J Korean Soc Radiol 2016;74(4):230-235 http://dx.doi.org/10.3348/jksr.2016.74.4.230
Distal Posterior Cerebral Artery Aneurysms: Retrospective Review of Characteristics and Endovascular Treatment
원위 후대뇌동맥 뇌동맥류: 특징과 혈관 내 치료에 대한 후향적 검토
Jin Wook Baek, MD
1,2, Won-Bae Seung, MD
3, Hae Woong Jeong, MD
2*
1Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
2Department of Diagnostic Radiology, Inje University College of Medicine, Busan Paik Hospital, Busan, Korea
3Department of Neurosurgery, Kosin University College of Medicine, Gospel Hospital, Busan, Korea
서론
후대뇌동맥(posterior cerebral artery)의 뇌동맥류는 전체 두 개 내 뇌동맥류의 0.7~2.3% 정도를 차지하는 드문 질환이며 (1-3), 다른 해부학적 위치에서 발견되는 뇌동맥류와 다른 몇 가지 특징을 가지고 있다(4-13). 상대적으로 이른 나이에 발견 되며(5, 14), 발견 당시 크기가 크고(14-16), 박리성 뇌동맥류의 비율이 높다(17-19). 후대뇌동맥에 발생한 뇌동맥류는 수술을 통해 직접 병변에 접근해 클립을 이용해 치료하는 방법과 혈관 내 치료를 통해 병변에 접근해 코일을 이용해 치료하는 방법 모 두가 가능하나, 수술적인 치료는 후대뇌동맥에 존재하는 수많 은 관통 가지들과 후대뇌동맥 자체가 해부학적으로 뇌신경들 과 상부 뇌간에 매우 근접해 있기 때문에 기술적으로 어렵다.
혈관 내 접근을 통한 치료의 경우는 수술에 비해 기술적으로 접근이 용이하며 일반적으로 관통 가지들을 보존하며 치료하는 것이 가능하므로 수술적 방법을 대체하기에 적합한 것으로 알 려져 있다(7). 본 연구에서는 혈관 내 치료를 이용해 P1 분절의 뇌동맥류를 제외한 원위 후대뇌동맥의 뇌동맥류를 치료한 사 례들을 통해 원위 후대뇌동맥 뇌동맥류의 치료에 혈관 내 치료 가 유용하게 사용될 수 있을지 알아보고자 한다.
대상과 방법
본 연구는 후향적 연구로 Institutional Review Board 승인은 기관에서 면제되었다.
2002년 12월에서 2013년 12월까지, 인제대학교 부산백병원 Purpose: The objective of this study was to review the clinical outcome after treat-
ment of distal posterior cerebral artery (PCA) aneurysms via endovascular approach.
Materials and Methods: Eleven patients with 11 distal PCA aneurysms who were treated via endovascular approach in Inje University Busan Paik Hospital and Kosin University Gospel Hospital from December 2002 to December 2013 were retrospec- tively reviewed.
Results: Among the 11 patients, there were 3 males (27.3%) and 8 females (72.7%).
The mean age was 56.6 years (range 44–72 years) and the mean aneurysm size was 8.45 mm (3–30 mm). Four (36.4%) aneurysms were located in the P2 segment, 6 (54.5%) in the P3 segment and 1 (9.1%) in the P1/2 junction. Seven (63.6%) aneu- rysms were treated with preservation of the parent artery; and the remaining 4 (36.4%) aneurysms were treated with parent artery occlusion. After treatment, the overall complication rate was 27% with the morbidity rate of 9.1% and the mortali- ty rate of 18%.
Conclusion: Endovascular treatment of distal PCA aneurysm might be used to minimize neurologic deficit, considering the diverse and rich collaterals of posterior cerebral artery.
Index terms Aneurysm
Posterior Cerebral Artery Endovascular Techniques
Received July 27, 2015 Revised October 26, 2015 Accepted November 26, 2015
*Corresponding author: Hae Woong Jeong, MD Department of Diagnostic Radiology, Inje University College of Medicine, Busan Paik Hospital, 75 Bokji-ro, Busanjin-gu, Busan 47392, Korea.
Tel. 82-51-890-6547 Fax. 82-51-896-1085 E-mail: [email protected]
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distri- bution, and reproduction in any medium, provided the original work is properly cited.
과 고신대학교 복음병원에서 후대뇌동맥의 뇌동맥류로 진단 및 치료받은 환자들 중, P1 분절에서 발견된 뇌동맥류를 제외한 원위 후대뇌동맥 뇌동맥류로 확인된 총 11명의 환자의 11개의 뇌동맥류를 대상으로 연구를 진행하였다. 11명의 환자들은 모 두 혈관 내 치료를 통한 치료를 시행하였다. 11명 환자에 대한 개별 정보와 뇌동맥류 초기 영상의학적 소견 및 특성, 각각의 뇌동맥류에 대한 치료 결과는 Table 1에 정리된 바와 같다.
모든 환자들은 내원 당시, 출혈 여부와 원인을 알아보기 위 해 전산화단층촬영(computed tomography)과 전산화단층혈관 촬영(computed tomography angiography)을 시행하였고, 이후 출혈 여부에 관계없이 원위 후대뇌동맥 뇌동맥류가 발견된 환 자들에 대해 진단목적의 대퇴동맥경유 뇌혈관조영술(trans- femoral cerebral angiography)을 시행하였다. 이 검사를 통해 뇌동맥류의 유형, 위치, 크기에 대해 분석하였다. 후대뇌동맥은 Ciceri 등(3)에 의해 제시된 방법에 따라 4개의 해부학적 분절 로 나누어 분류되었고 각각의 분절은 다음과 같다. P1 분절은 뇌바닥동맥갈림(tip of the basilar artery)에서부터 후교통동맥 (posterior communicating artery)의 시작 부분까지이며, P2 분 절은 후교통동맥의 시작부에서 중뇌(mid brain)의 후방 부분까 지로, 다시 앞쪽의 P2A 분절과 뒤쪽의 P2P 분절로 세분된다.
P3 분절은 후관자동맥(posterior temporal artery)이 기원하는 부분인 사구체수조(quadrigeminal cistern)의 외측 부분에서부 터 새발톱고랑(calcarine fissure)에 이르는 부분이다. 마지막으 로 P4 분절은 후대뇌동맥의 종말 겉질 가지(terminal cortical branches)들로 이루어져 있으며, 마루뒤통수동맥(parietooc- cipital artery)과 새발톱고랑동맥(calcarine artery)이 분지된 이 후의 부분이다. 이후 뇌동맥류의 유형에 따라 소낭성 뇌동맥류 의 경우 모체 동맥(parent artery)을 보존하며 선택적 뇌동맥류
색전술을 시행하였고 박리성 뇌동맥류의 경우 뇌동맥류와 동 시에 모체 동맥을 폐쇄하는 방법으로 치료를 시행하였다. 최종 적으로 환자의 치료 결과에 대해 변형 란킨 점수(modified Rankin Scale score)에 의해 평가하였다.
결과
연구에 포함된 총 11명 환자의 결과는 Table 1에 정리하였다.
연령 분포는 44세에서 72세였고, 평균연령은 56.6세였다. 남 자 환자가 3명(27.3%), 여자 환자가 8명(72.7%)으로 여자 환 자가 좀 더 많은 양상을 보였다. 내원 당시 시행한 전산화단층 촬영에서 11명의 환자 중 5명의 환자(45.4%)에서 거미막밑출 혈(subarachnoid hemorrhage)이 동반되어 있었고 2명의 환자 (18.2%)에서 두개 내 출혈(intracranial hemorrhage)을 동반하 였으며 출혈이 발견되지 않은 환자는 4명(36.4%)이었다. 11개 의 뇌동맥류 중 6개(54.5%)는 소낭성 뇌동맥류, 4개(36.4%) 는 박리성 뇌동맥류, 1개(9.1%)는 동정맥기형과 연관되어 박 리성과 소낭성이 동시에 나타난 유형(saccular with dissecting type)이었다. 각 뇌동맥류의 위치는 P2 분절이 4개(36.4%), P3 분절이 6개(54.5%)였으며, P1과 P2 분절의 경계에 위치한 경우가 1개(9.1%)였다. 전체 뇌동맥류의 크기는 3 mm에서 30 mm 사이로 측정되었고, 측정된 뇌동맥류 크기의 평균값은 8.45 mm였다. 7개의 소낭성 뇌동맥류(63.6%)에 대해 모체 동맥을 보존하며 선택적 뇌동맥류 색전술을 시행하였고, 4개 의 박리성 뇌동맥류(36.4%)에 대해 뇌동맥류와 동시에 모체 동맥을 폐쇄하는 방법으로 치료를 시행하였다(Figs. 1, 2). 전 체 11명 환자의 뇌동맥 색전술에 사용된 기술(technique), 코일 (coil)의 개수와 총 길이, 시술시간은 Table 2에 정리하였다. 치 Table 1. Data for Distal PCA Aneurysm in 11 Patients
Patient
Number Sex/Age (yr) Clinical Presentation
Aneurysm Clinical
Outcome
Location Type Size (mm) Treatment
1 M/56 SAH P2 Saccular 7 SCE mRS 0
2 F/56 ICH P3 Saccular 8 SCE mRS 0
3 F/61 Hemorrhage (-) P2 Saccular with dissecting 9 SCE mRS 0
4 F/65 Hemorrhage (-) P3 Saccular 3 SCE mRS 0
5 F/49 Hemorrhage (-) P2 Saccular 7 SCE mRS 0
6 F/65 Hemorrhage (-) P1-P2 Saccular 9 SCE mRS 0
7 M/44 ICH P3 Saccular 5 SCE Death
8 F/51 SAH P3 Dissecting 30 PAO mRS 0
9 M/45 SAH P2 Dissecting 5 PAO mRS 0
10 F/59 SAH, IVH P3 Dissecting 7 PAO mRS 4
11 F/72 SAH, IVH P3 Dissecting 3 PAO Death
ICH = intracranial hemorrhage, IVH = intraventricular hemorrhage, mRS = modified Rankin score, PAO = parent artery occlusion, PCA = posterior cerebral artery, SAH = subarachnoid hemorrhage, SCE = selective coil embolization
료 후 8명의 환자(72.7%)가 변형 란킨 점수가 0으로 특별한 신경학적 결손을 보이지 않았으며, 1명의 환자(9.1%)는 변형 란킨 점수가 4였고, 2명의 환자(18.2%)는 사망하였다.
고찰
이전의 다른 연구들에서 보고한 바에 따르면, 후대뇌동맥의
뇌동맥류는 해부학적으로 P1과 P2 분절과 같은 근위부에서 발 견되는 빈도가 더 많고(13), 후대뇌동맥 이외의 다른 해부학적인 위치에서 발견되는 뇌동맥류에 비해 더 어린 나이에 발견되며 (5, 14), 발견 당시의 크기가 큰 것으로 알려져 있다(14-16). 하 지만 본 연구에서 원위 후대뇌동맥의 뇌동맥류만을 대상으로 살펴본 결과, 발생 나이는 평균 56.6세로 다른 해부학적인 위 치에서 발견되는 뇌동맥류와 호발 연령에 큰 차이가 없었고, 한
Fig. 1. Successful embolization was done by using parent artery occlusion technique in a 59-year-old female who presented with subarachnoid and intraventricular hemorrhage (patient number 10 in Table 1).
A. Initial non-contrast enhanced computed tomography scan shows diffuse subarachnoid hemorrhage with bilateral intraventricular hemor- rhage.
B, C. The anteroposterior (B) and lateral (C) projection views of a left vertebral artery angiography show a fusiform dissecting aneurysm (arrow) with ruptured state in the left P3 segment.
D. Parent artery occlusion (arrow) technique was used for complete embolization.
A
C
B
D
개(9%)의 거대 뇌동맥류만이 발견되었다. 본 연구에서 이전의 연구 결과들과 다른 결과가 나온 것은 후대뇌동맥의 뇌동맥류 에서 가장 많은 빈도를 차지하는 P1 분절의 뇌동맥류를 제외한 원위부의 뇌동맥류만을 대상으로 연구를 진행하였기 때문에, 후대뇌동맥의 뇌동맥류를 대표하는 특징을 나타내기에 부족함 이 있으며, 연구에 포함된 뇌동맥류의 수가 적어 통계적 대표성 을 가질 수 없기 때문인 것으로 생각된다. 일반적으로 후대뇌동 맥의 뇌동맥류 환자는 거미막밑출혈을 주소로 내원하는 경우 가 가장 많으며(5, 18, 20), 이외에 뇌동맥류의 크기가 커지게 되면 주변 구조물들을 압박하게 되어 발생할 수 있는 시각장 애, 기억장애 또는 발작 등의 증상으로 내원하게 된다(21). 본
연구에서는 첫 내원 시 거미막밑출혈을 주소로 한 경우가 가장 많았다.
본 연구에 포함된 모든 환자는 혈관 내 치료를 받았으며, 7개 의 소낭성 뇌동맥류에 대해 모체 동맥을 보존하는 선택적 뇌동 맥류 색전술을 시행하였으나, 모체 동맥의 보존이 어려운 4개 의 박리성 뇌동맥류의 경우 동맥류와 동시에 모체 동맥을 폐쇄 하는 방법으로 치료를 하였다. 모체 동맥을 동시에 폐쇄하는 경우에도 시야결손 등의 합병증이 발생하는 빈도는 낮은 것으 로 알려져 있는데(3), 이는 외측 후맥락막동맥(lateral posterior choroidal artery)(P2 분절의 가지)과 전맥락막동맥(anterior choroidal artery)의 곁순환, 긴휘돌이동맥(long circumflex ar- tery)(P1 분절의 가지)과 위소뇌동맥(superior cerebellar ar- tery)의 곁순환, 뇌들보팽대동맥(splenial artery)(P3-P4 분절 의 가지)과 후뇌들보주위동맥(posterior pericallosal artery)[전 대뇌동맥(anterior cerebral artery)의 가지]의 곁순환, 후대뇌 동맥의 아래 관자 가지(inferior temporal branch)와 중대뇌동 맥(middle cerebral artery)의 위 관자 가지(superior temporal branch)의 곁순환 등 후대뇌동맥이 주변의 여러 다른 혈관들 과 다양하고 풍부한 해부학적 곁순환을 형성하기 때문인 것으 로 알려져 있다(3).
본 연구에서도 4명의 환자의 4개의 박리성 뇌동맥류에 대해 모체 동맥의 폐쇄를 시행하였으나 시술 후 특별한 합병증은 발 견되지 않았다. 하지만 일부 연구에 따르면, 근위부 후대뇌동 맥 또는 종말 후대뇌동맥부의 경우 곁순환의 도움을 받지 못 Table 2. Data for Used Technique and Materials for 11 Patients
Patient
Number Used Technique Number of Coils
Total Coil Length (cm)
Procedural Time (min)
1 Balloon assisted 7 93 230
2 Single microcatheter 9 27 160
3 Single microcatheter 12 128 170
4 Single microcatheter 2 5 215
5 Single microcatheter 5 22 80
6 Double microcatheter 21 238 200
7 Single microcatheter 4 20 130
8 Double microcatheter 5 60 120
9 Single microcatheter 5 40 185
10 Single microcatheter 6 23 280
11 Single microcatheter 2 6 135
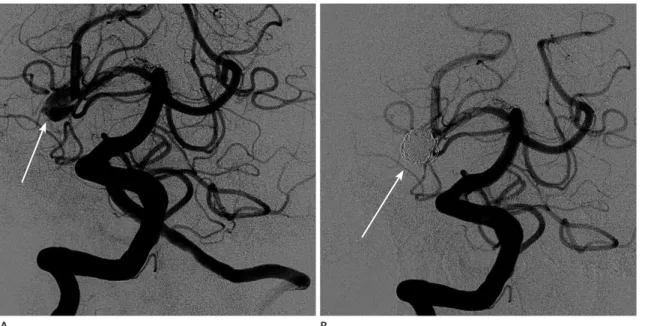
Fig. 2. A saccular dissecting aneurysm at the right P2 segment in a 61-year-old female patient who presented with headache (patient number 3 in Table 1).
A. The anteroposterior projection of right vertebral artery angiography shows a saccular dissecting aneurysm (arrow) in the right P2 segment.
B. After selective coil embolization, complete aneurysmal occlusion (arrow) was conducted without parent artery occlusion.
A B
해 뇌경색에 취약할 수 있으며(22), 합병증의 존재 유무와 관 계없이 다양한 뇌경색의 소견이 치료 후 관찰될 수 있다는 보고 가 있어(23), 비교적 치료 후 예후는 좋지만 치료 시 뇌경색이 발생할 가능성은 항상 염두에 두어야 할 것으로 생각된다.
본 연구에 포함된 11명의 환자들은 치료 후 8명의 환자에서 변형 란킨 점수가 0으로 특이할 만한 신경학적 결손은 발견되 지 않았으나, 1명의 환자에서 변형 란킨 점수 4, 2명의 환자는 사망하였다. 이전에 21개의 후대뇌동맥 뇌동맥류에 대해 선택 적 뇌동맥 색전술과 모체 동맥 폐쇄의 방법으로 치료하였던 기 존의 연구(3) 결과와 비교해 볼 때 유병률에 있어서는 유사한 결과를 보여주나(9.1% vs. 10%), 합병증 발생률과 사망률에 있어서 더 높은 결과를 나타내었다. 이는 기존에 출혈량이 많은 환자들이 좋지 않은 치료 결과를 나타낸 것에 의한 것으로 생 각된다. 변형 란킨 점수가 4인 환자와 1명의 사망 환자는 모두 초기 내원 단계에 이미 출혈량이 많고 상태가 좋지 않아 시술 이후에도 후유증이 남거나 사망한 것으로 생각된다. 나머지 1명 의 사망 환자는 내원 당시 많은 양의 혈종이 있어 감압두개절제 술(decompressive craniectomy) 시행 후 혈관 내 치료를 시행 한 환자로 시술 중 뇌동맥류가 다시 파열되어 시술 후 3일째 사 망한 사례이다. 본 연구는 원위부 후대뇌동맥의 다양하고 풍부 한 곁순환으로 인해 모체 동맥의 폐쇄가 필요한 박리성 뇌동맥 류의 경우에도 혈관 내 치료가 적절한 치료 방법이 될 수 있다 는 점을 보여준다.
결론적으로, 원위 후대뇌동맥 뇌동맥류의 혈관 내 치료는 모 체 동맥을 보존하는 경우뿐만 아니라 폐쇄하는 경우에 있어서 도 후대뇌동맥 특유의 다양하고 풍부한 곁순환을 고려하여 치 료방침을 정한다면 신경학적 결손을 최소화하는 치료법으로 사 용될 수 있다.
REFERENCES
1. Honda M, Tsutsumi K, Yokoyama H, Yonekura M, Nagata I.
Aneurysms of the posterior cerebral artery: retrospective review of surgical treatment. Neurol Med Chir (Tokyo) 2004;44:164-168; discussion 169
2. Chang HS, Fukushima T, Takakura K, Shimizu T. Aneurysms of the posterior cerebral artery: report of ten cases. Neu-
rosurgery 1986;19:1006-1011
3. Ciceri EF, Klucznik RP, Grossman RG, Rose JE, Mawad ME.
Aneurysms of the posterior cerebral artery: classification and endovascular treatment. AJNR Am J Neuroradiol 2001;22:27-34
4. Drake CG, Amacher AL. Aneurysms of the posterior cere- bral artery. J Neurosurg 1969;30:468-474
5. Ferrante L, Acqui M, Trillò G, Lunardi P, Fortuna A. Aneu- rysms of the posterior cerebral artery: do they present specific characteristics? Acta Neurochir (Wien) 1996;138:
840-852
6. Gerber CJ, Neil-Dwyer G, Evans BT. An alternative surgical approach to aneurysms of the posterior cerebral artery.
Neurosurgery 1993;32:928-931; discussion 931
7. Guglielmi G, Viñuela F, Duckwiler G, Dion J, Lylyk P, Beren- stein A, et al. Endovascular treatment of posterior circula- tion aneurysms by electrothrombosis using electrically de- tachable coils. J Neurosurg 1992;77:515-524
8. Hallacq P, Piotin M, Moret J. Endovascular occlusion of the posterior cerebral artery for the treatment of p2 seg- ment aneurysms: retrospective review of a 10-year series.
AJNR Am J Neuroradiol 2002;23:1128-1136
9. Orita T, Tsurutani T, Izumihara A, Kajiwara K. Distal poste- rior cerebral artery aneurysms--three case reports. Neurol
Med Chir (Tokyo) 1994;34:692-696
10. Sakata S, Fujii K, Matsushima T, Fujiwara S, Fukui M, Mat- subara T, et al. Aneurysm of the posterior cerebral artery:
report of eleven cases--surgical approaches and proce- dures. Neurosurgery 1993;32:163-167; discussion 167-168 11. Seoane ER, Tedeschi H, de Oliveira E, Siqueira MG, Calderón
GA, Rhoton AL Jr. Management strategies for posterior ce- rebral artery aneurysms: a proposed new surgical classifi- cation. Acta Neurochir (Wien) 1997;139:325-331
12. Terasaka S, Sawamura Y, Kamiyama H, Fukushima T. Surgi- cal approaches for the treatment of aneurysms on the P2 segment of the posterior cerebral artery. Neurosurgery 2000;47:359-364; discussion 364-366
13. Zeal AA, Rhoton AL Jr. Microsurgical anatomy of the pos- terior cerebral artery. J Neurosurg 1978;48:534-559 14. Scholten FG, ter Berg HW, Hofstee N, Vellenga CJ. Giant
aneurysm of the posterior cerebral artery in a one-year- old child. Eur J Radiol 1992;15:56-58
15. de Sousa AA, Dantas FL, Neto AP, Carvalho GT. Giant pos- terior cerebral artery aneurysm in a 4-year-old child: case report. Surg Neurol 1996;45:31-35
16. Lempert TE, Halbach VV, Higashida RT, Dowd CF, Urwin RW, Balousek PA, et al. Endovascular treatment of pseu-
doaneurysms with electrolytically detachable coils. AJNR
Am J Neuroradiol 1998;19:907-911
17. Lazinski D, Willinsky RA, TerBrugge K, Montanera W. Dis- secting aneurysms of the posterior cerebral artery: angio- architecture and a review of the literature. Neuroradiology 2000;42:128-133
18. Pia HW, Fontana H. Aneurysms of the posterior cerebral ar- tery. Locations and clinical pictures. Acta Neurochir (Wien) 1977;38:13-35
19. Sasaki O, Koizumi T, Ito Y, Sorimachi T, Koike T, Tanaka R.
Dissecting aneurysm of the posterior cerebral artery treat- ed with proximal ligation. Surg Neurol 1992;37:394-401 20. Gerber CJ, Neil-Dwyer G. A review of the management of
15 cases of aneurysms of the posterior cerebral artery. Br J
Neurosurg 1992;6:521-527
21. Yacubian EM, Rosemberg S, da Silva HC, Jorge CL, de Olivei- ra E, de Assis LM. Intractable complex partial seizures as- sociated with posterior cerebral artery giant aneurysm: a case report. Epilepsia 1994;35:1317-1320
22. Kim YB, Lee JW, Huh SK, Kim BM, Kim DJ. Outcomes of multidisciplinary treatment for posterior cerebral artery aneurysms. Clin Neurol Neurosurg 2013;115:2062-2068 23. Roh HG, Kim SS, Han H, Kang HS, Moon WJ, Byun HS. En-
dovascular treatment of posterior cerebral artery aneu- rysms using detachable coils. Neuroradiology 2008;50:
237-242
원위 후대뇌동맥 뇌동맥류: 특징과 혈관 내 치료에 대한 후향적 검토
백진욱
1,2· 승원배
3· 정해웅
2*
목적: 원위부 후대뇌동맥 뇌동맥류의 혈관 내 치료에 따른 임상적 결과에 대해 알아보고자 하였다.
대상과 방법: 2002년 12월에서 2013년 12월까지 인제대학교 부산백병원과 고신대학교 복음병원에서 원위부 후대뇌동맥 뇌동맥류로 혈관 내 치료를 받은 11명 환자의 11개 뇌동맥류에 대해 후향적으로 분석하였다.
결과: 11명의 환자 중 남자가 3명(27.3%), 여자가 8명(72.7%)이었으며 평균 나이는 56.6세(44~72세)였고, 평균 크기 는 8.45 mm(3~30 mm)였다. 해부학적 위치는 각각 P2 분절 4개(36.4%), P3 분절 6개(54.5%), P1과 P2 분절의 경 계에 위치한 경우가 1개(9.1%)였다. 7개(63.6%)의 뇌동맥류가 모체 동맥을 보존하며 선택적 뇌동맥류 색전술을 시행하 였으며, 나머지 4개(36.4%)의 뇌동맥류는 뇌동맥류와 동시에 모체 동맥을 폐쇄하는 방법으로 치료가 이루어졌다. 치료 후 합병증 발생률은 27%였으며, 이환율은 9.1%, 사망률은 18%였다.
결론: 원위 후대뇌동맥 뇌동맥류의 혈관 내 치료는 후대뇌동맥 특유의 다양하고 풍부한 곁순환을 고려하여 치료방침을 정한다면 신경학적 결손을 최소화하는 치료법으로 사용될 수 있다.
1성균관대학교 의과대학 삼성병원 영상의학과, 2인제대학교 의과대학 부산백병원 영상의학과,
3고신대학교 의과대학 복음병원 신경외과