and contracture which have malignant transformation potential. Its consequence often demonstrates the bigger defect size than the size of cancer before the surgery (Fig. 7). And reconstructive op- eration after the removal of tumor is an important factor to decide the quality of life for the patient.
Also wide excision of Marjolin's ulcer conducts deeper resection compared to other forms of skin cancer and as a consequence, the defect is not just skin defect but skin
Fig. 7. (A) Scar contracture with Marjolin's ulcer, (B) Excisional release with wide excision. Defect size was lager than primary ulcera- tion.
and soft tissue defect with the shape of concave5). Skin graft was the most frequently used reconstructive surgery method, but flap coverage is better in terms of contour and texture. Also from an aesthetic aspect, movement fail- ure occurs due to contracture in the joint such as inguinal area and popliteal fossa with skin graft. So flap coverage is better than skin graft.
Free flap is a useful way to solve this problem. It main- tains mobility of the joints and aesthetic satisfaction when compared with skin graft. In our hospital, reconstruction surgery with free flap was performed in three patients.
Each patient's wound size were 30×25 cm, 10×5 cm and 15×10 cm. The locations of tumor were popliteal fossa and inguinal area. Unfortunately, one relapse, but the other two are showing good results in the range of mo- tion and aesthetic aspects. When Marjolin's ulcer was in the joint and size of ulcer was more than 100 cm2, free flap is recommended.
Marjolin's ulcer is a preventable complication of burns.
If medical professionals care primary wound with careful attention and educate patients thoroughly, then we can prevent serious prognosis which might lead to death1,5-7).
REFERENCES
1) Urszula O, Rafal M, Bartlomiej S, Jan K. Marjolin’s ulcer:
malignant neoplasm in scars. Radiother Oncol. 2006;11:
135-138.
2) Türegün M, Nişanci M, Güler M. Burn scar carcinoma with longer lag period arising in previously grafted area. Burns.
1997;23:496-497.
3) Gamatsi IE, McCulloch TA, Bailie FB, Srinivasan JR. Mali- gnant melanoma in a skin graft: burn scar neoplasm or a transferred melanoma? Br J Plast Surg. 2000;53:342-344.
4) Hatzis GP, Finn R. Marjolin's ulcer: a review of the literature and report of a unique patient treated with a CO(2) laser. J Oral Maxillofac Surg. 2007;65:2099-2105.
5) Chalya PL, Mabula JB, Rambau P, Mchembe MD, Kahima KJ, Chandika AB, et al. Marjolin's ulcers at a university teaching hospital in Northwestern Tanzania: a retrospective review of 56 cases. World J Surg Oncol. 2012;15:10-38.
6) Kowal-Vern A, Criswell BK, Sumner L. Burn scar neoplasms:
a literature review and statistical analysis. Burns. 2005;31:
403-413.
7) Chowdri NA, Darzi MA. Postburn scar carcinomas in Kash- miris. Burns. 1996;22:477-482.
8) Aydoğdu E, Yildirim S, Aköz T. Is surgery an effective and adequate treatment in advancement Marjolin’s ulcer? Burns.
2005;31:421-431.
9) Huang CY, Feng CH, Hsiao YC, Chuang SS, Yang JY. Burn scar carcinoma. J Dermatolog Treat. 2010;21:350-356.
10) Koga Y, Sawada Y. Basal cell carcinoma developing on a burn scar. Burns. 1997;23:75-77.
11) Yücel A, Yazar S, Demirkesen C, Durak H, Dervişoğlu S, Altintaş M. An unusual long-term complication of burn injury malignant fibrous histiocytoma developed in chronic burn scar. Burns. 2000;26:305-310.
12) Nishimoto S, Matsushita T, Matsumolo K, Adachi S. A rare case of burn scar malignancy. Burns. 1996;22:497-499.
13) Cavadas PC, Baena-Montilla P, Jordá-Cuevas J, Vera-Sempere FJ. Primary intracranial malignant tumor mistaken for a postburn scalp Marjolin’s ulcer. Burns. 1996;22:331-334.