pISSN: 0378-6471 eISSN: 2092-9374 http://dx.doi.org/10.3341/jkos.2013.54.2.375
= 증례보고 =
내시경적 부비동 수술 시행 후 내직근 절제로 발생한 외사시를 1년이 지난 시점에서 수술적 치료를
통하여 교정한 1예
유애리⋅임혜빈
가톨릭대학교 의과대학 인천성모병원 안과 및 시과학교실
목적: 이비인후과 내시경적 부비동 수술시 발생한 내직근 절제로 인한 우안 외사시 환자에 대해 수상 1년 후 내직근을 제외한 상직근과 하직근의 전위술 및 외직근의 후전술을 차례로 시행하여 만족스러운 결과를 보였기에 이를 보고하고자 한다.
증례요약: 내시경적 부비동 수술 후, 우안 내직근 절제로 우안 외사시 발생한 41세 남자 환자로, 수상 1년 후 본원 내원하였으며, 안와 자기 공명 영상에서 내직근 절제 소견 확인되었으며, 초진 시 95PD의 우안 외사시 소견 보였다. 1차 수술로 우안 상직근 및 하직근 전위술을 시행하였다. 수술 6주 후 원거리, 근거리 외사시각 35PD 남은 상태로 교정되었으며, 남은 교정을 위해 2차 수술로 우안의 외직근 후전술(7 mm)을 시행하였다. 2차 수술 후 우안 외사시각 10PD 남은 상태로 교정되었으며 환자 미용적으로 만족하고 있으며, 복시도 호전되었다.
결론: 내시경적 부비동 수술 중 발생한 내직근 절단에 의한 의인성 우안 외사시에 대하여, 수상 후 1년이 지난 시점에서 1차 수술로 상직근, 하직근의 전위술(6 mm) 및 2차 수술로 외직근의 후전술(7 mm)을 시행함으로써, 외사시와 미용적 이상 및 복시증상을 교정하 였기에 이를 보고하고자 하는 바이다.
<대한안과학회지 2013;54(2):375-381>
■ 접 수 일: 2012년 5월 18일 ■ 심사통과일: 2012년 8월 24일
■ 게재허가일: 2012년 12월 15일
■ 책 임 저 자: 임 혜 빈
인천광역시 부평구 동수로 56 가톨릭대학교 인천성모병원 Tel: 1544-9004, Fax: 032-510-5833 E-mail: [email protected]
이비인후과에서 시행하는 내시경적 부비동 수술(FESS, Functional Endoscopic Sinus Surgery)은 축농증을 포함한 다양한 부비동 질환에 시행하는 흔한 수술방법이지만 복잡 한 비강과 부비동의 해부학적 구조에 대한 불완전한 지식 및 미숙한 기구조작 때문에 드물게 외안근 손상, 시신경 손 상, 비루관 손상 등의 안과적 합병증을 유발할 수 있다.1,2 내시경적 부비동 수술에 의한 안과 영역의 합병증으로는 국내에서 2002년도 Lee et al3이 내시경적 비강 내 용종 및 사골 절제술 후 발생한 내직근 손상을 수술 후 2달째 우안 외직근 후전술 시행 후 3달째 하멜샤임씨(Hummelsheim) 술식으로 교정한 예3가 보고되었으며, 2003 년도 Kim et al4이 우안의 내직근 손상과 시신경이 완전 절단된 환자를 보고한 바 있다. 2003년도 보고된 증례환자는 우안 시신경 의 절단으로 인한 복시 증상이 없어 수술적 치료를 시행하 지 않았고,42002년도에 보고된 증례환자에서는 본 증례에
서 기술한 것과 수술 방법에 차이가 있으며 무엇보다도 수 술 시기가 수상 후 3개월 이내였다. 또한 내시경적 부비동 수술 중 내직근 손상으로 발생한 외사시는 수상직후의 치 료가 이루어지는 것이 통상적이지만2수상 후 장기간 치료 받지 않고 지속적인 외사시를 보인 환자에서의 수술결과에 대한 보고는 국내에 없다.
본 증례는 축농증 진단하에 내시경적 부비동 수술(FESS) 시 행 후 우안 내직근이 절제되어 발생한 우안 외사시를 보였던 환자가 수상 후 1년이나 지난 시점에서 본원으로 전원되었음 에도 불구하고 상직근과 하직근의 전위술과 외직근의 후전술 을 시간적 간격을 두어 단계적으로 시행하여 외사시와 복시의 호전에서 좋은 결과를 보였기에 이를 보고하고자 한다.
증례보고
41세 남자환자가 내원 1년 전 타 병원 이비인후과에서 축농증 진단 하에 시행한 내시경적 부비동 수술(FESS) 후 발생한 우안 외사시를 주소로 내원하였다. 수술 후 복시와 우안의 외편위 발생하여 시행한 안와 자기 공명 영상(MRI) 결과 우안 내직근의 절제로 진단되었으며, 그 후 이비인후 과와 안과에서 별다른 치료 없이 경과관찰하다 환자가 원
A
B
Figure 1. Preoperative orbital magnetic resonance imaging
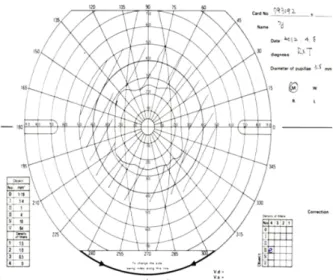
(MRI) of the patient. (A) T2-WI axial images show that medial rectus muscle has been resected and retracted anteriorly form- ing an anterior bulge (solid arrow head). (B) T1-W I axial im- ages also show discontinuity of medial rectus muscle (solid ar- row head). Compare to the normal opposite side. T2WI = T2 weighted image; T1W I = T1 weighted image.Figure 2. Nine cardinal movement photography taken at initial visit to our clinic. Large exotropia (95 PD) in the right eye and
marked limitation of adduction (nearly full limitation on medial gaze) in the right eye was noted.하여 본원으로 의뢰되었으며, 타 병원에서 시행한 안와 자 기 공명영상(MRI)을 확인한 결과 우안 내직근 절제를 확 인할 수 있었다(Fig. 1). 환자는 전신적으로 고혈압 외에 특
이사항 없었으며, 안과적 과거력 또한 특이사항 없었다. 우 안 나안 시력 0.8(우안 외전된 상태로 고개를 우측면으로 돌려 측정한 나안 및 교정 시력임), 좌안 나안 시력 0.7(교 정시력 0.9)이었으며, 굴절력상 우안 정시, 좌안 -1.0D의 근시가 있었고, 안압은 우안 13 mmHg, 좌안 15 mmHg였 으며 전안부 소견상 특이소견 관찰되지 않았다. 사시각 측 정 상 정면 주시 시, 95PD의 우안 외사시 소견이 관찰되었 으며, 우안 동향 운동 검사 시 우안 -4의 내전장애 보였다 (Fig. 2). 골드만 복시검사상 중앙 30도 이내의 복시 소견 이 관찰되었고(Fig. 3), 복시가 심하여 검사가 어려워 양안 시 검사는 의미가 없다고 판단하여 시행하지 않았다.
수상 후 1년의 시간이 지난 만성화된 외사시의 교정을 위 해서는 수술적 방법만이 가능하다고 판단되었고 내직근 절 제로 인한 우안 외사시 진단하에 수술을 계획하였다. 편위 정도가 심하였기에 수술은 시간적 간격을 둔 단계적 교정 을 계획하였고, 1차 수술로 우안의 상직근과 하직근의 전위 술을 시행하였다. 수술 시 내직근 절제부위는 육안으로 확 인되지 않았으나, Forced duction test 상 저항이 전혀 느껴 지지 않았다. 1차 수술 시 여러 가지 전위술의 방법 중 손상 된 근육의 방향 쪽으로 가장 많은 힘을 실어 줄 수 있는 총 건막 이전술(Full-tendon transposition procedure)을 시 행하였다. 수술 방법은 우안의 상직근과 하직근을 절개하여 각막윤부로부터 근육 부착부위까지의 거리를 유지하며 전
Figure 3. Goldman perimetry taken at initial visit. Shading
represents the area of binocular diplopia. Diplopia was present neal total field of vision include central 30 degree filed.A B C
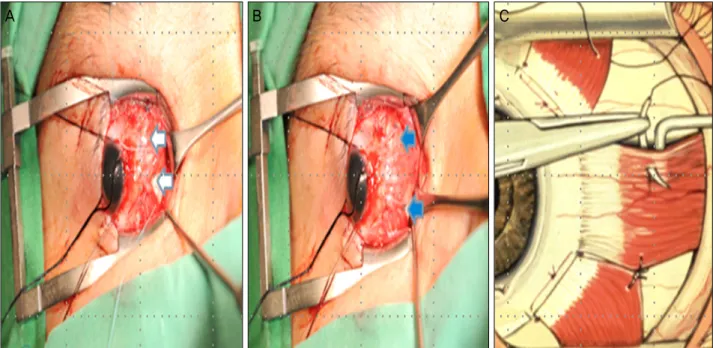
Figure 4. Photography taken in the operation theater. The superior rectus muscle and Inferior rectus muscle was isolated and cleared
of surrounding attachment. (A, solid arrow head) Full-tendon transposition of superior and inferior rectus was to the remnant medial rectus was performed. (B, solid arrow head) Schematic diagram of Full-tendon transposition. (C) Appearance of full tendon trans- position for resected medial rectus. Note that relative distances to the limbus.위하였으며(Fig. 4), 내직근 부착부위로부터 6 mm 지점의 근육 밀착술(Buckley procedure)을 시행하였다(Fig. 5).
수술 9일 후 정면 주시 시 우안 나안시력 0.8 측정되었으며, 25PD의 우안 외사시 소견 관찰되었고(Fig. 6), 우안의 -2 의 중등도의 내전장애 관찰되었다. 수술 6주 후 우안의 30-35PD의 외사시 소견 관찰되었고, 수직 편위는 관찰되 지 않았으며, 내전장애는 -2로 변화 없었다. 환자가 복시 증상을 계속 호소하여, 남은 외사시 교정을 위하여 1차 수 술 2달 뒤, 우안의 외직근 후전술 7.0 mm 시행하였다. 2차 수술을 시행한 3주 후, 정면 주시 시 10PD의 우안 외사시 측정되어 수술 전 사시각 보다 현저히 줄어든 소견 보였으 며, 내전장애는 변화 없었다(Fig. 7). 환자는 남은 10PD의 우안 외사시에 대해서 특별한 미용적 불편함을 호소하지
않았으며 골드만 복시검사상 좌우측방 30도 이상에서 복시 가 남아 있으나(Fig. 8) 환자가 일상생활의 불편함이 없어 졌기에 만족하였으며 수술 후 6개월이 지난 현재까지 사시 각 및 증상의 변화 없이 경과관찰 중이다.
고 찰
만성 부비동 질환에 있어서 이비인후과에서 시행하는 내 시경적 부비동 수술(FESS)는 흔히 선택되는 수술 방법이 며, 이에 따른 합병증의 발생률은 수술자와 사용된 술기에 따라 많은 차이가 있다. Wigand5는 372건의 내시경적 부비 동 수술 후 1.6%에서 뇌척수액 비루증이 있다고 하였고 Stammberger and Posawetz6는 4,500건 중에 0.07%의 합 병률을 보고하였다.1안과적 영역에서의 합병증으로는 Lessell1 의 보고에 따르면 외안근 손상, 비루관 손상, 안와 내 혈종 및 기종, 시신경 손상 등이 있고, 유병률은 각 보고마다 편 차가 있다. 안와내 손상이 의심될 경우 수술에 의한 손상과 안와 내 혈종 등을 확인하기 위해 영상촬영이 필요하며,2 급성 안와내 혈종일 경우에는 시력과 동공반응이 정상이면 경과관찰을 하고, 후안와 혈종에 의한 간접적인 시신경 압 박의 경우에는 고용량의 스테로이드 치료를 시행해야 한 다.7,8 수술 후 안구운동의 장애와 외안근 기능부전이 관찰 될 경우, 외안근의 손상을 의심해 봐야 한다. 내직근의 손상 은 Huang et al9이 보고한 바로는 5년 동안 735명의 수술 중 1명꼴로 발생하는 매우 드물게 발생하지만,2외안근 손 상 중에는 내직근의 손상이 제일 흔하며 그 다음이 하직근 의 손상이다.2,10만성 부비동염시 생길 수 있는 안와 내벽의
A B C
Figure 5. Buckley procedure. Buckley procedure uses a nonabsorbable suture to attach the edges of transposed muscle to the resected muscle.
The suture is placed approximately 6 mm posterior to new insertion, along the border of the transposed muscle. (A, solid arrow head) The effect of transposition can be further enhanced by suturing the border of transposed muscle. (B, solid arrow head) Schematic diagram of Buckley procedure. (C) Nonabsorbable suture is placed 6.0 mm from the insertion along the lateral border of the transposed muscle.
Figure 6. Nine cardinal movement photography taken at 7 days after initial surgery (right superior and inferior rectus muscle
full-tendon transposition). Right exodeviation about 25 prism diopters by alternative cover test was noted and moderated limitation on medial gaze of right eye was still remained.약화 등에 의해 사골봉소와 비강내로부터 안와 연부조직을 분리할 때 그 경계가 명확치 않은 경우가 많다.2그래서 수
술 시 안와 내벽의 손상 때문에 안와 내 지방이 수술부위로 돌출하거나 외안근의 손상이 동반될 수 있다.2
Figure 7. Photography taken at 3 weeks after second surgery (right lateral rectus muscle 7 mm recession). Right exodeviation de-
creased to 10 prism diopters by alternative cover test and limitation on medial gaze of the right eye did not change.Figure 8. Goldman perimetry taken at 6 weeks after second
surgery. Improvement in the area of diplopia area was noted.But remnant peripheral diplopia area was noted.
내직근 손상은 크게 4가지 유형으로 나눌 수 있는데, 첫 번째 유형은 본 증례의환자와 같이 내직근의 전절제 또는 부분 절제된 경우이며 이때는 큰 외사시각을 보일 수 있다.2 두 번째 유형은 혈종에 의한 내직근 손상일 경우이며 그보 다 작은 중등도의 사시각을 보이고, 세 번째 유형은 도르래 신경의 손상인 경우이며 이 경우에도 중등도 사시각을 보 일 수 있으며, 네 번째 유형은 내직근 또는 조직의 감돈에
의한 경우이며, 제일 눈 위치에서 경도의 외측 편위를 보이 나 눈 모음의 현저한 장애를 보일 수 있다.2외안근 감돈의 경우 2주간 경과 관찰 후에도 증상 호전이 없으면 수술을 고려한다.11 지방조직의 감돈이나 신경손상에 의한 외안근 마비는 비수술적 방법으로 증세 호전을 기대할 수 있으므 로 정확한 감별 후 수술 여부를 결정해야 한다.12
본 증례는 내시경적 부비동 수술 도중 우안의 내직근 절 제로 인한 심한 외편위 환자의 예로, 과다한 외편위각의 교 정을 위하여 두 번의 수술적 치료를 시행하였으며, 두 수술 간 2개월의 시간적 간격을 둔 단계적 수술을 시행하였다.
여러 연구에서 영구적인 조직의 구축 및 섬유화를 방지하 기 위해서는 수상 후 3-4주 내에 수술이 이루어져야 한다 고 보고되고 있으나,2,9,13,14 본 증례의 환자는 기존의 보고 와 달리 수상 후 1년이 넘은 시점에서 외사시 교정술의 효 과를 보였다는 점에서 의의가 있다고 할 수 있다. 본 증례 는 내시경적 부비동 수술 후 발생한 외안근 수상을 수술로 교정한 2002년도 국내 보고와는 몇 가지 뚜렷한 차이가 있 는데 수상 후 상당한 시간이 지난 시점에서 교정수술을 했 다는 점, 기존 수술방법과는 다르게 총 건막 이전술(Full- tendon transposition procedure)을 시행한 후 근육 밀착술 (Buckley procedure)을 시행하여 기존의 보고보다 만족스 러운 결과를 보였다는 점이다.
사시 수술을 시행할 때 근육을 부착부위에서 절제하는
과정에서 발생할 수 있는 전 모양체 동맥의 손상과 전안부 허혈을 막기 위해 한번에 3개 이상의 직근을 수술하지 않는 것이 일반적인 원칙이므로 본 증례에서는 단계적 수술을 계획하였다.15,16앞선 국내 증례가 1차 수술로 외직근 후전 술부터 시행한 것과는 달리 본 증례 환자에서는 외직근을 제외한 상직근과 하직근의 전위술을 먼저 시행하기로 계획 하였다. 이는 전위술의 경우 사시각의 교정 정도의 예측이 쉽지 않기 때문에 이를 먼저 시행하여 우안 외사시를 최대 한 교정한 뒤 남은 양의 우안 외사시를 외직근 후전술로 교 정하기로 계획하였으며, 수술 후 경과는 만족스러웠다. 1차 수술에는 상직근과 하직근 2개 근육의 전위술을 시행하기 로 계획하였으며 전위술의 방법으로, 총 건막 이전술을 시 행하였다. 비흡수성 봉합사(5-0 Ethibond®Ethicon, USA) 를 이용한 총건막 이전술(Full tendon)은 냅(knapp)술식이 나 젠슨(Jensen)술식 또는 하멜샤임(Hummelsheim)술식 같은 근육 분리술(muscle-splitting procedure)에 비하여 외편위각의 교정 효과가 좋은 것으로 보고된 바 있다.17,18 본 증례에서는 교정 효과를 극대화하기 위하여 전위된 근 육의 경계(border)에 비흡수성 봉합사로 밀착술(Buckley procedure)을 시행하였으며 2달의 시간적 간격을 두어 2차 수술로 외직근의 후전술(7.0 mm)을 시행하였다. 2차 수술 후 6개월째 경과관찰 중이며 현재 현재 10PD의 우안 외사 시 남아있으나 환자가 일상적 불편 및 복시의 개선으로 만 족하고 있는 상태이다.
본 증례는 내시경적 부비동 수술(FESS) 후 내직근의 의 인성 절제가 발생한 1년이 지난 시점에서 수술을 시행하였 음에도 복시와 외사시가 현저하게 교정된 경우이다. 수상 후 가능한 빠른 시기에 수술을 시행하여 최종 우안 외사시 각이 20PD까지 교정된 기존의 보고와는 달리 본 증례는 수 상 1년이 지난 시점에서 수술을 시행하였음에도 불구하고 단계적 수술(총건막 이전술과 Buckley procedure)을 시행 하여 보다 만족스러운 결과를 보였다. 저자들은 본 증례를 통하여 내시경적 부비동 수술 후 발생하는 안과적 합병증 에 대한 적극적인 접근에 도움이 되고자 한다.
참고문헌
1) Lessell S. Indirect optic nerve trauma. Arch Ophthalmol 1989;
107:382-6.
2) Bleier BS, Schlosser RJ. Prevention and management of medial rectus injury. Otolaryngol Clin North Am 2010;43:801-7.
3) Lee MH, Kin SD, Hur YJ. A case of medial rectus muscle injury af- ter functional endoscopic sinus polypectomy and ethmoidectomy.
J Korean Ophthalmol Soc 2002;43:934-9.
4) Kim HC, Kim JH, Lee SY. A case of medial rectus muscle injury and optic nerve transection developed during functional endo- scopic sinus surgery. J Korean Ophthalmol Soc 2003;44:2705-10.
5) Wigand ME. [Transnasal, endoscopical surgery for chronic sinusitis. III. Endonasal ethmoidectomy (author's transl)]. HNO 1981;29:287-93.
6) Stammberger H, Posawetz W. Functional endoscopic sinus surgery.
Concept, indications and results of the Messerklinger technique.
Eur Arch Otorhinolaryngol 1990;247:63-76.
7) Kitthaweesin K, Yospaiboon Y. Dexamethasone and methyl- prednisolone in treatment of indirect traumatic optic neuropathy. J Med Assoc Thai 2001;84:628-34.
8) Neuhaus RW. Orbital complications secondary to endoscopic sinus surgery. Ophthalmology 1990;97:1512-8.
9) Huang CM, Meyer DR, Patrinely JR, et al. Medial rectus muscle injuries associated with functional endoscopic sinus surgery: char- acterization and management. Ophthal Plast Reconstr Surg 2003;
19:25-37.
10) Thacker NM, Velez FG, Demer JL, et al. Extraocular muscle dam- age associated with endoscopic sinus surgery: an ophthalmology perspective. Am J Rhinol 2005;19:400-5.
11) Lee MS, Ahn JH, Kim HY, Lee SY. Clinical study of orbital wall fracture. J Korean Ophthalmol Soc 1997;38:1687-93.
12) Koornneef L. Current concepts on the management of orbital blow- out fractures. Ann Plast Surg 1982;9:185-200.
13) Hong JE, Goldberg AN, Cockerham KP. Botulinum toxin A ther- apy for medial rectus injury during endoscopic sinus surgery. Am J Rhinol 2008;22:95-7.
14) Penne RB, Flanagan JC, Stefanyszyn MA, Nowinski T. Ocular mo- tility disorders secondary to sinus surgery. Ophthal Plast Reconstr Surg 1993;9:53-61.
15) France TD, Simon JW. Anterior segment ischemia syndrome fol- lowing muscle surgery: the AAPO&S experience. J Pediatr Ophthalmol Strabismus 1986;23:87-91.
16) Olver JM, Lee JP. The effects of strabismus surgery on anterior segment circulation. Eye (Lond) 1989;3(Pt 3):318-26.
17) Hong S, Chang YH, Han SH, Lee JB. Effect of full tendon trans- position augmented with posterior intermuscular suture for para- lytic strabismus. Am J Ophthalmol 2005;140:477-83.
18) Foster RS. Vertical muscle transposition augmented with lateral fixation. J AAPOS 1997;1:20-30.
=ABSTRACT=
Sequential Correction for Large Exotropia: A Case of Iatrogenic Exotropia Developed after Excision of Medial Rectus Muscle During
Functional Endoscopic Sinus Surgery (FESS)
Ae Ri Yoo, MD, Hye Bin Yim, MD, PhD
Department of Ophthalmology and Visual Science, Incheon St. Mary’s Hospital, The Catholic University of Korea College of Medicine, Incheon, Korea
Purpose: To report a case of iatrogenic exotropia caused by accidental excision of medial rectus muscle during functional endoscopic sinus surgery (FESS), which was successfully corrected by sequential surgical intervention (superior and in- ferior rectus muscle transposition followed by lateral rectus muscle recession).
Case summary: Forty one year old male patient visited our clinic with large exotropia of the right eye developed after func- tional endoscopic sinus surgery (FESS) which was performed one year ago. At the initial visit in our clinic, there was a large exotropia (95 PD) of the right eye and transection of the medial rectus muscle was observed at the orbital MRI. In or- der to correct this large iatrogenic exotropia, sequential surgery was planned. Initially, full-tendon transposition of the right superior and inferior rectus muscle was performed which reduced the deviation to 35 PD. Six weeks after the initial sur- gery, 7 mm right lateral rectus muscle recession was additionally performed, which resulted in exotropia of 10 PD. Diplopia was also improved and the patient was esthetically satisfied with the result.
Conclusions: Even in a case of iatrogenic exotropia following one year after an accidental excision of medial rectus muscle during intranasal sinus surgery, sequential surgery such as transposition of superior and inferior rectus muscle followed by lateral rectus muscle recession can result in satisfying cosmetic and functional improvement.
J Korean Ophthalmol Soc 2013;54(2):375-381
Key Words: Endoscopic sinus surgery, Exision of extraocular muscle, Full-tendon transposition, Iatrogenic exotropia, Sequential strabismus surgery
Address reprint requests to Hye Bin Yim, MD, PhD
Department of Ophthalmology, The Catholic University of Korea, Incheon St. Mary’s Hospital
#56 Dongsu-ro, Bupyeong-gu, Incheon 403-720, Korea
Tel: 82-1544-9004, Fax: 82-32-510-5833, E-mail: [email protected]