www.jkfas.org 있으며 각각 그 장단점이 보고되고 있다.1-6) 그 중 최소 침습적 수 술은 1990년 Bösch 등7)에 의해 시작되었는데, 특히 최소 절개를 이 용한 원위 중족골 절골술은 경도 및 중등도의 무지 외반증에 유용 한 술식으로 알려져 있다.8-11) 그러나 Kadakia 등12)이 이 술식은 높 은 재발률 및 부정유합 빈도를 보인다고 보고하였으며, 특히 중등 도 이상의 무지 외반증에서 최소 절개를 이용한 원위 중족골 절골 술을 시행한 결과에 대한 보고는 저자에 따라 이견이 있다.13,14) 이에 저자는 중등도 이상의 무지 외반증 환자에서 최소 절개를 이용한 원위 중족골 절골술의 방사선학적 및 임상적 결과를 분석하였다.
서 론
무지 외반증에 대한 수술적 치료 방법으로는 130여 가지 이상이
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/CC
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright 2015 Korean Foot and Ankle Society. All rights reserved.ⓒ
Purpose: Minimal incision distal metatarsal osteotomy (MIDMO) is known to be an effective surgical procedure for mild to moderate
hallux valgus. However, the result of MIDMO on moderate to severe hallux valgus is controversial; therefore, we investigated the radio- logical and clinical results of MIDMO on moderate to severe hallux valgus.Materials and Methods: We reviewed 51 feet (48 patients) with moderate to severe hallux valgus. The mean age was 67.0 years and
the mean follow-up period was 32.2 months. Radiological data of hallux valgus angle, first intermetatarsal angle, and distal metatarsal articular angle on plain radiographs were analyzed. Recurrence, union, lateral translation of distal fragment and angulation were also analyzed. The clinical data were obtained using American Orthopaedic Foot and Ankle Society (AOFAS) score of preoperation and last follow-up. Receiver operating characteristic (ROC) curve was used to determine a cut-off value.Results: The mean hallux valgus angle measured at preoperation was 37.7
o and 15.9o at last follow-up. The mean first intermetatarsal angle of preoperation and last follow-up were 15.2o and 8.3o. The mean distal metatarsal articular angle changed from 12.6o at preopera- tion to 7.8o at last follow-up. Preoperative hallux valgus angle (p=0.0051) and distal metatarsal articular angle (p=0.0078) were statisti- cally significant factors affecting postoperative AOFAS score. Cut-off value of each was 37o and 13o, respectively. Lateral translation of distal fragment in 5 recurrent cases was 23.0% compared to 45.3% of 46 non-recurrent cases. The result was statistically significant and the cut-off value was 38%.Conclusion: Sufficient lateral translation over 38% in MIDMO on moderate to severe hallux valgus patients with preoperative hallux
valgus angle under 37° and distal metatarsal articular angle under 13° can lead to good clinical results without recurrence.Key Words: Moderate to severe hallux valgus, Minimal incision, Distal metatarsal osteotomy
중등도 이상의 무지 외반증에서
최소 절개를 이용한 원위 중족골 절골술의 결과
허정욱, 은일수, 고영철, 박만준, 박숙현
부산의료원 정형외과
Results of Minimal Incision Distal Metatarsal Osteotomy for Moderate to Severe Hallux Valgus
Jung-Wook Huh, Il-Soo Eun, Young-Chul Ko, Man-Jun Park, Sook-Hyun Park
Department of Orthopedic Surgery, Busan Medical Center, Busan, Korea
Received April 6, 2015 Revised April 25, 2015 Accepted April 27, 2015 Corresponding Author: Il-Soo Eun
Department of Orthopedic Surgery, Busan Medical Center, 359 Worldcup-daero, Yeonje-gu, Busan 611-706, Korea
Tel: 82-51-507-3000, Fax: 82-51-507-3001, E-mail: [email protected] Financial support: None.
Conflict of interest: None.
로 원위 골편을 외측으로 충분히 전위시키고 전위된 골편을 2 mm 의 K-강선으로 고정하였다. 고정 방법은 절골된 골편의 내측에서 시작하여 제 1중족골의 골두와 무지의 내측 면을 따라 무지의 조갑 내측 모서리 약 2 mm 내측으로 K-강선을 후향적 방향으로 삽입한 후, K-강선을 다시 전향적 방향으로 중족골의 골수강 내로 진입시 켜 중족골의 근위부까지 도달하여 고정시켰다(Fig. 2). 이때 중족 골두의 각변형 및 회전변형을 방지하기 위해 K-강선 고정 전 절골 면의 상하연을 확인하여 정렬이 일치함을 확인 후 고정하였다. K- 강선을 고정하고 무지 외반각은 ―10o까지 과교정되도록 하였다 (Fig. 3). 모든 예에서 연부조직 술식 등의 다른 부가적인 시술은 시 행하지 않았다. 수술 후 처치는 제 1물갈퀴공간에 거즈를 충전하 고 단하지 부목을 시행한 상태로 발뒤꿈치를 이용한 보행을 허용 하였다. 수술 6∼7주 후에 K-강선을 제거하고 이후에도 제 1물갈 퀴공간에 거즈 충전을 2주간 더 시행하였다. 핀 주위 및 절개 부위 소독은 이틀마다 시행하였으며, 예방적 항생제는 수술 후 1주간 정 맥 투여하였다.
3. 평가
본 연구는 후향적 연구로서 결과에 대한 평가는 방사선학적 평 가, 임상적 평가로 나누어 시행하였다. 방사선학적 평가는 수술 전, 수술 직후, 수술 후 핀 제거 시, 추시 3개월, 추시 6개월, 추시 1 년 및 최종 추시 시의 족부 단순 방사선 사진에서 무지 외반각과 제 1∼2 중족골간 각 및 원위 중족골 관절면 각을 분석하였다. 수 술 후 재발, 유합, 원위 골편의 외측 전위 정도 및 시상면상 각변형
대상 및 방법
1. 연구 대상
본 연구는 부산의료원에서 2005년 8월부터 2012년 12월까지, 무 지 외반각이 30o 이상인 중등도 이상의 무지 외반증으로 최소 절개 를 이용한 원위 중족골 절골술을 시행하고 최소 1년 이상 추시가 가능하였던 48명의 환자 51예를 대상으로 하였다. 수술은 단일 술 자(I.S.E)에 의해 시행되었으며 무지 강직증이 있거나 이전에 무지 에 수술적 치료를 받은 환자, 그리고 제 1중족 족지 관절의 심한 퇴 행성 질환이 있는 경우는 제외하였다. 남자가 3명, 여자가 45명이 었고, 평균 연령은 67.0세(41∼78세)였으며, 평균 추시 기간은 32.2 개월(12∼65개월)이었다. 본 연구는 부산의료원의 임상연구윤리 위원회(institutional review board)로부터 승인을 받았다.
2. 수술 방법 및 수술 후 처치
척추 마취 후 환자를 앙와위의 자세로 한 후 C형 투시 장치를 이 용하여 제 1중족 족지 관절과 절골술을 시행할 부위를 표시하였 다. 절골술은 중족골의 골두하 지역에서 시행하였으며 이 절골술 부위를 중심으로 2 cm의 종적 피부 절개를 시행한 후 피부와 피하 조직을 박리하고 관절낭을 절개하여 절골 부위를 노출시켰다(Fig.
1). 이후 소형 호만 견인기(Hohmann retractor) 등으로 공간을 확 보하고 작은 전기톱으로 절골술을 시행하였으며, 절골술은 중족 골 골두의 약간 근위부에서 시상면상 제 1중족골의 간부에 수직하 는 단면으로 선상 절골을 시행하였다. 선상 절골 후 90o 겸자 등으
M-P joint M-P joint
Osteotomy site Osteotomy site
Skin incision 2 cm Skin incision 2 cm Skin incision 2 cm
Skin incision 2 cm M-P joint
Osteotomy site Osteotomy site
Osteotomy site
Skin incision 2 cm Skin incision 2 cm
M-P joint
Osteotomy site
Figure 1.
Figure 1. The lines are osteotomy site and skin incision line of minimal incision distal metatarsal osteotomy. M-P joint: meta- tarsophalangeal joint.
Figure 2.
Figure 2. After inserting Kirschner wire from the incision site into the soft tissue of hallus in proximal-todistal direction along the axis, insert the Kirschner wire in the opposite direction.
www.jkfas.org
결 과
무지 외반각은 수술 전 평균 37.7o (30.0o∼50.5o)였고, 최종 추 시 시 평균 15.9o (7.5o∼29.0o)로 약 21.8o 교정되었다. 수술 6∼7주 후 핀 제거 시 무지 외반각은 8.6o (―5o∼21o)로 핀 제거 후 평균 약 7.3o 정도 교정 소실이 발생하였다. 제 1∼2중족골간 각은 수술 전 평균 15.2o (9.5o∼18.0o)에서 최종 추시 시 평균 8.3o (1.0o∼11.6o) 로 약 6.9o 교정되었으며, 원위 중족골 관절면 각은 수술 전 평균 12.6o (5.0o∼22.0o), 최종 추시 시 평균 7.8o (1.0o∼13.6o)로 약 4.8o 교정된 것으로 측정되었다(Table 1).
AOFAS 점수는 수술 전 평균 58.9점(44∼79점), 최종 추시 시 평 균 83.9점(70∼96점)이었다. 합병증으로는 재발 5예(9.8%), 원위 골편의 족배 굴곡 6예(11.8%), 족저 굴곡 2예(3.9%), 제 1중족지 관 절의 강직 3예(5.9%), 수술 부위의 이상 감각 1예(2%), 핀 삽입 부 위 감염 1예(2%)가 발생하였다. 원위 골편의 족배 굴곡 및 족저 굴 곡은 수술 후 시상면상 방사선 촬영에서 관찰하였고, 족저 굴곡이 심한 경우 보행 시 경도의 통증을 호소하였다. 심한 제 1중족지 관 절의 강직은 3예였으나, 일부에서 무지의 관절운동 범위의 경한 강 직이 관찰되었다. 기존의 원위부 갈매기형 절골술 등의 수술과 비 교하였을 때 핀 고정기간 동안 통증 및 불편감은 차이가 나지 않았다.
원위 골편의 외측 전위 정도는 평균 43.1% (5%∼71%)였고 최 을 평가하였으며 재발은 수술 후 무지 외반각 20o 이상으로 정의하
였다.13)
임상적 평가는 수술 전과 최종 추시 시의 American Orthopaedic Foot and Ankle Society (AOFAS) Hallux-Metatarsophalangeal- Interphalangeal scale을 이용하였으며 AOFAS 등급15)을 불량(AO- FAS 점수 70점 이하), 보통(71∼80점), 양호(81∼90점), 우수(91점 이상)로 구분하여 평가하였고, AOFAS 등급 양호 이상은 임상적 결 과가 좋은 것으로 판단하였다.
통계 분석에는 PASW Statistics version 18.0 (IBM Co., Armonk, NY, USA) 프로그램을 사용하였다. 수술 전, 후 무지 외반각, 제 1∼
2중족골간 각, 원위 중족골 관절면 각, 원위 골편의 외측 전위 정 도, 시상면상 각변형 등과 수술 후 재발 및 AOFAS 점수의 관련성 을 paired t-test 및 로지스틱 회귀분석(logistic regression analysis) 을 수행하였으며 p<0.05인 경우를 통계적으로 유의한 것으로 판정 하였다. 통계적 유의성을 보인 항목의 cut-off value를 구하기 위해 receiver operating characteristic (ROC) curve를 이용하여 그 curve 에서 area under the curve와 민감도와 특이도의 합이 가장 큰 적정 cut-off value를 구하였다.
Figure 3.
Figure 3. The left foot of 59-year-old female was treated with minimal incision distal metatarsal osteotomy. Antero- posterior radiograph of preoperative (A), postoperative (B), and last follow-up (C).
B
A C
Table 1.
Table 1. Radiologic Data after Minimal Incision Distal Metatarsal Osteotomy
Angle (o) Preoperative Postoperative After pin removal
Follow-up Last
follow-up
3 mo 6 mo 1 yr
HVA 37.7 ―2.8 8.6 12.8 14.7 15.5 15.9
IMA 15.2 4.2 5.8 6.0 6.3 6.4 8.3
DMAA 12.6 1.1 4.1 6.6 7.9 8.5 7.8
Values are presented as mean.
HVA: hallux valgus angle, IMA: intermetatarsal angle, DMAA: distal metatarsal articular angle.
의한 차이를 보이는 인자는 외측 전위 정도 외에는 없었다.
본 연구에서는 AOFAS 등급 양호 이상(81점 이상)을 기준으로 한 로지스틱 회귀 분석상, 수술 후 AOFAS 점수에 영향을 주는 인 자로 수술 전 무지 외반각(p=0.0051)과 수술 전 원위 중족골 관절 대 71%까지 외측 전위시킨 예도 있었으며 전 예에서 골 유합을 얻
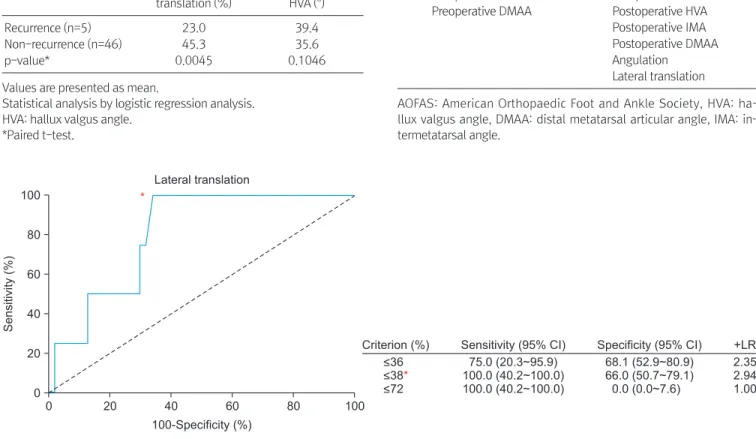
었고 재발률은 9.8%였다. 재발한 5예의 군에서 원위 골편의 외측 전위 정도는 평균 23.0%로 재발하지 않은 군의 평균 45.3%와 비 교하였을 때 통계적으로 유의한 차이가 있었다(p=0.0045; Table 2). ROC curve를 이용한 cut-off value는 원위 골편 외측 전위 정도 38%로 측정되었다(Fig. 4). 재발한 군과 재발하지 않은 군에서 유
Figure 5.
Figure 5. Receiver operating characteristic curve of American Orthopaedic Foot and Ankle Society score and preoperative hallux valgus angle (HVA) is shown that 37o is proposed as cut-off value. CI: confidence interval, +LR: positive likelihood ratio.
0 20 40 60 80
100 80 60 40 20
100
Sensitivity(%)
100-Specificity (%) 0
HVA
Sensitivity (95% CI) 91.7 (61.5~98.6) 91.7 (61.5~98.6) 83.3 (51.6~97.4)
Specificity (95% CI) 30.8 (17.0~47.6) 71.8 (55.1~85.0) 71.8 (55.1~85.0)
+LR 1.323.25 2.95
*
Criterion (%)
<33.4
<37*
<37.5 Table 2.
Table 2. Comparison of Recurrence and Non-recurrence Group Lateral
translation (%)
Mean preoperative HVA (o)
Recurrence (n=5) 23.0 39.4
Non-recurrence (n=46) 45.3 35.6
p-value* 0.0045 0.1046
Values are presented as mean.
Statistical analysis by logistic regression analysis.
HVA: hallux valgus angle.
*Paired t-test.
0 20 40 60 80
100 80 60 40 20
100
Sensitivity(%)
100-Specificity (%) 0
Lateral translation
Criterion (%)
<36
<38*
<72
Sensitivity (95% CI) 75.0 (20.3~95.9) 100.0 (40.2~100.0) 100.0 (40.2~100.0)
Specificity (95% CI) 68.1 (52.9~80.9) 66.0 (50.7~79.1)
0.0 (0.0~7.6)
+LR 2.352.94 1.00
*
Figure 4.
Figure 4. Receiver operating characteristic curve of recurrence and lateral translation is shown that 38% is proposed as cut-off value. CI: confidence interval, +LR: positive likelihood ratio.
Table 3.
Table 3. Factors Affecting and Not Affecting AOFAS Score in Minimal Incision Distal Metatarsal Osteotomy
Factors affecting AOFAS score
Factors not affecting AOFAS score Preoperative HVA Preoperative IMA Preoperative DMAA Postoperative HVA
Postoperative IMA Postoperative DMAA Angulation Lateral translation
AOFAS: American Orthopaedic Foot and Ankle Society, HVA: ha- llux valgus angle, DMAA: distal metatarsal articular angle, IMA: in- termetatarsal angle.
www.jkfas.org 을 발생시킬 수 있으나 임상적 결과에는 큰 영향을 미치지 않는다 고 보고하였다.
원위부 갈매기형 절골술을 이용한 무지 외반증의 교정은 경 도 및 중등도 무지 외반증에서 유용하다고 알려져 있으나,23) San- hudo24)에 의하면 절골각을 줄여 절골부의 안정성을 크게 하고 원 위 골편의 외측 전위를 더 크게 하면 중증의 무지 외반증에서도 원 위부 갈매기형 절골술을 시행할 수 있다고 하였다. 최소 절개를 이 용한 원위 중족골 절골술을 시행한 본 연구에서는 51예의 무지 외 반증 중 5예에서 수술 후 무지 외반각 20o 이상으로 재발을 하였는 데 원위 골편의 외측 전위 정도가 재발과 관련 있는 것으로 관찰되 었고(p=0.0045) ROC curve를 이용한 cut-off value는 원위 골편 외 측 전위 정도 38%로 측정되었으며(Fig. 4) 이는 중등도 이상의 무 지 외반증에서 수술 중 38% 이상의 충분한 원위 골편 외측 전위를 시행하였을 경우 수술 후 재발을 줄일 수 있음을 보여준다. 원위 골편의 외측 전위 정도 외에도 무지 외반증의 수술 후 재발에는 다 양한 원인들이 영향을 끼친다고 보고되고 있는데, 제 1∼2중족골 간 각, 원위 중족골 관절면 각, 무지 외반각과 종자골의 부족한 교 정은 잘 알려진 무지 외반증의 재발 요인이다.25-28) 본 연구에서 수 술 전 무지 외반각 등은 재발과 관련하여 통계적으로 유의한 차이 가 없었다(p=0.1046; Table 2). 또한 충분한 원위 골편의 외측 전위 는 추가적인 연부조직 술식 없이도 만족할 만한 무지 외반각의 교 정을 얻을 수 있게 하였다. Magnan 등11)은 최소 절개를 이용한 원 위 중족골 절골술에서 연부조직 술식을 시행하지 않더라도 재발률 이 높지 않았다고 보고하였으며, Kadakia 등12)은 연부조직 술식을 최소화함으로써 혈관손상의 위험을 줄여 골 유합률을 높일 수 있 다고 보고하였다.
Deenik 등29)은 136예의 무지 외반증에 대해 원위부 갈매기형 절 골술 70예, 스카프 절골술 66예를 시행하여 분석한 결과, 수술 후 방사선학적 및 임상적 결과에 영향을 미치는 인자는 수술 전 무 면 각(p=0.0078)이 통계적으로 유의한 차이를 보였다(Table 3).
ROC curve를 이용한 cut-off value는 수술 전 무지 외반각 37o, 수술 전 원위 중족골 관절면 각 13o로 측정되었다(Fig. 5, 6).
고 찰
무지 외반증의 수술적 치료 방법으로는 연부조직 재건술, 제 1 중족골 원위부 절골술, 제 1중족골 근위부 절골술, 족무지 근위 지 골 절골술, 제 1중족골 간부 절골술, 절제 관절 성형술, 관절 고정 술 등 여러 가지 방법들이 있으며 여러 문헌에서 각각의 수술법에 대한 추시 관찰에서 양호한 결과를 보고하고 있다.16-20) 하지만 명 확하고 널리 인정받는 하나의 치료 지침이 제시되고 있지 않은 상 황이다. 그 중 최소 절개를 이용한 원위 중족골 절골술은 고식적인 방법과 비슷한 수술 결과를 나타내면서도 수술 시간 단축, 간단한 술기, 저비용, 적은 합병증, 작은 절개 부위, 조기 체중부하가 가능 하다는 장점을 가지고 있다.21,22) 이러한 최소 절개를 이용한 원위 중족골 절골술은 경도 및 중등도의 무지 외반증에 유용한 술식으 로 알려져 있으나 중등도 및 중증의 무지 외반증 환자에서 최소 절 개를 이용한 원위부 중족골 절골술의 유용성 여부는 이견이 있다.
Huang 등13)은 수술 전 무지 외반각이 30o 이하인 무지 외반증 환자 (89예)와 30o 이상인 환자(36예)에서 최소 절개를 이용한 원위 중 족골 절골술을 시행하였으며 무지 외반각이 30o 이하인 그룹에서 재발 및 부정유합이 6.7%, 30o 이상인 그룹에서 63.9% 발생하여, 무지 외반각이 30o 이상인 경우 최소 절개를 이용한 원위 중족골 절골술을 시행하지 않기를 권하였다. 반면 Angthong 등14)은 2예의 경도의 무지 외반증 환자를 포함하여 무지 외반증 36예에 대해 최 소 절개를 이용한 원위 중족골 절골술을 시행하였으며, 그 결과 중 등도의 무지 외반증 환자에서 최소 절개를 이용한 원위 중족골 절 골술을 시행하였을 때 방사선학적으로 시상면상 부정유합 및 재발 Figure 6.
Figure 6. Receiver operating characteristic curve of American Orthopaedic Foot and Ankle Society score and preoperative distal metatarsal articular angle (DMAA) is shown that 13o is proposed as cut-off value. CI: confidence interval, +LR: positive likelihood ratio.
0 20 40 60 80
100 80 60 40 20
100
Sensitivity(%)
100-Specificity (%) 0
DMAA
Sensitivity (95% CI) 75.0 (42.8~94.2) 83.3 (51.6~97.4) 83.3 (51.6~97.4)
Specificity (95% CI) 66.7 (49.8~80.9) 64.1 (47.2~78.8) 51.3 (34.8~67.6)
+LR 2.252.32 1.71
*
Criterion ( )o
<12
<13*
<14
7. Bösch P, Markowski H, Rannicher V. Technik und erste ergeb- nisse der subkutanen distalen metatarsale-I-osteotomie. Orthop Praxis. 1990;26:51-6.
8. Faour-Martín O, Martín-Ferrero MA, Valverde García JA, Vega- Castrillo A, de la Red-Gallego MA. Long-term results of the ret- rocapital metatarsal percutaneous osteotomy for hallux valgus.
Int Orthop. 2013;37:1799-803.
9. Bösch P, Wanke S, Legenstein R. Hallux valgus correction by the method of Bösch: a new technique with a seven-to-ten-year follow-up. Foot Ankle Clin. 2000;5:485-98.
10. Kissel CG, Unroe BJ, Parker RM. The offset "V" bunionectomy using cortical screw and buried Kirschner wire fixation. J Foot Surg. 1992;31:560-77.
11. Magnan B, Pezzè L, Rossi N, Bartolozzi P. Percutaneous distal metatarsal osteotomy for correction of hallux valgus. J Bone Joint Surg Am. 2005;87:1191-9.
12. Kadakia AR, Smerek JP, Myerson MS. Radiographic results after percutaneous distal metatarsal osteotomy for correction of hal- lux valgus deformity. Foot Ankle Int. 2007;28:355-60.
13. Huang PJ, Lin YC, Fu YC, Yang YH, Cheng YM. Radiographic evaluation of minimally invasive distal metatarsal osteotomy for hallux valgus. Foot Ankle Int. 2011;32:S503-7.
14. Angthong C, Yoshimura I, Kanazawa K, Hagio T, Ida T, Naito M.
Minimally invasive distal linear metatarsal osteotomy for cor- rection of hallux valgus: a preliminary study of clinical outcome and analytical radiographic results via a mapping system. Arch Orthop Trauma Surg. 2013;133:321-31.
15. Ozan F, Bora OA, Filiz MA, Kement Z. Interposition arthroplasty in the treatment of hallux rigidus. Acta Orthop Traumatol Turc.
2010;44:143-51.
16. Hawkins FB, Mitchell CL, Hedrick DW. Correction of hallux valgus by metatarsal osteotomy. J Bone Joint Surg Am. 1945;
27:387-94.
17. Mann RA, Coughlin MJ. Hallux valgus--etiology, anatomy, treat- ment and surgical considerations. Clin Orthop Relat Res. 1981;
(157):31-41.
18. Shapiro F, Heller L. The Mitchell distal metatarsal osteotomy in the treatment of hallux valgus. Clin Orthop Relat Res. 1975;
(107):225-31.
19. Trnka HJ, Zembsch A, Easley ME, Salzer M, Ritschl P, Myerson MS. The chevron osteotomy for correction of hallux valgus.
Comparison of findings after two and five years of follow-up. J Bone Joint Surg Am. 2000;82:1373-8.
20. Wu KK. Wu's bunionectomy: a clinical analysis of 150 personal cases. J Foot Surg. 1992;31:288-97.
21. Giannini S, Faldini C, Nanni M, Di Martino A, Luciani D, Vannini F.
A minimally invasive technique for surgical treatment of hallux valgus: simple, effective, rapid, inexpensive (SERI). Int Orthop.
2013;37:1805-13.
22. Portaluri M. Hallux valgus correction by the method of Bösch: a clinical evaluation. Foot Ankle Clin. 2000;5:499-511.
23. Mann RA, Donatto KC. The chevron osteotomy: a clinical and radiographic analysis. Foot Ankle Int. 1997;18:255-61.
24. Sanhudo JA. Extending the indications for distal chevron oste- otomy. Foot Ankle Int. 2000;21:522-3.
25. Bonnel F, Canovas F, Poirée G, Dusserre F, Vergnes C. Evaluation 지 외반각이며 그 각이 37o 이상일 경우 교정률이 낮아진다고 보
고하였다. 반면 제 1∼2중족골간 각 및 원위 중족골 관절면 각 등 은 큰 영향을 미치지 않는다고 하였다. 본 연구에서는 무지 외반각 30o 이상인 중등도 이상의 무지 외반증 환자에게 최소 절개를 이용 한 원위 중족골 절골술을 시행하였으며 AOFAS 점수는 수술 전 평 균 58.9점(44∼79점), 최종 추시 시 평균 83.9점(70∼96점)이었다.
AOFAS 점수에 영향을 주는 인자는 수술 전 무지 외반각이 통계적 으로 유의한 차이가 있었으며(p=0.0051), cut-off value는 37o로 측 정되어(Fig. 5) Deenik 등29)의 연구와 같은 수치를 보였다. 한편 본 연구에서는 수술 전 원위 중족골 관절면 각 역시 수술 후 AOFAS 점수에 영향을 미치는 것으로 관찰되었으며(p=0.0078) cut-off value는 13o였다(Fig. 6). 이는 37o 이상의 무지 외반각을 가지거나 13o 이상의 원위 중족골 관절면 각을 가진 환자에서 최소 절개를 이용한 원위부 중족골 절골술을 시행하였을 때 임상적 결과가 좋 지 않음을 보여준다.
본 연구의 제한점으로는 증례수가 다소 적고, 무지 외반각 30o 이하인 무지 외반증 환자와의 비교가 없으며 심한 원위 중족골 관 절면 각을 가지는 예가 적다는 점과 골관절염 여부나 제 1중족골의 길이, 종자골의 위치를 고려하지 않았다는 점이다. 좀 더 많은 수 의 환자를 대상으로 한 전향적 연구가 필요할 것으로 생각된다.
결 론
중등도 이상의 무지 외반증 환자에게 최소 절개를 이용한 원위 중족골 절골술을 시행할 때 수술 전 무지 외반각이 37o 이하이고 수술 전 원위 중족골 관절면 각이 13o 이하인 환자들에서 38% 이상 의 충분한 외측 전위를 시행하면 재발 없이 우수한 임상 결과를 얻 을 수 있을 것으로 생각된다.
REFERENCES
1. Robinson AH, Limbers JP. Modern concepts in the treatment of hallux valgus. J Bone Joint Surg Br. 2005;87:1038-45.
2. Radwan YA, Mansour AM. Percutaneous distal metatarsal oste- otomy versus distal chevron osteotomy for correction of mild- to-moderate hallux valgus deformity. Arch Orthop Trauma Surg.
2012;132:1539-46.
3. Borton DC, Stephens MM. Basal metatarsal osteotomy for hallux valgus. J Bone Joint Surg Br. 1994;76:204-9.
4. Coughlin MJ, Grebing BR, Jones CP. Arthrodesis of the first metatarsophalangeal joint for idiopathic hallux valgus: interme- diate results. Foot Ankle Int. 2005;26:783-92.
5. Klosok JK, Pring DJ, Jessop JH, Maffulli N. Chevron or Wilson metatarsal osteotomy for hallux valgus. A prospective random- ised trial. J Bone Joint Surg Br. 1993;75:825-9.
6. Sammarco GJ, Brainard BJ, Sammarco VJ. Bunion correction us- ing proximal Chevron osteotomy. Foot Ankle. 1993;14:8-14.
www.jkfas.org factor for recurrence of hallux valgus. J Bone Joint Surg Am.
2009;91:1637-45.
28. Veri JP, Pirani SP, Claridge R. Crescentic proximal metatarsal os- teotomy for moderate to severe hallux valgus: a mean 12.2 year follow-up study. Foot Ankle Int. 2001;22:817-22.
29. Deenik AR, de Visser E, Louwerens JW, de Waal Malefijt M, Drai- jer FF, de Bie RA. Hallux valgus angle as main predictor for cor- rection of hallux valgus. BMC Musculoskelet Disord. 2008;9:70.
of the Scarf osteotomy in hallux valgus related to distal metatar- sal articular angle: a prospective study of 79 operated cases. Rev Chir Orthop Reparatrice Appar Mot. 1999;85:381-6.
26. Pontious J, Mahan KT, Carter S. Characteristics of adolescent hallux abducto valgus. A retrospective review. J Am Podiatr Med Assoc. 1994;84:208-18.
27. Okuda R, Kinoshita M, Yasuda T, Jotoku T, Kitano N, Shima H.
Postoperative incomplete reduction of the sesamoids as a risk