Clavicle Nonunion: Matchstick Bone-grafting and Osteosynthesis
Yong Bok Park*, Jae Chul Yoo1,*, Geun Min Park1, Dong Ho Kum1, Mohammed Tauheed1, Jeung Yeol Jeong1
Department of Orthopaedic Surgery, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, 1Department of Orthopaedic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Background: This study was conducted to evaluate the surgical outcomes of plate fixation using autologous iliac bone graft shaped in the form of a matchstick in clavicle nonunion resulting from prior surgical or non-surgical management.
Methods: From May 2005 to February 2013, 17 patients underwent surgery for clavicle nonunion. The mean age at the time of sur- gery was 48.8 years. The iliac bone was harvested and shaped into slivers approximately 3 cm long, which resembled matchsticks. After opening of the medullary canal, the plate and screws were applied and cancellous bone was placed at the nonunion site. Matchstick bone grafts which were longitudinally placed and encircled on the nonunion site were tied with periosteum using 3–4 stitches. Union was determined via postoperative plane X-ray. Clinical status was evaluated using the visual analogue scale score for pain, and Constant and American Shoulder Elbow Surgeon score.
Results: All patients had a stable radiological union at the follow-up. The mean duration from index operation to nonunion operation was 13.2 months (7–32 months). The mean follow-up period was 20.1 months (8–56 months), and the mean duration until union was 11.2 weeks (8–16 weeks). All clinical scores were improved at the final follow-up (p<0.001). The mean segmental defect was 3.3 ± 2.6 mm (1–18 mm); and the difference in clavicular length between operative and non-operative site was 5.9 ± 6.9 mm.
Conclusions: Matchstick shaped autologous iliac bone grafting technique in clavicle nonunion is acceptable with a high union rate.
(Clin Shoulder Elbow 2016;19(1):33-38)
Key Words: Nonunion; Bone graft; Clavicle; Matchstick
Copyright © 2016 Korean Shoulder and Elbow Society. All Rights Reserved. pISSN 2383-8337
Clinics in Shoulder and Elbow Vol. 19, No. 1, March, 2016 http://dx.doi.org/10.5397/cise.2016.19.1.33
Received January 14, 2016. Revised January 26, 2016. Accepted January 28, 2016.
*These authors contributed equally to this paper as co-first authors.
Correspondence to: Jeung Yeol Jeong
Department of Orthopaedic Surgery, Samsung Medical Center, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea Tel: +82-2-3410-3501, Fax: +82-2-3410-0061, E-mail: [email protected]
Financial support: None. Conflict of interests: None.
Introduction
Clavicle fractures are common injuries accounting for 5% to 10% of all fractures.1) A large meta-analysis study reported the in- cidence of clavicle nonunion as 5.9% for undisplaced, to 15.1%
for displaced fractures.2) However, the incidence of nonunion is variable according to different studies.
In non-surgically managed clavicle fractures, displacement and comminution of fractures, female gender, advancing age,3) and >2 cm shortening4) have been reported as the cause of clavicle nonunion. Even though the fractures were treated surgi- cally, improper choice of implant or failure of fixation can result in nonunion.5,6)
Various implants including intramedullary fixation with the
Steinmann pin,7) Hagie pin,8) Rush pins,9) Kirschner wires,10) external fixators,11) plate and screws,12) and screws alone13) are used in the treatment of clavicle nonunion. Some authors have advocated vascularized bone graft reconstruction14) or osteosyn- thesis with pectoralis major muscle augmentation in recurrent nonunion.15) However, the definitive management is still contro- versial.
Numerous studies have reported open reduction and internal fixation with autologous bone grafting as an acceptable tech- nique to regain the necessary clavicle length in the treatment of clavicle nonunion in cases with atrophied fracture ends and or shortening of the fracture site.16-18) However, we sometimes feel that the conventional method should not be used in cases with failed atrophic nonunion surgery using conventional cancellous
chip bone graft technique.
The purpose of this study was to evaluate the surgical out- comes of plate fixation using autologous iliac bone graft shaped in the form of a matchstick in clavicle nonunion previously treat- ed with non-surgical or surgical management including failed nonunion surgery.
The hypothesis was that the healing rate would be as good as that of previous reports.
Methods
Patient Demographics
This study was a retrospective review of 17 operations for atrophic clavicle nonunion between May 2005 and Febru- ary 2013 by 1 surgeon at a single institution. Indications were patients with no evidence of radiological union, persistence of pain, cosmetic deformity, dysfunction or gross movement at the fracture site even after 16 weeks,19) but usually more than 2 years of conservative treatment or in cases of primary fixa- tion failure. Exclusion criteria included patients with an active infection at the nonunion site at the time of surgery, nonunion following a pathological fracture or through previously irradiated bone, previous history of clavicle fracture, or callus formation of
the nonunion site (hypertrophic). Institutional Review Board ap- proval was obtained before data collection.
Of the 17 patients, 13 were male and 4 were female with a mean age of 48.8 years at the time of surgery. The right clavicle was involved in 6 cases and the left clavicle in 11 cases. Nine patients sustained fracture following a fall; 4 from a road traffic accident; 2 from sports injury; and 2 from falling off a bicycle.
The clavicle fractures were classified according to the Edinburg classification.1)
In total 17 cases of nonunion, 10 cases received primar- ily non-surgical treatment. In 10 cases of nonunion with non- surgical treatment, 7 cases were type IIB1 (displaced mid-3/5th shaft fracture with or without a single fragment), 2 cases were type IIB2 (displaced mid-3/5th shaft fracture with multi-fragment or segmental), and 1 case was IIIB1 (displaced extra articular lateral end fracture). In 17 cases of nonunion, 7 cases resulted in nonunion after surgical treatment. Among these, 5 cases were nonunion with hardware failure including plate breakage, and 2 with an intact plate. Of the 5 cases of hardware failure, 3 had cerclage wires that were inserted as a primary procedure for a comminuted fracture at a different institution and 2 were fixed with a plate and lag screws for fragment fixation; 1 of these patients presented to us with 3 failed operations performed else-
Table 1. Detailed Demographic Data of the Patients Who Had Open Reduction and Internal Fixation with Autologous Iliac Bone Graft Shaped in the Form of a Matchstick in Clavicle Nonunion
Patient No. Sex Age (yr) Site Duration from injury
to surgery (wk) Cause of injury Prior management Classifi cation*
1 M 65 Lt 16 Soccer Conservative IIB1
2 M 53 Lt 28 Slip and fall Conservative IIB2
3 F 58 Lt 17 Traffi c accident Conservative IIB2
4 M 38 Lt 48 Fall down Operative II†,‡
5 M 57 Lt 20 Traffi c accident Conservative IIB1
6 M 34 Lt 29 Fall down Operative II†,‡
7 F 36 Rt 62 Traffi c accident Operative II†,§
8 M 62 Rt 20 Fall down Conservative IIB1
9 M 60 Lt 36 Fall down Conservative IIB1
10 F 62 Rt 41 Bicycle Conservative IIB1
11 M 57 Rt 80 Slip and fall Conservative IIB1
12 M 42 Lt 20 Traffi c accident Operative II†,§
13 M 47 Rt 56 Bicycle Operative II†,‡
14 M 32 Lt 27 Snow board Operative II†,‡
15 F 51 Rt 43 Fall down Operative II†,‡
16 M 24 Lt 52 Fall down Conservative IIB1
17 M 52 Lt 54 Fall down Conservative IIIB1
M: male, F: female, Lt: left , Rt: Right.
*According to Edinburg classifi cation of clavicle fracture. †Detailed classifi cation of the fracture was impossible because of prior surgery performed at other insti- tutions. ‡Nonunion with hardware failure. §Nonunion with hardware in situ.
where for treatment of the nonunion. The mean duration from the onset of fracture to surgery for nonunion was 38.2 weeks (range, 16–80 weeks). All patients were symptomatic with pain, restricted mobility, weakness, or cosmetic deformity. Plain X-ray showed 17 cases as atrophic nonunion. The mean follow-up duration was 20.1 months (range, 8–56 months). The patients’
demography is described in Table 1.
Surgical Procedure
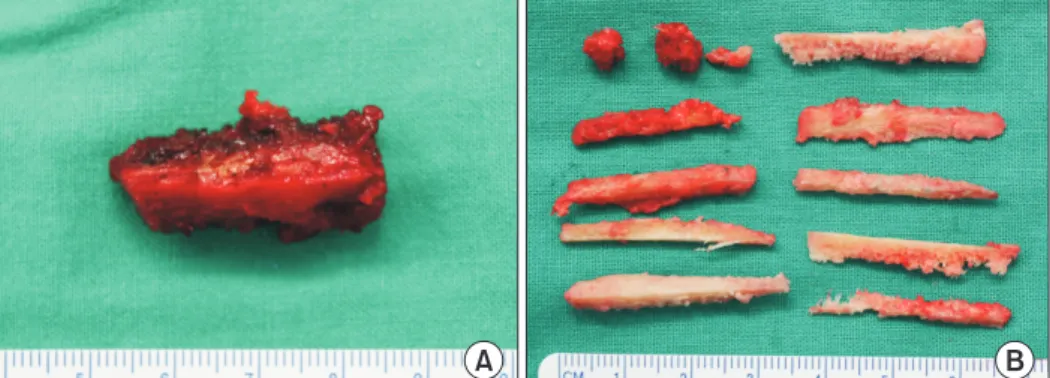
All operations were performed under general anesthesia in the beach-chair position. The corticocancellous bone graft was typically harvested from the ipsilateral iliac crest and shaped into slivers approximately 3 cm long that resembled matchsticks (Fig. 1). A skin incision was made over the superior surface along the longitudinal axis of the clavicle. Careful sub-periosteal dissec- tion was performed and the nonunion site was approached, the fibrous tissue was excised along with the sclerotic bone ends and the medullary canals of both fragments were opened using a 3.5 mm drill bit (Fig. 2). The debrided fracture ends were reduced, and the plate was applied with screws of at least 3 cortices. A 3.5 mm reconstruction plate (reconstruction plate; AO Syn- thes, Paoli, PA, USA) was used in 8 cases, a 3.5 mm anatomical
plate (locking compression plate [LCP]; AO Synthes) in 8 cases (including 1 case of type IIIB1), and a 3.5 mm anatomical plate (LCP; Acumed, Hillsboro, OR, USA) in 1 case. After applica- tion of the plate and screws, cancellous bone was placed at the nonunion site. Using Ethibond no. 5, 3, or 4 stiches purchasing periosteum were passed around the nonunion site, and then the Fig. 2. Th e medullary canals of both fragments were opened with a 3.5 mm
drill bit.
Fig. 4. Th e sutures are tied with periosteum, fi rmly opposing the bone graft to the nonunion site.
Fig. 3. Using Ethibond no. 5, 3, or 4 stiches purchasing periosteum were passed around the fracture ends with the plate, and then the individual sticks of bone graft were longitudinally placed encircling nonunion site.
A B
Fig. 1. (A) The corticocancellous bone was typically harvested from the ipsilateral iliac crest. (B) The harvested bone stock was shaped into slivers of about 3–4 cm long re- sembling matchsticks.
individual sticks of bone graft were placed encircling the non- union site (Fig. 3). The sutures were tied with periosteum, firmly opposing the bone graft to the nonunion site (Fig. 4). Remaining cancellous bone was also placed at the nonunion site and the soft tissue and skin were closed in layers. An arm sling was used for immobilization for 2 to 4 weeks.
Clinical and Radiological Evaluation
Patients were evaluated in the outpatient clinic at regular intervals using the visual analogue scale score for pain (pVAS), American Shoulder and Elbow Surgeon (ASES) score,20) and Constant-Murley shoulder scoring system.21) Union was defined as disappearance of the fracture line, continuity of the bony cortices and remodeling on 2 plain X-ray views (Anteroposterior and 15 degree cephalic tilt view). Fracture gap between both fracture ends was measured, and clavicular length was com- pared with the non-operative site.
Statistical Analysis
Preoperative and postoperative clinical scores (pVAS, ASES, Constant scores) were compared by t-test or Wilcoxon signed rank test. Statistical analyses were performed by IBM SPSS sta- tistics ver. 20.0 (IBM Co., Armonk, NY, USA) and a confidence interval of 95% was used throughout.
Results
The mean follow-up period was 20.1 months (range, 8–56 months). The mean pVAS was significantly decreased from 4.1
± 2.2 points (range, 1–8 points) to 1.3 ± 1.7 points (range, 0–5 points) at the final follow-up (p<0.001). The mean Constant score and ASES score were significantly increased from 55.5 ± 16.2 points (range, 23–82 points) to 88.7 ± 8.1 points (range, 71–100 points) and from 51.7 ± 16.0 (range, 10–70 points) to 87.4±10.6 points (range, 62–100 points) (p<0.001). All pa- tients had a stable radiological union at the end of the follow-up period (Fig. 5). The mean duration until union was 11.2 weeks (range, 8–16 weeks). The mean segmental defect was 3.3 ± 2.6 mm (range, 1–18 mm). The mean difference in clavicular length between operative and non-operative site was 0.9 ± 4.9 mm, and the mean difference in clavicular length between operative and non-operative site was 5.9 ± 6.9 mm (operative site, 155.5
± 15.9 mm; non-operative site, 161.5 ± 16.7 mm). There were no complications pertaining to the hardware, or infection.
Discussion
Our study showed a 100% union rate in 17 cases of non- union treated with open reduction and internal fixation with a plate using autologous iliac bone graft. The key modification of the autograft was the shape of the iliac crest graft, which was
A
B
C
D
E
Fig. 5. (A) Radiologic images of the patient who had 3 previously failed oper- ations at other institutions (1st operation-for fracture, 2nd and 3rd operation- for nonunion with hardware failure). Preoperative X-ray image before 1st operation for fracture. Th e classifi cation according to Edinburg was type IIB2.
(B) Postoperative X-ray of 1st operation for fracture. (C) Preoperative X-ray of 4th operation for nonunion. Nonunion with hardware failure was noted.
(D) Immediate postoperative X-ray using matchstick technique for nonunion.
Auto-iliac bone graft shaped matchsticks were noted (white arrow). (E) Hard- ware was removed at postoperative 24 months. Complete union was noted.
shaped in the form of a matchstick.
Clavicle fractures have a high healing rate with nonsurgical treatment and result in good functional outcomes.22) However, more recent evidence recommends surgical treatment for larger subsets of clavicle fractures than previously known, due to a higher risk of nonunion, symptomatic malunion, and suboptimal functional outcomes.3,23) Hill et al.24) reported that the majority of displaced mid-shaft clavicle fractures that were treated conserva- tively were associated with higher rates of nonunion and patient dissatisfaction with the final result.
Despite several concerns regarding autologous bone graft, including donor site morbidity and blood loss,25) open reduc- tion and internal fixation with plate and autologous bone graft is an accepted technique for atrophic nonunion of the clavicle, because of its osteoconductive, osteoinductive, and osteogenic effect.16-18)
Some authors have suggested that autologous bone graft might be unnecessary in every case of clavicle nonunion.26) En- drizzi et al.27) reported a high union rate (44 of 47 patients, 93%) in their series treated with local bone graft or demineralized matrix alone. Ramoutar et al.26) reported a 100% union rate (11 patients) in their series treated by fragment decortication and compression without bone graft. However, the definitive inter- pretation of these reports is not that bone graft is unnecessary in all cases of clavicle nonunion. Conventional internal fixation without bone graft or with demineralized matrix alone might be insufficient for bone healing in patients with repeated failed operations for nonunion. Autologous bone graft is accepted as the gold standard for nonunion surgery and a high healing rate of bone graft surgery was often reported.16,17) Addition of the bone graft to conventional internal fixation, as compared to con- ventional technique without bone graft could increase the union rate, particularly in difficult cases.
This technique has an advantage for bone healing, as com- pared with conventional cancellous bone graft, because of the comparatively large amount of bone graft and the strut bone ef- fect.
According to systematic review of clavicle fractures, the most common type of nonunion was the type IIB1 fracture that was initially treated with conservative management.2,28) We likewise found that the majority of fractures among the nonunion cases were type IIB1. The classification was not possible on X-ray for the nonunion cases that were treated with an earlier opera- tion. We observed 1 case of lateral 1/5th fracture nonunion of the clavicle. Displaced lateral end fractures of the clavicle are difficult to treat due to their small size and high rate of delayed union i.e., up to 45%, and nonunion up to 30%.29) We achieved complete union using 3.5 mm LCP with a matchstick bone graft technique in cases of nonunion with displaced lateral end frac- tures.
Matchstick shaped bones that are firmly tied with periosteum
have a strut bone effect, although somewhat weaker than actual strut bone graft. Our results were comparable with those of oth- er studies reporting a 91% to 100% union rate with autologous bone graft and plate fixation.8,16) The factors that contributed to superior outcomes (100% union) compared with other research would have been the usage of matchstick shape bone graft as well as the cerclage which was performed using suture material.
Wu et al.30) reported that wire cerclage could be a risk factor for clavicle nonunion, thus suture material should be used in place of wire.
This study had several limitations. First, the sample size was small. A larger sample size would facilitate a definitive conclu- sion. Second, we included no control group of plate fixation with autologous iliac bone chip graft alone. Third, the mean follow-up period was short. However, because this disease was associated with fracture, the results provided limited meaning regarding the healing of nonunion. And fourth, morbidity of the donor site including pVAS, and postoperative symptom dura- tion was not evaluated. Although there were no complications requiring specific postoperative management, prospective evalu- ation of the donor site would be helpful in advancing this tech- nique.
Conclusion
Matchstick autologous iliac bone grafting in clavicle nonunion showed a high union rate which might have contributed to the healing with an appropriate surgical technique.
References
1. Robinson CM. Fractures of the clavicle in the adult. Epidemiol- ogy and classification. J Bone Joint Surg Br. 1998;80(3):476-84.
2. Zlowodzki M, Zelle BA, Cole PA, Jeray K, McKee MD;
Evidence-Based Orthopaedic Trauma Working Group. Treat- ment of acute midshaft clavicle fractures: systematic review of 2144 fractures: on behalf of the Evidence-Based Orthopaedic Trauma Working Group. J Orthop Trauma. 2005;19(7):504-7.
3. Brinker MR, Edwards TB, O’Connor DP. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am. 2005;87(3):676-7; author reply 677.
4. Wick M, Müller EJ, Kollig E, Muhr G. Midshaft fractures of the clavicle with a shortening of more than 2 cm predispose to nonunion. Arch Orthop Trauma Surg. 2001;121(4):207-11.
5. Der Tavitian J, Davison JN, Dias JJ. Clavicular fracture non-union surgical outcome and complications. Injury.
2002;33(2):135-43.
6. Duncan SF, Sperling JW, Steinmann S. Infection after clavicle fractures. Clin Orthop Relat Res. 2005;439:74-8.
7. Capicotto PN, Heiple KG, Wilbur JH. Midshaft clavicle non-
unions treated with intramedullary Steinman pin fixation and onlay bone graft. J Orthop Trauma. 1994;8(2):88-93.
8. Boehme D, Curtis RJ Jr, DeHaan JT, Kay SP, Young DC, Rock- wood CA Jr. Non-union of fractures of the mid-shaft of the clavicle. Treatment with a modified Hagie intramedullary pin and autogenous bone-grafting. J Bone Joint Surg Am.
1991;73(8):1219-26.
9. Enneking TJ, Hartlief MT, Fontijne WP. Rushpin fixation for midshaft clavicular nonunions: good results in 13/14 cases.
Acta Orthop Scand. 1999;70(5):514-6.
10. Ngarmukos C, Parkpian V, Patradul A. Fixation of fractures of the midshaft of the clavicle with Kirschner wires. Results in 108 patients. J Bone Joint Surg Br. 1998;80(1):106-8.
11. Barlow T, Upadhyay P, Barlow D. External fixators in the treat- ment of midshaft clavicle non-unions: a systematic review. Eur J Orthop Surg Traumatol. 2014;24(2):143-8.
12. Kloen P, Werner CM, Stufkens SA, Helfet DL. Anteroinferior plating of midshaft clavicle nonunions and fractures. Oper Or- thop Traumatol. 2009;21(2):170-9.
13. Sun JZ, Zheng GH, Zhao KY. Minimally invasive treatment of clavicular fractures with cannulated screw. Orthop Surg.
2014;6(2):121-7.
14. Fuchs B, Steinmann SP, Bishop AT. Free vascularized cortico- periosteal bone graft for the treatment of persistent nonunion of the clavicle. J Shoulder Elbow Surg. 2005;14(3):264-8.
15. Van Tongel A, Kegels L, Berghs B, Karelse A, Van Isacker T, De Wilde L. Use of the clavicular part of the pectoralis major in treatment of failed revision osteosynthesis of the clavicle. J Shoulder Elbow Surg. 2014;23(5):729-36.
16. Ebraheim NA, Mekhail AO, Darwich M. Open reduction and internal fixation with bone grafting of clavicular nonunion. J Trauma. 1997;42(4):701-4.
17. Faraud A, Bonnevialle N, Allavena C, Nouaille Degorce H, Bonnevialle P, Mansat P. Outcomes from surgical treatment of middle-third clavicle fractures non-union in adults: a series of 21 cases. Orthop Traumatol Surg Res. 2014;100(2):171-6.
18. O’Connor D, Kutty S, McCabe JP. Long-term functional out- come assessment of plate fixation and autogenous bone graft-
ing for clavicular non-union. Injury. 2004;35(6):575-9.
19. Manske DJ, Szabo RM. The operative treatment of mid-shaft clavicular non-unions. J Bone Joint Surg Am. 1985;67(9):1367- 71.
20. Michener LA, McClure PW, Sennett BJ. American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, patient self-report section: reliability, validity, and responsive- ness. J Shoulder Elbow Surg. 2002;11(6):587-94.
21. Constant CR, Murley AH. A clinical method of func- tional assessment of the shoulder. Clin Orthop Relat Res.
1987;(214):160-4.
22. Neer CS 2nd. Nonunion of the clavicle. J Am Med Assoc.
1960;172:1006-11.
23. McKee MD, Pedersen EM, Jones C, et al. Deficits following nonoperative treatment of displaced midshaft clavicular frac- tures. J Bone Joint Surg Am. 2006;88(1):35-40.
24. Hill JM, McGuire MH, Crosby LA. Closed treatment of dis- placed middle-third fractures of the clavicle gives poor results.
J Bone Joint Surg Br. 1997;79(4):537-9.
25. Arrington ED, Smith WJ, Chambers HG, Bucknell AL, Davino NA. Complications of iliac crest bone graft harvesting. Clin Or- thop Relat Res. 1996;(329):300-9.
26. Ramoutar DN, Rodrigues J, Quah C, Boulton C, Moran CG.
Judet decortication and compression plate fixation of long bone non-union: Is bone graft necessary? Injury. 2011;42(12):1430-4.
27. Endrizzi DP, White RR, Babikian GM, Old AB. Nonunion of the clavicle treated with plate fixation: a review of forty-seven consecutive cases. J Shoulder Elbow Surg. 2008;17(6):951-3.
28. Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE. Estimating the risk of nonunion following nonopera- tive treatment of a clavicular fracture. J Bone Joint Surg Am.
2004;86(7):1359-65.
29. Edwards DJ, Kavanagh TG, Flannery MC. Fractures of the distal clavicle: a case for fixation. Injury. 1992;23(1):44-6.
30. Wu CL, Chang HC, Lu KH. Risk factors for nonunion in 337 displaced midshaft clavicular fractures treated with Knowles pin fixation. Arch Orthop Trauma Surg. 2013;133(1):15-22.