대한소화기학회지 2004;44:93~98
서 론
1)만성 췌장염은 췌장 외분비선의 비가역적인 염증반응을 일으켜 내분비 및 외분비의 기능 부전을 일으키는 질환으 로 현재까지 염증을 직접 치료하거나 예방하는 방법이 알 려지지 않은 질환이다. 이러한 가장 큰 이유는 발병 기전에
접수: 2004년 4월 9일, 승인: 2004년 7월 12일 연락처: 류지곤, 110-744, 서울특별시 종로구 연건동 28
서울대학교병원 내과
Tel: (02) 760-1962, Fax: (02) 762-9662 E-mail: [email protected]
*본 연구는 서울대학교병원 연구비(04-2003-045-0) 보조를 받았음.
대해서 아직까지 잘 알지 못하기 때문으로 생각된다.2) 여러 발병 기전 중 가설로 췌장 내에서 트립신이 자가 활성화되어 췌장의 자가 소화와 췌장염이 생길 수 있는 데,1-3 이러한 가설을 뒷받침하는 임상적 질환으로 유전성 췌장염이 있다. 상염색체 우성으로 유전되는 유전성 췌장 염(hereditary pancreatitis) 환자에서 양이온 트립시노겐
Correspondence to: Ji Kon Ryu, M.D.
28 Yungun-dong, Jongno-gu, Seoul 110-744, Korea
Department of Internal Medicine, Seoul National University Hospital
Tel: +82-2-760-1962, Fax:+82-2-762-9662 E-mail: [email protected]
한국인 만성 췌장염 환자에서 SPINK1 및 PRSS1 유전자 변이
서울대학교 의과대학 내과학교실, 간연구소*
이광혁·윤원재·류지곤·김용태·윤용범·김정룡*
Mutations of SPINK1 and PRSS1 Gene in Korean Patients with Chronic Pancreatitis
Kwang Hyuck Lee, M.D., Won Jae Yoon, M.D., Ji Kon Ryu, M.D., Yong-Tae Kim, M.D., Yong Bum Yoon, M.D., and Chung Yong Kim, M.D.*
Departments of Internal Medicine, Liver Research Institute*, Seoul National University College of Medicine, Seoul, Korea
Background/Aims: It has been found that mutations of cationic trypsinogen gene (PRSS1) and serine protease inhibitor, Kazal type 1 gene (SPINK1) increase the susceptibility of chronic pancreatitis (CP). Specifically, mutations in the PRSS1 gene are related to the occurrences of hereditary and idiopathic pancreatitis while SPINK1 mutations are known to act as a disease modifier and are associated with idiopathic CP. However, the association of SPINK1 mutations with alcoholic CP is still controversial. We investigated the prevalence of PRSS1 and SPINK1 mutations in idiopathic and alcoholic CP in Korea. Methods: Seventy-one Korean patients with CP (alcoholic: 47, idiopathic: 22 and familial: 2) and 19 controls were included in this studies. Genomic DNA was extracted from peripheral blood of the patients. Mutations of SPINK1 (exon 3: N34S) and PRSS1 (exon 2: N29I, exon 3: R122H) genes were detected by PCR-RFLP methods. For the detection of SPINK1 mutation, restriction endonuclease PstI and BsrDI were used, while Sau3A and AflIII were used for the defection of PRSS1 mutation.
Results: Only one patient (2.1%) with alcoholic CP was a heterozygote for SPINK1 (N34S) mutation. Mutation in the PRSS1 (N29I, R122H) gene was not found in any group of CP patients. Additionally, we could not find any mutations of SPINK1 or PRSS1 in the control group. Conclusions: SPINK1 and PRSS1 mutations are not related to the development of CP in Korea. (Korean J Gastroenterol 2004;44:93-98)
Key Words: Cationic trypsinogen Gene; SPINK1 Gene; Pancreatitis, Chronic idiopathic; Pancreatitis, alcohol
대한소화기학회지: 제44권 제2호, 2004
(cationic trypsinogen 또는 serine protease 1, PRSS1) 유전자 변이로 생긴 돌연변이 트립시노겐이 췌장 내에서 조기 활 성화가 되어 췌장염을 일으킨다는 사실이 밝혀졌다.4-9가장 흔한 변이는 exon 2 N29I와 exon 3 R122H이며, 이외에도 10개 이상의 다른 부위에서도 변이가 나타난다.10-14 특발성 췌장염 환자에서 PRSS1의 변이는 0-19%의 빈도이다.15-21
췌장 내에서의 트립시노겐의 자가 활성화를 억제하여 췌장염 발생에 방어 기능을 하는 췌장 분비 트립신 억제 제(pancreatic secretory trypsin inhibitor, PSTI 또는 serine protease inhibitor, Kazal type 1, SPINK1)가 있다.3,18,19,22,23
서양에서는 SPINK1 유전자 변이 빈도가 특발성 만성 췌장 염 환자에서 높으며,19,22,24,25
열대성 췌장염에서도 그 빈도 가 상승된다.26 대표적인 변이로 exon 3 N34S 변이가 있 다.22,27
본 연구에서는 우리나라 만성 췌장염 환자에서 PRSS1 및 SPINK1 유전자 변이 중 가장 흔한 변이의 대표적인 빈 도를 조사하여 만성 췌장염에서 유발 인자로서의 가능성에 대해 조사하고자 하였다.
대상 및 방법
1. 대상
1998년 10월부터 2003년 8월까지 병원에 내원한 만성 췌장염 환자를 대상으로 하였으며, 대조군으로는 만성 췌 장염의 증거가 없는 사람을 대상으로 하였다. 만성 췌장염 의 진단기준은 반복적인 복통과 더불어 만성 췌장염의 방 사선검사 결과가 있거나, 지속적인 췌장 외분비 기능 장애 가 있는 경우로 하였다. 만성 췌장염 환자 중 알코올 섭취 가 적어도 5년 이상 하루 80 g 이상을 섭취한 경우를 알코 올 췌장염, 1대 또는 2대의 혈연관계를 가진 가족 중에서 췌장염이 있는 경우를 가족성 췌장염, 가족력이 없으며 특 별한 원인이 없는 경우를 특발성 췌장염으로 각각 정의하 였다. 특발성 췌장염 환자는 발병 시점의 나이를 기준으로
35세 이하를 조기 특발성 췌장염, 35세 이후를 후기 특발성 췌장염으로 각각 분류하였다.
2. 유전자 변이 검출 방법
1) DNA 추출 및 중합효소연쇄 반응(Polymerase chain reaction, PCR)
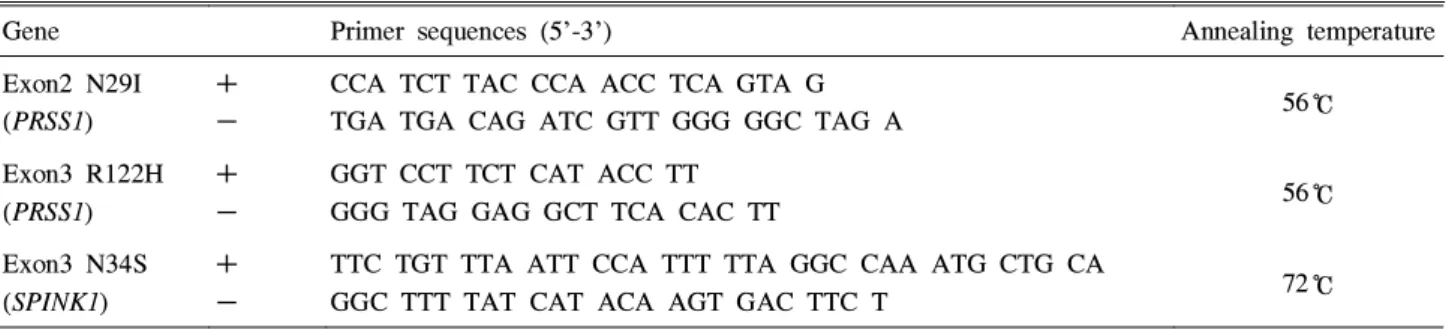
혈액을 원심분리하여 얻은 말초혈액 백혈구연층(buffy coat)에서 QIAmp DNA mini kit (Qiagen, California, USA) 를 이용하여 genomic DNA를 추출하였다. SPINK1 exon 3 N34S, PRSS1 exon 2 N29I 및 exon 3 R122H 변이 검출을 위한 PCR 시발체와 중합효소연쇄반응의 온도는 Table 1과 같다.24,28,29
중합효소연쇄반응은 10×PCR buffer, dNTP 100 µM, MgCl2 1.5 mM, 정방향과 역방항의 시발체 각 300 nM을 Taq polymerase (Perkin-Elmer, New Jersey, USA) 및 추출 한 DNA와 혼합하고 Perkin-Elmer GeneAmp PCR System 9600을 이용하여 시행하였다. SPINK1 exon 3 N34S 변이 검출에는 Taq polymerase 3 unit와 추출한 DNA 6 µL를 넣 고 총 반응량이 60 µL 되게 혼합하였으며, PRSS1 exon 2 N29I 및 exon 3 R122H 변이 검출에는 Taq polymerase 2 unit와 추출한 DNA 4 µL를 넣고 총 반응량이 40 µL 되게 혼합하였다.
2) 제한효소 절편 길이 다형성(Restriction enzyme fragment length polymorphism, RFLP) 및 전기 영동 SPINK1 exon 3 N34S 변이 검출을 위한 최초 PCR 생산 물은 320 bp인데 야생형 산물은 BsrDI 제한효소(New England Biolabs, Beverly, USA)에 의해서 286 bp로, 변이 가 있는 산물은 PstI 제한효소(New England Biolabs)에 의 해서 286 bp로 분쇄됨을 이용하여 genomic DNA의 SPINK1 변이 유무를 검출하였다.24 제한효소 반응은 PCR 산물 25 µL에 10 units 제한효소, 1×digest buffer (New England Biolabs), 1×BSA (New England Biolabs)를 넣고 최종 부피 50 µL가 되게 만들었다. PstI 제한효소는 37℃에
Table 1. PCR Primers and Annealing Temperature used for the Detection of Cationic Trypsinogen (PRSS1) and Serine Protease Inhibitor, Kazal Type 1 (SPINK1) Mutations
Gene Primer sequences (5'-3') Annealing temperature Exon2 N29I
(PRSS1)
+
-
CCA TCT TAC CCA ACC TCA GTA G
TGA TGA CAG ATC GTT GGG GGC TAG A 56℃
Exon3 R122H (PRSS1)
+
-
GGT CCT TCT CAT ACC TT
GGG TAG GAG GCT TCA CAC TT 56℃
Exon3 N34S (SPINK1)
+
-
TTC TGT TTA ATT CCA TTT TTA GGC CAA ATG CTG CA
GGC TTT TAT CAT ACA AGT GAC TTC T 72℃
94
이광혁 외 5인. 한국인 만성 췌장염 환자에서 SPINK1 및 PRSS 1 유전자 변이
서 1시간 반응시키고, BsrDI 제한효소는 55℃에서 1시간 반응시킨 후 두 경우 모두 80℃에서 15분 잠복하여 불활성 화시켰다.
PRSS1 exon 3 R122H 변이가 있는 경우에는 AflIII 제한 효소(New England Biolabs)에 의해서 911 bp의 PCR 산물 이 565 bp와 346 bp로 분쇄되고,3 PRSS1 exon 2 N29I 변이 가 있는 경우에는 Sau3A 제한효소(New England Biolabs)에 의해서 분쇄됨을 이용하여 변이 유무를 검출하였다.28,29 두 경우 모두 제한효소 반응은 PCR 산물 25 µL에 10 units 제 한효소, 1×digest buffer (New England Biolabs), 1×BSA (New England Biolabs)를 넣고 최종 부피 50 µL가 되게 만 들어서 37℃에서 1시간 반응을 시켰다. 반응을 불활성화시 키기 위하여 AflIII 제한효소는 80℃에서 20분, Sau3A 제한 효소는 65℃에서 20분 간 잠복시켰다.
최종 산물은 0.5 µg/mL ethium bromide를 포함한 agarose gel에서 전기 영동한 후 분석하였다. SPINK1 변이의 경우 에는 3% agarose gel을 사용하였으며, PRSS1 변이의 경우 에는 2% agarose gel을 사용하였다.
결 과
1. 대상 환자
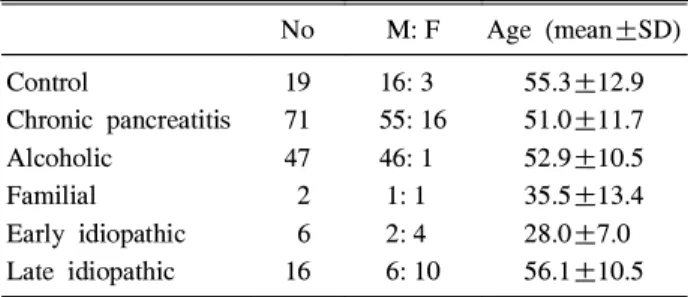
만성 췌장염 환자는 총 71명(남자 55명, 여자 16명)으로 평균 연령은 51.0세이었고 대조군은 19명(남자 16명, 여자 3명)으로 평균 연령은 55.3세였다. 만성 췌장염 환자를 원 인에 따라서 분류하면, 알코올 췌장염 환자는 47명, 가족성 췌장염 환자는 2명, 조기 특발성 췌장염 환자는 6명, 후기 특발성 췌장염 환자는 16명이었다. 각 환자군에서 남녀 비 및 평균 연령은 Table 2와 같다.
2. 변이 검출 결과
PRSS1 exon 3 R122H 변이 및 exon2 N29I 변이 검출을 위해서 PCR-RFLP 시행하였을 때, 환자군 및 대조군 모두
에서 검출되지 않았다. SPINK1 N34S 변이에 대해서 검사 를 실시한 결과는 알코올 췌장염 환자 47명 중 1명(2.1%)에 서만 이종형이 관찰되었고, 나머지 환자군 및 대조군에서 는 SPINK1 유전자 변이가 검출되지 않았다(Fig. 1).
고 찰
만성 췌장염 환자에서 질병과 관계가 있는 유전자들에 대한 연구가 있었는데 이 중 PRSS1, SPINK1 및 cystic fibrosis transmembrane conductance regulator (CFTR)의 유 전자 변이가 대표적으로 알려져 있다. 이러한 유전자 변이 에 대한 연구가 서양에서는 비교적 활발하게 진행되어 왔 으나, 국내에서는 11명의 특발성 췌장염 환자에서 PRSS1 변이를 찾기 위한 염기서열 분석이 행해진 연구와 25명의 만성 췌장염 환자와 47명의 기관지확장증 환자를 대상으로 CFTR 유전자 변이에 대한 연구가 있다.30,31 본 연구에서는 만성 췌장염 환자를 대상으로 PCR-RFLP의 방법으로 SPINK1 및 PRSS1 유전자 변이를 발견하고자 했다.
상염색체 우성으로 유전되는 유전성 췌장염의 경우 약 80%의 질병 표현율(disease penetrance rate)을 가진다.32 PRSS1 유전자의 여러 부위에서 변이가 나타나는데, 122번 째 염기서열의 arginine (CGC)이 histidine (CAC)으로 변하 는 exon 3의 R122H 변이와 29번째 염기서열의 asparagine (AAC)이 isoleucine (ATC)으로 변하는 exon 2의 N29I 변이 가 가장 흔하다.3,10,33-36 이외에도 빈도는 드물지만 A16V,37 K23R, -28delTCC38등의 변이가 발견된다. 최근에는 D22G, P36R, E79K, G83E, K92N, V123M, L104P, R116C, C139F, R122C, N29T 등의 변이도 보고되었다.39-41
PRSS1 유전자의 변이는 특발성 췌장염 환자에서도 나타
Table 2. Age and Sex Ratio in Controls and Patients according to Subtypes of Chronic Pancreatitis
No M: F Age (mean±SD) Control
Chronic pancreatitis Alcoholic
Familial Early idiopathic Late idiopathic
19 71 47 2 6 16
16: 3 55: 16 46: 1
1: 1 2: 4 6: 10
55.3±12.9 51.0±11.7 52.9±10.5 35.5±13.4 28.0±7.0 56.1±10.5 SD, standard deviation.
Fig. 1. SPINK1*and PRSS1†polymerase chain reaction-restriction fragment length polymorphism analysis. (A) Gel electrophoresis of BsrDI (a) and PstI (b) digestion for SPINK1 exon 3 N34S is shown. Lane 7 shows the result of heterozygote and the others those of wild types. (B) Gel electrophoresis of PCR product (a) and AflIII digestion (b) for PRSS1 exon 3 R122H is shown. (C) Gel electrophoresis of PCR product (a) and Sau3A digestion (b) for PRSS1 exon 2 N29I is shown. No PRSS1 mutation is detected.
Lane 1-2 are from controls, lane 3 is from a patient with idiopathic chronic pancreatitis, lane 4 is from a patient with familial pancreatitis, and lane 5-8 are from patients with alcoholic chronic pancreatitis.
*SPINK1, serine proteare inhibitor, Kazal type I gene.
†PRSS1, cationic trypsinogen gene.
95
The Korean Journal of Gastroenterology: Vol. 44, No. 2, 2004
날 수 있는데 연구 대상 집단에 따라서 0%에서 19%까지 다양하다.5-21,37,39,40,42
우리나라에서 시행된 11명의 특발성 췌장염 환자의 염기서열 분석에서는 PRSS1의 변이가 발견 되지 않았다.30본 연구에서도 특발성 및 가족성 췌장염 환 자에서 PRSS1 변이는 발견되지 않았다.
SPINK1은 56개의 아미노산으로 구성되어 있으며, 그 기 능은 트립시노겐 조기 활성화로 분리된 트립신과 결합하여 자가 소화를 억제한다.3,19,22,23 이 단백질에 결손 유전자 변 이가 일어나면 SPINK1과 트립신의 결합이 원활하게 이루 어지지 않아서 췌장염 유발을 촉진한다.19,22,27 이러한 대표 적인 결손 유전자 변이로 SPINK1 exon 3의 N34S와 P55S 변이가 있다. 원인 불명의 만성 췌장염 환자에서 이러한 유 전자 변이의 빈도는 25%까지 보고되며,19,22 특발성 췌장염 환자에서 SPINK1 유전자 변이 빈도가 높은 지역의 경우 정 상인에게서도 SPINK1 유전자 변이는 2%까지 나타난다.22,27 특발성 췌장염이 16,000명당 한 명 꼴로 발생하는 드문 질 환임을 고려하면, SPINK1의 변이는 직접적인 병의 원인이 기보다는 췌장염 발생 역치를 낮추는 질병 교란자(disease modifier)로서의 역할을 할 것으로 추정된다. 개인에 따라서 췌장염을 일으키는 알코올의 양이 다른 것으로 알려진 알 코올 췌장염 환자에서 SPINK1의 유전자 변이가 정상인보 다 높게 나타나서 알코올 췌장염에서도 질병 교란자의 역 할을 한다고 하지만,24,43,44 최근 이탈리아에서의 연구에 의 하면 SPINK1 유전자 변이 빈도가 알코올 췌장염 환자와 알 코올 간질환 환자 사이에서 별 차이가 없다는 보고도 있 어,45 알코올 췌장염에서 SPINK1의 역할은 아직 정립되지 않은 실정이다.
국내에서는 아직까지 SPINK1 유전자 변이에 대한 연구 가 없었다. 본 연구에서는 SPINK1 N34S 변이 빈도를 특발 성, 알코올 및 가족성 만성 췌장염 환자에서 검사했는데, 알코올 췌장염 환자 1명에게서만 이종형(heterozygote)으로 발견되었고 다른 환자 및 대조군에서는 변이가 없었다.
PRSS1 및 SPINK1 유전자 변이가 서구와 달리 본 연구에 서는 거의 검출되지 않았다. 그 이유를 분석하면 첫째, 유 전자 변이를 찾기 위해서 사용한 방법이 PRSS1 exon 3 R122H 및 exon 2 N29I와 SPINK1 exon 3 N34S만 검출할 수 있는 PCR-RFLP 방법을 사용하였기 때문에 다른 exon 부위의 변이가 췌장염 발생에 기여하여 위음성으로 나왔을 가능성이 있다. 그러나 본 연구에서 찾고자 한 유전자 변이 부위가 가장 흔한 부위이고, 조사한 환자 수가 71명으로 충 분하였기에 위음성의 가능성은 떨어진다. 둘째는 인종적 및 민족적 차이로 실제로 국내에는 이러한 유전적 변이가 적을 가능성이 있다. 본 연구에서는 가족력이 있는 췌장염 환자가 2명 포함되어 있는데 이들 모두에게서 PRSS1 및 SPINK1 유전자 변이가 검출되지 않았고, 현재까지 우리나
라에서는 PRSS1 변이를 동반한 유전성 췌장염 환자가 보 고된 바 없다. 이러한 점도 서양과는 다른 유전적 차이가 있을 것을 시사한다. 유전성 췌장염에 대한 결론을 얻기 위 해서는 전국적으로 가족력이 있는 췌장염 환자를 모아서 정확한 가계도 조사와 PRSS1 유전자 변이를 조사해야 할 것이다. 다른 대표적인 CFTR 변이의 경우 최근까지도 국 내에서는 없는 것으로 알려져 있었으나, 최근 대조군 117 명과 만성 췌장염이나 기관지확장증을 가진 환자군 75명 을 대상으로 한 연구에서 외국의 보고와는 달리 M470V- Q1352H, IVS8T5-M470V와 E217G 변이가 높은 빈도로 나 타나며 이러한 변이가 CFTR 의존성 음이온 전달에 이상을 미친다는 사실이 밝혀졌다.31 앞으로 췌장염 환자의 유전적 소인에 대한 연구로 최근에 새로 밝혀진 위치의 CFTR 유 전자의 변이에 대한 빈도의 조사가 필요할 것으로 생각된 다.
외국의 보고와는 달리 국내의 특발성 및 알코올 만성 췌 장염 환자에서 SPINK1 및 PRSS1 유전자 변이의 빈도가 높 지 않았고, 대조군에서도 SPINK1 유전자 변이가 발견되지 않았다. 이 연구에서는 SPINK1 및 PRSS1 유전자 변이와 만성 췌장염과의 연관성을 밝히지 못하였다.
요 약
목적: 만성 췌장염 환자에서 질병을 일으키는 유전자로 양이온 트립시노겐(cationic trypsinogen 또는 serine protease 1, PRSS1) 유전자 변이와 췌장 분비 트립신 억제 제(serine protease inhibitor, Kazal type 1, SPINK1) 유전자 변이가 있다. 서양에서의 연구 결과, PRSS1 유전자 변이는 유전성 및 특발성 췌장염과 관련이 있고 SPINK1의 경우에 는 특발성 췌장염과의 관련이 있는 것으로 알려져 있다. 가 장 흔한 알코올 만성 췌장염과 SPINK1과의 연관성에 대해 서는 아직까지 논란이 있는 실정이다. 본 연구에서는 우리 나라 만성 췌장염 환자에서 PRSS1 및 SPINK1 유전자 변이 빈도를 조사하여 알코올 및 특발성 만성 췌장염에서 유발 인자로서의 가능성에 대해 조사하고자 하였다. 대상 및 방 법: 71명의 만성 췌장염 환자(알코올 췌장염: 47명, 특발성 췌장염: 22명, 가족성 췌장염: 2명) 및 19명의 대조군을 연 구 대상으로 하였다. 혈액에서 추출한 genomic DNA에서 SPINK1 및 PRSS1 유전자 변이를 PCR-RFLP 방법을 이용 하여 검사하였다. Pst I와 BsrDI 제한효소는 SPINK1 exon 3 N34S 유전자 변이 검출에 사용되었고, Sau3A 제한효소 및 AflIII 제한효소는 각각 PRSS1 exon 2 N29I 및 PRSS1 exon 3 R122H의 변이 검출에 사용하였다. 결과: SPINK1 유전자 변이는 알코올 만성 췌장염 환자 중 한 명(2.1%)에서 이종 형(heterozygote)으로 검출되었고 PRSS1 유전자 변이는 한 96
Lee KH, et al. Mutations of SPINK1 and PRSS 1 Gene in Korean Patients with Chronic Pancreatitis
명도 검출되지 않았다. 대조군에서도 SPINK1 및 PRSS1 유 전자 변이가 검출되지 않았다. 결론: 외국의 보고와는 달리 국내의 만성 췌장염 환자에서는 SPINK1 및 PRSS1 유전자 변이는 유발 인자로서의 역할이 적을 것으로 추정된다.
색인단어: Cationic trypsinogen 유전자, SPINK1 유전자, 만 성 특발성 췌장염, 알코올 췌장염
참고문헌
1. Hofbauer B, Saluja AK, Lerch MM, et al. Intra-acinar cell activation of trypsinogen during caerulein-induced pancreatitis in rats. Am J Physiol 1998;275:G352-G362.
2. Kruger B, Lerch MM, Tessenow W. Direct detection of premature protease activation in living pancreatic acinar cells. Lab Invest 1998;78:763-764.
3. Whitcomb DC, Gorry MC, Preston RA, et al. Hereditary pancreatitis is caused by a mutation in the cationic trypsi- nogen gene. Nat Genet 1996;14:141-145.
4. Sahin-Toth M, Graf L, Toth M. Trypsinogen stabilization by mutation Arg117-->His: a unifying pathomechanism for hereditary pancreatitis? Biochem Biophys Res Commun 1999;264:505-508.
5. Sahin-Toth M, Toth M. Gain-of-function mutations associated with hereditary pancreatitis enhance auto- activation of human cationic trypsinogen. Biochem Biophys Res Commun 2000;278:286-289.
6. Whitcomb DC. Hereditary pancreatitis: new insights into acute and chronic pancreatitis. Gut 1999;45:317-322.
7. Teich N, Ockenga J, Hoffmeister A, Manns M, Mossner J, Keim V. Chronic pancreatitis associated with an activation peptide mutation that facilitates trypsin activation. Gastro- enterology 2000;119:461-465.
8. Chen JM, Montier T, Ferec C. Molecular pathology and evolutionary and physiological implications of pancreatitis- associated cationic trypsinogen mutations. Hum Genet 2001;109:245-252.
9. Naruse S, Kitagawa M, Ishiguro H. Molecular under- standing of chronic pancreatitis: a perspective on the future.
Mol Med Today 1999;5:493-499.
10. O'Reilly DA, Kingsnorth AN. Hereditary pancreatitis and mutations of the cationic trypsinogen gene. Br J Surg 2000;87:708-717.
11. Teich N, Ockenga J, Keim V, Mossner J. Genetic risk factors in chronic pancreatitis. J Gastroenterol 2002;37:1-9.
12. Witt H, Becker M. Genetics of chronic pancreatitis. JPGN J Padiatr Gastroenterol Nutr 2002;34:125-136.
13. Chen JM, Ferec C. Gene conversion-like missense mutations in the human cationic trypsinogen gene and insights into the molecular evolution of the human trypsinogen family. Mol Genet Metab 2000;71:463-469.
14. Jansen JB, te Morsche R, van Goor H, Drenth JP. Genetic basis of chronic pancreatitis. Scand J Gastroenterol 2002;
236(suppl):91S-94S.
15. Ockenga J, Stuhrmann M, Ballmann M, et al. Mutations of the cystic fibrosis gene, but not cationic trypsinogen gene, are associated with recurrent or chronic idiopathic pan- creatitis. Am J Gastroenterol 2000;95:2061-2067.
16. Teich N, Hoffmeister A, Keim V. Mutations of cationic trypsinogen in chronic pancreatitis. Lancet 1999;354:1302.
17. Creighton J, Lyall R, Wilson DI, Curtis A, Charnley R.
Mutations of the cationic trypsinogen gene in patients with chronic pancreatitis. Lancet 1999;354:42-43.
18. Audrezet MP, Chen JM, Le Marechal C, et al. Determi- nation of the relative contribution of three genes-the cystic fibrosis transmembrane conductance regulator gene, the cationic trypsinogen gene, and the pancreatic secretory trypsin inhibitor gene to the etiology of idiopathic chronic pancreatitis. Eur J Hum Genet 2002;10:100-106.
19. Witt H, Luck W, Hennies HC, et al. Mutations in the gene encoding the serine protease inhibitor, Kazal type 1 are associated with chronic pancreatitis. Nat Genet 2000;25:
213-216.
20. Pfutzer RH, Whitcomb DC. Trypsinogen mutations in chronic pancreatitis. Gastroenterology 1999;117:1507-1508.
21. Truninger K, Kock J, Wirth HP, et al. Trypsinogen gene mutations in patients with chronic or recurrent acute pancreatitis. Pancreas 2001;22:18-23.
22. Pfutzer RH, Barmada MM, Brunskill AP, et al. SPINK1/
PSTI polymorphisms act as disease modifiers in familial and idiopathic chronic pancreatitis. Gastroenterology 2000;
119:615-623.
23. Rinderknecht H, Adham NF, Renner IG, Carmack C. A possible zymogen self-destruct mechanism preventing pancreatic autodigestion. Int J Pancreatol 1988;3:33-44.
24. Threadgold J, Greenhalf W, Ellis I, et al. The N34S mutation of SPINK1 (PSTI) is associated with a familial pattern of idiopathic chronic pancreatitis but does not cause the disease. Gut 2002;50:675-681.
25. Drenth JP, te Morsche R, Jansen JB. Mutations in serine protease inhibitor Kazal type 1 are strongly associated with chronic pancreatitis. Gut 2002;50:687-692.
26. Chandak GR, Idris MM, Reddy DN, Bhaskar S, Sriram PV, Singh L. Mutations in the pancreatic secretory trypsin 97
대한소화기학회지: 제44권 제2호, 2004
inhibitor gene (PSTI/SPINK1) rather than the cationic trypsinogen gene (PRSS1) are significantly associated with tropical calcific pancreatitis. J Med Genet 2002;39:347-351.
27. Chen JM, Mercier B, Audrezet MP, Ferec C. Mutational analysis of the human pancreatic secretory trypsin inhibitor (PSTI) gene in hereditary and sporadic chronic pancreatitis.
J Med Genet 2000;37:67-69.
28. O'Reilly DA, Yang BM, Creighton JE, Demaine AG, Kingsnorth AN. Mutations of the cationic trypsinogen gene in hereditary and non-hereditary pancreatitis. Digestion 2001;64:54-60.
29. Howes N, Greenhalf W, Rutherford S, et al. A new polymorphism for the R122H mutation in hereditary pan- creatitis. Gut 2001;48:247-250.
30. Lee WJ, Kim KA, Lee JS, et al. Cationic trypsinogen gene mutation in patients with chronic idiopathic pancreatitis.
Korean J Gastroenterol 2004;43:41-46.
31. Lee JH, Choi JH, Namkung W, et al. A haplotype-based molecular analysis of CFTR mutations associated with respiratory and pancreatic diseases. Hum Mol Genet 2003;
12:2321-2332.
32. Comfort MW, Steinberg AG. Pedigree of a family with hereditary chronic relapsing pancreatitis. Gastroenterology 1952;21:54-63.
33. Gorry MC, Gabbaizedeh D, Furey W, et al. Mutations in the cationic trypsinogen gene are associated with recurrent acute and chronic pancreatitis. Gastroenterology 1997;113:
1063-1068.
34. Teich N, Mossner J, Keim V. Mutations of the cationic trypsinogen in hereditary pancreatitis. Hum Mutat 1998;
12:39-43.
35. Bell SM, Bennett C, Markham AF, Lench NJ. Evidence for a common mutation in hereditary pancreatitis. Mol Pathol 1998;51:115-117.
36. Tautermann G, Ruebsamen H, Beck M, Dertinger S, Drexel H, Lohse P. R116C mutation of cationic trypsinogen in a Turkish family with recurrent pancreatitis illustrates genetic microheterogeneity of hereditary pancreatitis. Digestion 2001;64:226-232.
37. Witt H, Luck W, Becker M. A signal peptide cleavage site mutation in the cationic trypsinogen gene is strongly associated with chronic pancreatitis. Gastroenterology 1999;
117:7-10.
38. Ferec C, Raguenes O, Salomon R, et al. Mutations in the cationic trypsinogen gene and evidence for genetic heterogeneity in hereditary pancreatitis. J Med Genet 1999;
36:228-232.
39. Teich N, Bauer N, Mossner J, Keim V. Mutational screening of patients with nonalcoholic chronic pancreatitis:
identification of further trypsinogen variants. Am J Gastro- enterol 2002;97:341-346.
40. Chen JM, Piepoli Bis A, Le Bodic L, et al. Mutational screening of the cationic trypsinogen gene in a large cohort of subjects with idiopathic chronic pancreatitis. Clin Genet 2001;59:189-193.
41. Pfutzer R, Myers E, Applebaum-Shapiro S, et al. Novel cationic trypsinogen (PRSS1) N29T and R122C mutations cause autosomal dominant hereditary pancreatitis. Gut 2002;50:271-272.
42. Nishimori I, Kamakura M, Fujikawa-Adachi K, et al.
Mutations in exons 2 and 3 of the cationic trypsinogen gene in Japanese families with hereditary pancreatitis. Gut 1999;44:259-263.
43. Witt H, Luck W, Becker M, et al. Mutation in the SPINK1 trypsin inhibitor gene, alcohol use, and chronic pancreatitis.
JAMA 2001;285:2716-2717.
44. Schneider A, Pfützer RH, Barmada MM, et al. Limited contribution of the SPINK1 N34S mutation to the risk and severity of alcoholic chronic pancreatitis: a report from the United States. Dig Dis Sci 2003;48: 1110-1115.
45. Perri F, Piepoli A, Stanziale P, Merla A, Zelante L, Andriulli A. Mutation analysis of the cystic fibrosis transmembrane conductance regulator (CFTR) gene, the cationic trypsinogen (PRSS1) gene, and the serine protease inhibitor, Kazal type 1 (SPINK1) gene in patients with alcoholic chronic pancreatitis. Eur J Hum Genet 2003;11:
687-692.
98