한국 여성에서 유방촬영술 암검진의 득과 실 Column Special
배종면*
제주대학교 의학전문대학원 예방의학교실
On the Benefi ts and Harms of Mammography for Breast Cancer Screening in Korean Women
Jong-Myon Bae*
Department of Preventive Medicine, Jeju National University School of Medicine, Jeju, Korea
As breast cancer is becoming more prevalent in Korean women, mammography screening for early cancer detection is very important. However, risks, including over-prescription of mammography screening, have been emphasized recently. The governments of Canada and the USA have reported that women younger than 50 years of age do not need to be screened routinely. The main reason for this recommendation is that the risk of over-diagnosis and biopsy may be greater than the benefit of decreasing mortality in younger women. Korean women have a 1/3 lower incidence rate than non-Hispanic White women, and the peak age group in Korean and USA women are 45 to 49 and 75 to 79 years, respectively. These epidemiological findings indicate that Korean women have a higher risk of unnecessary interventions and anti-cancer treatment as they have a higher chance of false positive in screening mammography. These results suggest that the national screening guidelines for Korean women should be adapted and screening mammography in normal risk healthy women should be optional.
Keywords: Guidelines; Mammography; Mass Screening; Breast Neoplasms
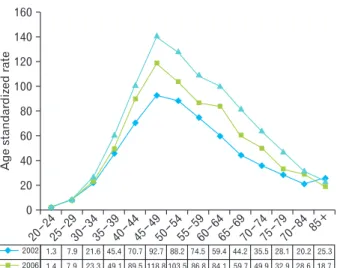
1/3 수준으로 낮다.3) 연령군별로 살펴보면 북미 여성은 연령 증가에 따라 급속히 증가하여 75–79세에 최대 수준에 이르지 만, 한국 여성은 전 연령층에서 북미보다 낮으면서 45–49세 에 최대치를 보인 다음 오히려 감소하는 분포를 보이고 있다 (Figure 1).4) 이런 패턴은 2002, 2006, 2010년을 비교해보아도 여전히 같은 모습을 유지하고 있다(Figure 2).3)
북미와 비교하여 낮은 발생률을 갖는 한국 여성의 유방암 은 ASR이 십만 명 중 45.4명으로 갑상선 다음의 2위를 차지하 고 있으나,3) 사망률은 십만 명 중 7.5명으로 폐암-위암-대장암- 간암-췌장암보다 낮다.5) 이렇게 발생률 대비 사망률이 상대적 으로 낮은 것은 국가암검진에 포함된 유방촬영술의 시행효과 라고도 해석할 수 있겠다.6) 또한 국가암검진대상 5대암에서 유방암 조기검진 수검률이 평균보다 높다는 점은 우리나라 여성의 유방암에 대한 관심 또한 높으면서 조기검진 사업투 입 비용 또한 큼을 알 수 있다.7)
우리나라를 포함하여 전 세계적으로 유방촬영술을 이용
서론
유방암은 전 세계적으로 2번째로 많은 암이면서, 여성 암 중 1위를 차지하고 있다.1) 2013년도에 발표한 미국 여성의 유 방암은 여성암 발생률 1위, 사망률 2위를 차지하고 있으며, 인 종별로는 백인 여성이 가장 높고 (127.3명/십만 명) 아시아계 가 가장 낮은 것으로 보고하였다(84.7명/십만 명).2) 이에 비하 여 2010년도 한국 여성의 연령표준화 발생률(age standardized rate, ASR)은 십만 명 중 45.4명으로 미국 백인 여성에 비하여
Received: December 15, 2013, Accepted: December 30, 2013
*Corresponding Author: Jong-Myon Bae
Tel: 064-764-3856, Fax: 064-725-2593 E-mail: jmbae@jejunu.ac.kr
Korean Journal of Family Practice
Copyright © 2014 by The Korean Academy of Family Medicine
하여 유방암 조기검진사업을 시행하고 있다.8) 그러나 우리나 라만 해도 유방암의 역학적 특성이 다름에도 불구하고,9,10) 북 미 및 북유럽 백인 여성을 대상으로 수행한 무작위임상시험 연구결과를 근거로 국가유방암검진지침을 결정하고 필수 검 진항목으로 포함하고 있다. 그러나 최근 들어 미국과 캐나다 의 북미를 중심으로 50세 미만에서 유방촬영술 검진은 사망 률 감소라는 효과보다는 과다진단에 따른 불필요한 검사와 시술의 위해가 더 많다는 논의가 개진되고 있다.11) 이에 따라 관련한 논쟁들을 검토하여서 한국 여성에 있어 유방암 검진 지침의 수정 필요성을 점검하고, 암 조기검진을 수행하는 일 차진료의사는 어떻게 수용해야 할 지를 정리하는 것이 본 논 문의 목적이다.
유방암검진효과에 대한 논쟁
유방촬영술의 조기검진에 따른 사망률 저하의 효과에 대 하여 본격적으로 의문이 제기된 계기는 2000년도 Lancet에 발 표된 ‘Is screening for breast cancer with mammography justifiable?’
이란 논문이었다.12) 해당 논문의 저자인 Gotzsche와 Olsen12)은 기존의 8개의 무작위배정연구를 평가했을 때, 6개는 연구방 법에 문제가 있었으며, 그나마 질적 수준이 있다고 판단한 나 머지 2개의 연구결과는 효과가 없게 나와서 유방촬영술을 이 용한 조기검진을 시행해서는 안된다고 주장하였다. 이상의
주장에 대한 다각도의 반박들이 있었고,13,14) 저자들의 재분석 과 해명도 이어졌다.15,16) 이런 논쟁에 더하여 2002년 캐나다 연 구팀은 유방암 검진 시행 후 11–16년의 추적을 한 결과, 자가 혹은 의사의 유방촉진법을 시행한 군과 비교할 때 유방촬영 술 시행군의 사망률은 차이가 없다고 발표하였다.17) 논란이 증폭되는 가운데 그 해 World Health Organization 산하 국제암 연구소(International Agency for Research on Cancer)는 추가적인 연구의 필요성을 제시하였다.18)
논란이 재촉발된 것은 2009년 US Preventive Services Task Force (USPSTF)란 미국 정부가 주도한 특별위원회에서 국가 암검진지침을 개정하면서, 50–74세 여성은 유방촬영술 검 진을 1년에서 2년으로 늦추고, 50대 미만은 득보다 실이 더 많기에 유방촬영술 시행을 권하지 않는 것으로 결정한 것이 다.19) 주목할 것은 40–49세 여성에서 위양성이 60%로 불필요 한 추가검사와 시술이 이루어진다는 사실이다. 같은 해 The Cochrane Collaboration에서 1명의 유방암 사망자를 줄이기 위 해서는 10명의 건강한 여성이 불필요한 검사나 시술을 받는 다는 보고가 있었다.20) 이 결론은 2011년과 2013년도에도 여전 히 유효한 근거이다.21,22)
2011년도에 미국 USPSTF와 같은 위상을 갖는 캐나다 Canadian Taskforce on Preventive Health Care 위원회는 50세 미 만에서의 과다진단(over-diagnosis)과 생검 위험이 상대적으로 높다고 발표하였다.23) 그리고 과다진단은 검진 시행자의 19%
정도라고 2012년도 영국에서 발표하였다.24) 추가로 과다진단 Figure 1. Incidence rates of female breast cancer by age in Canada,
USA, and Korea. From International Agency for Research on Cancer. Cancer incidence in fi ve continents volume X [Internet].
Available from: http://ci5.iarc.fr/CI5-X/ci5-X.htm.4)
Figure 2. Trends in female breast cancer incidence by age, 2002, 2006, 2010 in Korea. From National Cancer Center. Annual report of cancer statistics in Korea [Internet]. Available from: http://ncc.
re.kr/manage/manage03_033_list.jsp.3)
에 따른 불필요한 수술 및 항암제 치료로 사망하는 것을 고려 한다면 검진의 위해는 실제보다 더 크다고 주장하고 있다.25) 이와 함께 효과 대비 비용이 큰 검진에 대한 의료윤리적 문제 까지 제기되고 있다.26)
한국 여성의 유방암 검진지침에 대한 권고안
이상의 논란 흐름을 살펴보았을 때, 유방촬영술을 이용한 유방암 검진을 반대하는 이유는 다음 두 가지로 정리해 볼 수 있다. 첫째, 유방암 검진으로 사망률을 줄인다는 효과에 대한 의문 제기이다. Miller27)는 본격적인 시행을 하는 시점에 이미 유방암 사망률이 떨어지고 있었다고 지적하였고, Berry 등28)은 사망감소가 검진뿐만 아니라 치료법 향상에 따른 것이라고 발표하였기 때문이다. 둘째, 검진의 위해에 해당하는 과다진 단의 수준이 예상보다 심각하다는 것이다.11,29) 영국의 19%를 위시하여 유럽 7%에서 미국 30%라는 연구결과가 발표되었기 때문이다.24,30) 이렇듯 생각보다 득은 낮고 실이 높다는 근거들 이 발표되면서,11) 미국은 상대적으로 실이 큰 50대 미만의 연 령층에 대하여는 유방촬영술 검진을 권하지 않는 것으로 결 정한 것이다.19)
그렇다면 이런 근거들을 한국의 여성에 대하여는 어떻게 적용하고 해석해야 하는가? 특히 건강검진은 득보다는 실에 더 무게를 실어야 한다는 점에서,31) 다음 4가지로 정리할 수 있 다.
첫째, 한국 여성은 북미나 북유럽의 유방암 발생률보다 약 1/3 수준이기에, 검진시행으로 얻는 득은 발표된 것들보다 더 낮으며, 반면에 양성자를 찾아내기 위한 비용은 더 많다고 해 석할 수 있다.9,32) 다시 말해서 우리보다 3배 높은 발생률을 보 이는 백인 여성에 있어 유방촬영술 시행에 대한 논란이 있다 면, 우리 여성에서 시행의 이득보다는 위해가 더 클 것으로 볼 수 있다.
둘째, 북미와 달리 45세를 정점으로 발생률이 감소하는 50 세 이상의 건강인 한국 여성에 대한 검진주기를 재결정할 필 요가 있다.33) 현재의 2년 주기는 북미 및 북유럽 백인 여성을 대상으로 한 연구결과에 기반하고 있기 때문이다. 한국인 여 성을 대상으로 한 연구결과가 시급히 필요한 것이 사실이며, 이런 근거가 마련되기 전까지 북미보다 발생률이 현저히 낮 기 때문에 50세 이상이라고 해도 유방암 검진을 시행하는 것 은 득보다 실이 더 많다고 추론해 낼 수 있다.
셋째, 한국 여성의 유방암 발생률이 가장 높은 연령대는 45–49세로, 북미나 북유럽의 환자보다 훨씬 젊다는 사실이다.
이렇게 노년층에 비하여 젊은 연령층에 대한 필수 검진은 과
다진단이 될 위험이 높고,34) 비용이 더 많이 들며,35) 유방촬영 술로 인해 노출되는 방사선에 더 민감하며,36) 유방암 진행속 도가 빨라 주기 재조정이 필요하다는33) 기존의 연구결과에 비 추어 볼 때 유방촬영술의 이득보다는 위해의 가능성이 더 높 다는 것을 의미한다.
넷째, 서구 백인 여성에 비하여 한국 여성을 포함한 아시 아 여성의 유방조직의 밀도가 높다는 특성 또한 감안할 필요 가 있다.37) 이렇게 밀도가 높을 경우 유방촬영술의 판독 민감 도가 떨어지고,38,39) 위음성이 높아져서,40,41) 조기검진의 이득 을 제대로 확보하기 어렵기 때문이다.
이상의 내용들을 요약하면 현재 국가암검진지침에서 유 방촬영술이란 검사법, 40세란 시작 연령, 2년이란 주기 모두 재검토하여야 한다는 것이다. 나아가 이득보다 위해가 많다 는 근거에 따라 필수검진에서 우선적으로 배제해야 할 이유 가 충분하다는 것이다.
한국 여성의 유방암 검진지침에 있어 일차 의료인에 대한 권고안
북미와 유럽에서 50세 미만 여성에 대한 유방촬영술 검진 은 득보다 실이 높아 권하지 않는 분위기에서 우리나라 여성 에 대한 유방암 검진시행은 어떻게 해야 하는가? 이를 일차의 료인 입장에서 정리하면 다음과 같다.
첫째, 연령이 50세 미만인 일반 건강인에 대하여는 암검진 이 필수가 아니라 선택이라는 것을 수용할 필요가 있다. 그리 고 암검진대상은 유방암 발생 위험요인을 가진 고위험군에 집중하는 것이 필요하다. 이를 위해서 한국 여성에서의 고위 험군 선별이 가능한 위험예측도구 개발이 시급히 이루어져야 한다.41,42)
둘째, 일반인에게 과학적 근거로 얻어낸 득과 실의 정확한 정보를 충분히 제공해야 한다는 것이다. 그래서 환자의 가치 가 반영된 가운데 암검진이 수행될 수 있도록 여건을 형성해 야 한다는 것이다. 이를 위해서는 인터넷, 동영상, 캠페인, 팜플 렛 등의 홍보활동이 정부기관과 관련 학회 수준에서 체계적 으로 추진될 필요가 있다.43,44)
셋째, 현재 주된 검사법인 필름형 유방촬영술이 아닌 다 른 검진법을 개발하는 연구가 필요하다. 특히 40대 이하의 연 령층은 조직밀도가 높다는 점을 감안한 디지털 유방촬영술이 나, 방사선노출을 고려한 유방초음파술 등의 시행효과에 대 한 연구가 한국 여성을 대상으로 수행되어야 할 것이다.45,46)
결론
한국 여성에 있어 유방촬영술을 활용한 유방암 검진이 위 해보다는 이득이 많다는 근거가 확보되지 않는 한, 현재의 국 가암검진지침은 제고해야 하며 필수가 아닌 고위험군 중심으 로 조기암검진정책을 변경할 필요가 있다. 따라서 한국 여성 중 고위험군 선별을 위한 도구를 관련 학회 중심으로 개발, 공 인하여 일반인도 자신이 가진 고위험 정도를 판단하면서, 유 방촬영술의 득과 실을 충분히 이해한 다음 검사를 결정할 수 있는 정보를 적극 제공해야 할 것이다.
감사의 글
본 논문은 재단법인 대한암연구재단의 2013년도 암연구 지원사업에 의한 것이다.
요약
한국 여성에서 유방암의 질병부담이 높아지면서 유방촬 영술로 조기에 유방암을 검진하는 것이 암관리 차원에서 중 요하다. 그러나 최근들어 유방촬영술의 효과에 대한 의문이 제기되면서 미국과 캐나다 정부는 50세 미만의 일반 여성에 서 암검진을 위한 정기적인 유방촬영술을 권고하지 않도록 해당 지침을 개정하였다. 이런 조치의 배경에는 젊은 여성일 수록 암사망감소란 득보다는 과다진단에 따른 불필요한 진단 과 치료가 이루어질 위험이 더 크다는 판단때문이다. 한국 여 성은 서구 백인여성에 비하여 발생률이 1/3 수준으로 낮으면 서, 45–49세에 가장 높은 발생 수준을 보이고 있다. 이러한 역 학적 특성들을 감안하면 한국여성은 검진용 유방촬영술을 통 해 위양성 진단을 받아 불필요한 항암 치료를 받을 위험이 더 높다고 볼 수 있다. 따라서 일반 여성을 대상으로 암검진용 유 방촬영술을 필수로 권고하고 있는 국가암검진 지침은 대상자 의 상태에 맞추어 시행되도록 개정할 필요가 있다.
중심단어: 지침, 유방촬영술, 조기암검진, 유방암
REFERENCES
1. International Agency for Research on Cancer. GLOBOCAN 2012:
estimated cancer incidence, mortality and prevalence worldwide in 2012 [Internet]. Lyon: International Agency for Research on Cancer; 2012 [cited 2013 Dec 14]. Available from: http://
globocan.iarc.fr/Pages/fact_sheets_cancer.aspx.
2. Desantis C, Ma J, Bryan L, Jemal A. Breast cancer statistics, 2013.
CA Cancer J Clin 2014;64:52-62.
3. National Cancer Center. Annual report of cancer statistics in Korea [Internet]. Goyang: National Cancer Center [cited 2013 Dec 14].
Available from: http://ncc.re.kr/manage/manage03_033_list.jsp.
4. International Agency for Research on Cancer. Cancer incidence in five continents volume X [Internet]. Lyon: International Agency for Research on Cancer; 2013 [cited 2013 Dec 14].
Available from: http://ci5.iarc.fr/CI5-X/ci5-X.htm.
5. Statistics Korea. Nationwide cancer registry & statistics [Internet].
Daejeon: Statistics Korea [cited 2013 Dec 14]. Available from:
http://kosis.kr/statisticsList/statisticsList_01List.jsp?vwcd= MT_
ZTITLE&parentId=D.
6. Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med 2002;137(5 Part 1):347- 60.
7. Kim Y, Jun JK, Choi KS, Lee HY, Park EC. Overview of the National Cancer screening programme and the cancer screening status in Korea. Asian Pac J Cancer Prev 2011;12:725-30.
8. International Cancer Screening Network. Breast cancer screening programs in 26 ICSN countries, 2012: organization, policies, and program reach [Internet]. Bethesda: International Cancer Screening Network; 2012 [cited 2013 Dec 14]. Available from: http://appliedresearch.cancer.gov/icsn/breast/screening.
html.
9. Yoo KB, Kwon JA, Cho E, Kang MH, Nam JM, Choi KS, et al.
Is mammography for breast cancer screening cost-effective in both Western and asian countries?: results of a systematic review.
Asian Pac J Cancer Prev 2013;14:4141-9.
10. Leong SP, Shen ZZ, Liu TJ, Agarwal G, Tajima T, Paik NS, et al.
Is breast cancer the same disease in Asian and Western countries?
World J Surg 2010;34:2308-24.
11. Marmot MG. Sorting through the arguments on breast screening.
JAMA 2013;309:2553-4.
12. Gotzsche PC, Olsen O. Is screening for breast cancer with mammography justifiable? Lancet 2000;355:129-34.
13. Duffy SW. Interpretation of the breast screening trials: a commentary on the recent paper by Gotzsche and Olsen. Breast 2001;10:209-12.
14. Kopans DB. The most recent breast cancer screening controversy about whether mammographic screening benefits women at any
age: nonsense and nonscience. AJR Am J Roentgenol 2003;180:
21-6.
15. Olsen O, Gotzsche PC. Cochrane review on screening for breast cancer with mammography. Lancet 2001;358:1340-2.
16. Gotzsche PC. On the benefits and harms of screening for breast cancer. Int J Epidemiol 2004;33:56-64.
17. Miller AB, To T, Baines CJ, Wall C. The Canadian National Breast Screening Study-1: breast cancer mortality after 11 to 16 years of follow-up: a randomized screening trial of mammography in women age 40 to 49 years. Ann Intern Med 2002;137(5 Part 1):305-12.
18. International Agency for Research on Cancer. IARC handbooks of cancer prevention: volume 7, breast cancer screening. Lyon:
International Agency for Research on Cancer; 2002.
19. Woolf SH. The 2009 breast cancer screening recommendations of the US Preventive Services Task Force. JAMA 2010;303:162- 3.
20. Gotzsche PC, Nielsen M. Screening for breast cancer with mammography. Cochrane Database Syst Rev 2009;(4):CD001877.
21. Gotzsche PC, Nielsen M. Screening for breast cancer with mammography. Cochrane Database Syst Rev 2011;(1):CD001877.
22. Gotzsche PC, Jorgensen KJ. Screening for breast cancer with mammography. Cochrane Database Syst Rev 2013;6:CD001877.
23. Canadian Task Force on Preventive Health Care, Tonelli M, Connor Gorber S, Joffres M, Dickinson J, Singh H, et al.
Recommendations on screening for breast cancer in average-risk women aged 40-74 years. CMAJ 2011;183:1991-2001.
24. Independent UK Panel on Breast Cancer Screening. The benefits and harms of breast cancer screening: an independent review. Lancet 2012;380:1778-86.
25. Baum M. Harms from breast cancer screening outweigh benefits if death caused by treatment is included. BMJ 2013;346:f385.
26. Brody H. From an ethics of rationing to an ethics of waste avoidance. N Engl J Med 2012;366:1949-51.
27. Miller AB. Is mammography screening for breast cancer really not justifiable? Recent Results Cancer Res 2003;163:115-28.
28. Berry DA, Cronin KA, Plevritis SK, Fryback DG, Clarke L, Zelen M, et al. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med 2005;353:1784-92.
29. Puliti D, Duffy SW, Miccinesi G, de Koning H, Lynge E, Zappa M, et al. Overdiagnosis in mammographic screening for breast cancer in Europe: a literature review. J Med Screen 2012;19
Suppl 1:42-56.
30. Bleyer A, Welch HG. Effect of three decades of screening mammography on breast-cancer incidence. N Engl J Med 2012;
367:1998-2005.
31. Barton MB. Breast cancer screening: benefits, risks, and current controversies. Postgrad Med 2005;118:27-8, 33-6, 46.
32. Moss S. Should women under 50 be screened for breast cancer?
Br J Cancer 2004;91:413-7.
33. Gemignani ML. Breast cancer screening: why, when, and how many? Clin Obstet Gynecol 2011;54:125-32.
34. Krishnaiah PB, Nunes NL, Safranek S. FPIN’s clinical inquiries:
screening mammography for reducing breast cancer mortality.
Am Fam Physician 2012;85:176-83.
35. Salzmann P, Kerlikowske K, Phillips K. Cost-effectiveness of extending screening mammography guidelines to include women 40 to 49 years of age. Ann Intern Med 1997;127:955-65.
36. Berrington de Gonzalez A. Estimates of the potential risk of radiation-related cancer from screening in the UK. J Med Screen 2011;18:163-4.
37. El-Bastawissi AY, White E, Mandelson MT, Taplin S. Variation in mammographic breast density by race. Ann Epidemiol 2001;11:
257-63.
38. Kolb TM, Lichy J, Newhouse JH. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology 2002;225:165- 75.
39. Boyd NF, Guo H, Martin LJ, Sun L, Stone J, Fishell E, et al.
Mammographic density and the risk and detection of breast cancer. N Engl J Med 2007;356:227-36.
40. Mandelson MT, Oestreicher N, Porter PL, White D, Finder CA, Taplin SH, et al. Breast density as a predictor of mammographic detection: comparison of interval- and screen-detected cancers. J Natl Cancer Inst 2000;92:1081-7.
41. Warner E, Heisey R, Carroll JC. Applying the 2011 Canadian guidelines for breast cancer screening in practice. CMAJ 2012;
184:1803-7.
42. Martin N, Wingfield J. USPSTF screening recommendations for breast cancer: the potential impact on the African American community. J Health Care Poor Underserved 2012;23(2 Suppl):91-7.
43. Jorgensen KJ, Gotzsche PC. Presentation on websites of possible
benefits and harms from screening for breast cancer: cross sectional study. BMJ 2004;328:148.
44. Gotzsche PC, Jorgensen KJ. The breast screening programme and misinforming the public. J R Soc Med 2011;104:361-9.
45. Kerlikowske K. Screening mammography in women less than age 50 years. Curr Opin Obstet Gynecol 2012;24:38-43.
46. Kirwan CC. Breast cancer screening: what does the future hold?
BMJ 2013;346:f87.