38 접수일: 2010년 2월 4일, 게재결정: 2010년 2월 7일
*교신저자: 정명호, 501-757, 전남대학교병원 심장센터, Phone: 062-220-6243, FAX: 062-228-7174, E-mail: [email protected]
Chonnam Medical Journal Vol. 46, No. 1, pp. 38∼43 DOI: 10.4068/cmj.2010.46.1.38
급성 심근경색증 환자에서 Lipoprotein (a)와 섬유소원 농도에 따른 임상 경과
전남대학교병원 심장센터, 보건복지부 지정 심장질환 특성화연구센터
김수현ㆍ정명호*ㆍ이민구ㆍ고점석ㆍ박근호ㆍ심두선ㆍ홍영준ㆍ김주한ㆍ안영근ㆍ강정채
The Relationship between the Levels of Lipoprotein (a) and Fibrinogen and Clinical Outcome in Patients with Acute Myocardial Infarction
Su Hyun Kim, Myung Ho Jeong*, Min Goo Lee, Jum Suk Ko, Keun-Ho Park, Doo Sun Sim, Young Joon Hong, Ju Han Kim, Youngkeun Ahn and Jung Chaee Kang
The Heart Center of Chonnam National University Hospital, Heart Research Center of Chonnam National University Hospital Designated by Korea Ministry of Health, Welfare and Family Affairs, Gwangju, Korea
The aim of this study was to evaluate clinical outcomes in patients with acute myocardial infarction (AMI) on the basis of serum levels of lipoprotein (a) [Lp(a)] and fibrinogen. A total of 537 consecutive patients (62.4±12.3 years) diagnosed with AMI between January 2006 and December 2007 were divided into four groups according to serum levels of Lp(a) and fibrinogen on admission [group I: normal Lp(a) and normal fibrinogen levels (n=235); group II: elevated Lp(a) and normal fibrinogen levels (n=100); group III: normal Lp(a) and elevated fibrinogen levels (n=105); group IV: elevated Lp(a) and elevated fibrinogen levels (n=95)]. The baseline clinical characteristics showed significant differences between the four groups in age (p<0.001), body mass index (p=0.025), N-terminal pro-brain natriuretic peptide levels (p<0.001), left ventricular ejection fraction (p<0.001), and echocardiographic wall motion scores (p<0.001). In the coronary angiographic findings, the number of diseased vessels was higher?and involvement of the left anterior descending artery was more common in group IV than in group I (1.8±0.9 vs. 1.5±0.8, p=0.001, and 65% vs. 51%, p=0.042, respectively). Likewise, in-hospital and 1-month major adverse cardiac events were more frequent in group IV than in group I (4.2% vs. 1.3%, p=0.037, and 14.1% vs. 3.1%, p<0.001, respectively). In conclusion, AMI patients with high Lp(a) or fibrinogen levels had worse clinical outcomes than did patients with normal levels of Lp(a) and fibrinogen.
Key Words: Lipoproteins; Fibrinogen; Prognosis
서 론
현재 우리나라는 경제 수준의 성장 및 식생활의 서구화, 노령화 사회로 변함에 따라 관상동맥질환의 빈도가 급증하 고 있으며, 허혈성 심혈관 질환에 의한 사망이 가장 주요한
원인으로 대두되고 있다.1
Lipoprotein (a) [Lp(a)]는 1963년 노르웨이의 Kare Berg 에 의하여 처음 보고된 지질단백이며,2 관상동맥질환과 뇌경 색증을 비롯하여 동맥경화를 촉진하는 독립된 위험인자 중 하나임이 여러 임상적 연구 결과에 의하여 확인되어 왔다.
Lp(a)는 혈관벽에서 plasminogen이 plasmin으로 활성화되 는 것을 억제하며 부적절한 fibrinolysis를 유발하여 죽상경 화반을 증가시키고 혈전생성을 유발한다. 일반적으로 Lp(a) 농도가 30 mg/dL 이상이면 동맥경화의 발현과 통계적으로 유의하다고 알려져 있다. 또한 fibrinogen의 체내 농도가 높 을수록 심혈관계에 악영향을 줄 수 있다는 것도 여러 연구 에서 증명되고 있다. 우리나라에서도 관상동맥질환이나 뇌 경색증에서 독립적인 위험인자로 작용하고 있고 당뇨병에서 도 연관성이 높다는 보고가 있었다.3 그러나 실제 생체 내에 서 Lp(a)의 농도와 fibrinogen의 관계 및 혈전형성경향에 대해서 대규모 연구가 부족한 실정이다.
본 연구는 급성 심근경색증으로 내원한 환자를 대상으로 Lp(a)와 fibrinogen의 농도에 따른 임상적 경과의 차이를 분석하였다.
대상 및 방법
1. 연구 대상
2006년 1월부터 2007년 12월까지 전남대학교병원에 내 원하여 흉통 등의 임상증상, 심전도 변화, 심근효소변화 등 에 따라 급성 심근경색증으로 진단받은 환자 537명(남 : 여
=381 : 156, 연령=62.44±12.3세)을 대상으로 하였다.
2. 방법
대상환자들의 성별, 나이, 체중, 신장, 흡연 유무 등을 조 사하였으며 흡연조사는 현재 흡연자와 흡연 과거력이 있는 자를 모두 흡연군에 포함하였다. 체질량 지수는 체중(kg)/신 장(m2)의 관계식으로 구하였고, Lp(a), 혈청 총 콜레스테롤, 중성지방, 고밀도 지단백 콜레스테롤 등의 혈액 검사는 입원 후 1일째 8시간 이상 공복을 유지한 후 채취된 혈액으로 분 석하였다. Lp(a)의 정상 값은 30 mg/dL, fibrinogen의 정상 값은 350 mg/dL을 기준으로 하였다.
Lp(a)는 Behrring Nephelometer II를 이용하여 측정 검체 의 혼탁도를 Laser diode lamp에 의해서 발생되는 빛을 이용 하여 Scattered를 840 nm에서 측정하므로 정량적 분석하였
고 End point method를 사용하여 측정하였다.4 Fibrinogen 은 Sysmax CA-7000을 이용하여 시약반응을 거친 검체에 광원을 조사하고 산란광을 분석하여 변화율이 50%에 달하 는 점을 기존에 계산된 standard curve point와 비교하여 값을 측정하였다.5
심초음파를 통한 좌심실 구혈률(ejection fraction) 측정 은 biplane modified Simpson's rule을 이용하였으며 입원 1일 이내 검사하였다.6
대상 환자를 Lp(a)와 fibrinogen 측정값에 따라 4군으로 분류하였다. Group I: 정상(n=235, 60.1±12.7세, 남=
73.8%), Group II: Lp(a)증가(n=100, 62.5±11.5세, 남=
67.0%), Group III: fibrinogen증가(n=105, 63.7±12.3세, 남=68.6%), Group IV: Lp(a)와 fibrinogen 증가(n=95, 66.4±10.9세, 남=70.5%).
이들 군 간에 12개월 주요 심장사건을 추적 관찰하여 임 상적 유의성을 평가하였다.
3. 통계학적 분석
표기된 변수는 평균±표준편차로 표시하였고, 통계처리는 SPSS for Windows 15.0 (Stastistical Package for the Social Sciences, SPSS INC., USA)을 이용하였으며 연속 변수에 대한 그룹 간의 비교는 one way ANOVA test를 사용하였다. 1년 추적관찰 동안 각 변수의 교차비 및 비교 위험도를 구하는 단변량 분석을 시행한 후 유의한 변수에 대해 Cox regression analysis를 시행하여 종속 변수(사망 률)에 독립적으로 작용하는 지를 분석하였다. 또한 각 그룹 별로 생존곡선을 kaplan-Meier survival analysis로 작성하 였다. 모든 p-value 값은 0.05 미만일 때 통계적으로 유의한 것으로 판정하였다.
결 과
1. 임상적 특징
전체 대상자의 평균 나이는 62.4±12.3세였고 남자가 70.3%
였으며 Lp(a)의 평균 농도는 30.9±26.7 mg/dL이었으며, fibrinogen의 평균 농도는 335.9±111.0 mg/dL였다. 각 그룹간 의 임상적 특성을 분석한 결과 성별을 포함하여 고혈압, 당뇨병, 흡연, 고지혈증 등 심혈관 질환의 위험인자는 유의한 차이를 보이지 않았으나 Lp(a)와 fibrinogen이 높은 군에서 평균 나이 가 더 많았으며(p<0.001), 체질량 지수는 감소되는 양상으로
Table 1. Comparison of clinical and laboratory finding of four groups according to the levels of lipoprotein (a) and fibrinogen Group I (n=237) Group II (n=100) Group III (n=105) Group IV (n=95) p value Clinical characteristics
Age (years) Male (%) BMI (kg/m2) Hypertension (%) DM (%) Dyslipidemia (%) Smoking (%) STEMI (%) Laboratory finding Lp(a) (mg/dL) Fibrinogen (mg/dL) Glucose (mg/dL) Creatinine (mg/dL) Creatine-kinase (IU/L) CK-MB (IU/L) Troponin I (ng/mL) TC (mg/dL) Triglyceride (mg/dL) HDL-C (mg/dL) LDL-C (mg/dL) hs CRP (mg/dL) NT-proBNP (pg/mL)
60.1±12.7 73.8 24.2±3.0 43.5 (n=103)
26.6 (n=63) 3.8 (n=16) 62.0 (n=147)
38.4 (n=91)
15.5±6.4 260.5±49.9 175.8±86.7 1.1±0.6 1,709.2±2,048.2
99.6±116.2 53.3±68.9 179.8±40.2 129.9±97.4 49.1±37.1 115.9±35.1 1.9±3.1 1,726.2±4,576.1
62.5±11.5 67.0 24.4±2.9 47.0 (n=47) 27.0 (n=27) 5.0 (n=5) 58.0 (n=58) 39.0 (n=39)
57.1±27.1 280.2±44.5 172.2±84.0 1.2±1.3 1,289.3±1,680.0
97.2±116.9 51.7±67.9 185.4±37.4 102.8±48.7 46.9±11.7 122.4±37.1 1.7±3.0 1,986.4±4,762.6
63.7±12.3 68.6 24.3±3.2 54.3 (n=57) 34.3 (n=36) 5.7 (n=6) 61.9 (n=65) 40.9 (n=43)
16.2±6.3 450.1±86.1 169.9±79.2 1.2±1.4 1,477.5±1,790.1
91.1±113.7 50.7±77.2 182.7±42.9 119.1±74.3 43.3±11.8 121.9±36.8 4.1±5.3 4,442.3±7,783.7
66.4±10.9 70.5 23.1±3.8 49.5 (n=47) 29.5 (n=28) 7.4 (n=7) 58.9 (n=56) 43.1 (n=41)
58.2±28.6 456.4±82.7 191.5±113.0
1.3±0.8 1,336.9±1,543.9
87.8±107.1 52.2±70.4 181.9±41.4 104.3±49.7 46.3±14.3 119.8±39.6 3.9±4.5 6,274.2±9,105.4
<0.001 0.404 0.025 0.315 0.785 0.660 0.585 0.157
<0.001
<0.001 0.051 0.001 0.018 0.795 0.968 0.141 0.009 0.618 0.186
<0.001
<0.001 BMI, body mass index; DM, Diabetes mellitus; Lp(a), lipoprotein(a); CK-MB, creatine kinase-MB; TC, total cholesterol; HDL-C, high density lipoprotein- cholesterol; LDL-C, Low density lipoprotein-cholesterol; hsCRP, high sensitive C-reactive protein; NT-proBNP, N-terminal pro-B-type natriuretic peptide.
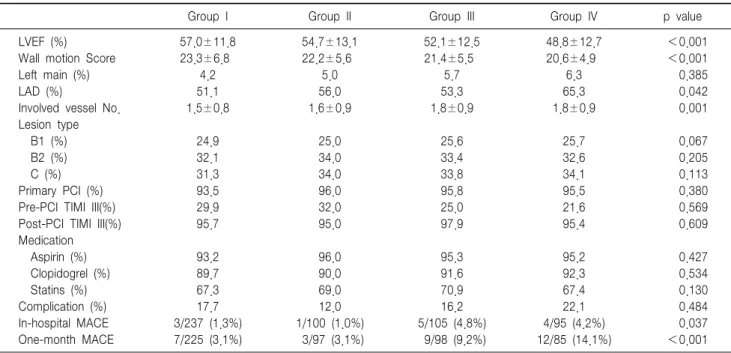
관찰되었다(p=0.025). 관상동맥 조영술에서 2개 이상의 혈관 을 침범한 경우는 32.7%였고 관상동맥 중재술 시술 전후에 Thrombolysis In Myocardial Infarction (TIMI) III flow는 각각 25.7%와 87.5%로 관찰되었다.
2. 진단의학 검사실, 심초음파 및 관상동맥 조영술 소견 진단의학검사에서 Lp(a)와 fibrinogen이 높은 군에서 high sensitivity C-reactiv protein (hsCRP) (p<0.001), N- terminal pro-B-type natriuretic peptide (NT-proBNP) (p
<0.001), 및 creatinine(p=0.001) 등이 더 높았다(Table 1).
심초음파도 검사에서 Lp(a)와 fibrinogen이 높은 군일수록 좌 심실 구혈률이 낮았으며(p<0.001), 좌심실의 벽운동 점수 지 수(wall motion score index)는 높았다(p<0.001). 각 군 간의 관상동맥 조영술에서 좌전하행동맥 병변이 Lp(a)와 fibrinogen 이 높은 그룹에서 더 많이 관찰되었으며(p=0.042), 병변이 관찰된 혈관 수도 더 많았다(p=0.001).
3. 임상 추적 관찰 및 사망률에 따른 분석 결과
537예 중 입원기간 내에 사망은 13건(2.4%)이었으며 사 인으로는 심부전이 8예, multi-organ failure 2예, 심근경색
후 합병증(ventricular septal defect) 1예, sudden cardiac death 2예가 발생하였다. 1개월 추적 관찰은 505예에서 시 행되었으며, 31예(6.1%)에서 주요 심장사건이 발생하였고 각 군 간의 유의한 차이를 나타내었다(p<0.001)(Table 2).
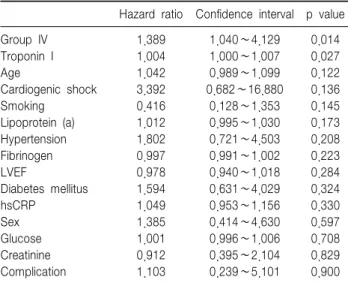
1년 추적 관찰은 380예에서 시행되었고 사망은 총 41건 (7.6%)이었다. 생존자와 사망자 간의 임상적 차이를 비교한 결과 사망자 군에서 평균 연령이 높았으며 상대적으로 남성 의 비율이 적었고(53.6%) 체질량지수는 낮았으며, Killip class II 이상이 더 많이 관찰되었다. 또한 고혈압과 당뇨를 가진 경우가 더 많았다(Table 3.). 평균 추적관찰 기간은 263.9일이었으며 단변량 분석을 통해 추적관찰 기간 내 사 망률에 관여하는 유의한 인자로 age (p<0.001), sex (p=
0.008), Group IV (p<0.001), hypertension (p<0.001), diabetes mellitus (p=0.007), smoking (p=0.031), Lp(a) (p=0.028), fibrinogen (p<0.001), glucose (p=0.001), creatinine (p<0.001), troponin I (p=0.021), high sensitive C-reactive protein (p<0.001), NT-proBNP (p
<0.001), left ventricular ejection fraction (p<0.001) 등이었다(Table 4). 이에 대하여 Cox regression analysis를 이용한 독립 위험 인자로서의 유의성을 평가한 결과 Group
Table 2. Comparison of coronary angiographic finding and major adverse cardiac events among four groups
Group I Group II Group III Group IV p value
LVEF (%) Wall motion Score Left main (%) LAD (%)
Involved vessel No.
Lesion type B1 (%) B2 (%) C (%) Primary PCI (%) Pre-PCI TIMI III(%) Post-PCI TIMI III(%) Medication Aspirin (%) Clopidogrel (%) Statins (%) Complication (%) In-hospital MACE One-month MACE
57.0±11.8 23.3±6.8
4.2 51.1 1.5±0.8
24.9 32.1 31.3 93.5 29.9 95.7
93.2 89.7 67.3 17.7 3/237 (1.3%) 7/225 (3.1%)
54.7±13.1 22.2±5.6
5.0 56.0 1.6±0.9
25.0 34.0 34.0 96.0 32.0 95.0
96.0 90.0 69.0 12.0 1/100 (1.0%) 3/97 (3.1%)
52.1±12.5 21.4±5.5
5.7 53.3 1.8±0.9
25.6 33.4 33.8 95.8 25.0 97.9
95.3 91.6 70.9 16.2 5/105 (4.8%) 9/98 (9.2%)
48.8±12.7 20.6±4.9
6.3 65.3 1.8±0.9
25.7 32.6 34.1 95.5 21.6 95.4
95.2 92.3 67.4 22.1 4/95 (4.2%) 12/85 (14.1%)
<0.001
<0.001 0.385 0.042 0.001
0.067 0.205 0.113 0.380 0.569 0.609
0.427 0.534 0.130 0.484 0.037
<0.001 LVEF, left ventricular ejection fraction; LAD, Left anterior descending artery; LCX, Left circumflex artery; RCA, Right coronary artery; PCI, percutaneous coronary intervention; TIMI, Thrombolysis In Myocardial Infarction; ACE, angiotensin converting enzyme: ARB, Angiotensin II Receptor Blocker MACE, major adverse cardiac events.
Table 3. Baseline clinical characteristics between survivors and moribund patients
Survivors (n=496)
Non-survivors (n=41) p value Age, years
Male (%)
Body mass index, kg/m2 SBP, mmHg
DBP, mmHg Heart rate, /min Killip class > II (%) Hypertension (%) Diabetes mellitus (%) Hyperlipidemia (%) Smoking (%) Family history (%)
61.4±14.3 72.9 24.1±3.2 134.6±30.1
83.1±18.7 74.4±17.8
18.8 47.3 28.7 5.0 59.7 5.0
70.3±16.4 53.6 23.4±2.6 129.8±27.9
82.7±17.9 76.1±19.1
63.4 73.1 46.3 1.2 46.3 1.1
<0.001
<0.001 0.035 0.127 0.311 0.109
<0.001
<0.001
<0.001 0.446 0.598 0.454 SBP, systolic blood pressure; DBP, diastolic blood pressure.
Table 4. Univariate predictors of one-year mortality
Variable Categorical Variables
Hazard ratio Confidence interval p value Male sex
Group IV Chest pain Previous MI history Hypertension Diabetes mellitus Dyslipidemia Smoking Family history Thrombolysis PCI
2.15 3.12 3.08 0.73 3.59 2.45 0.89 1.88 0.58 0.93 0.53
1.21∼3.81 1.54∼5.88 1.75∼5.43 0.41∼1.30 1.70∼7.58 1.25∼4.76 0.85∼0.92 1.05∼3.35 0.83∼1.09 0.35∼2.48 0.24∼1.19
0.008
<0.001
<0.001 0.286
<0.001 0.007 0.153 0.031 0.604 0.898 0.117 Continuous Variables
Hazard ratio Confidence interval p value Age
Lipoprotein(a) Fibrinogen Glucose Creatinine Troponin I hsCRP NT-proBNP LVEF
2.00 1.91 2.67 1.85 0.11 2.41 1.87 2.69 2.05
1.02∼3.95 1.29∼3.96 1.48∼4.82 1.73∼3.93 0.28∼0.70 1.34∼4.33 1.01∼3.47 1.45∼4.99 1.07∼3.93
<0.001 0.028
<0.001 0.001
<0.001 0.021
<0.001
<0.001
<0.001 hsCRP, high sensitive C-reactive protein; NT-proBNP, N-terminal pro-B-type natriuretic peptide LVEF, left ventricular ejection fraction.
IV (p=0.014)가 유의한 위험도(hazard ratio=1.389)를 나 타내었다(Table 5).
고 찰
심근경색증이나 협심증 등의 관상동맥 질환에 대한 관심 이 높아지고 있으며, 여러 위험인자에 대한 연구가 활발하게
Table 5. Cox regression analysis for independent predictors of one-year mortality in the patients with acute myocardial infarction
Hazard ratio Confidence interval p value Group IV
Troponin I Age
Cardiogenic shock Smoking
Lipoprotein (a) Hypertension Fibrinogen LVEF
Diabetes mellitus hsCRP
Sex Glucose Creatinine Complication
1.389 1.004 1.042 3.392 0.416 1.012 1.802 0.997 0.978 1.594 1.049 1.385 1.001 0.912 1.103
1.040∼4.129 1.000∼1.007 0.989∼1.099 0.682∼16.880
0.128∼1.353 0.995∼1.030 0.721∼4.503 0.991∼1.002 0.940∼1.018 0.631∼4.029 0.953∼1.156 0.414∼4.630 0.996∼1.006 0.395∼2.104 0.239∼5.101
0.014 0.027 0.122 0.136 0.145 0.173 0.208 0.223 0.284 0.324 0.330 0.597 0.708 0.829 0.900 hsCRP, high sensitive C-reactive protein; LVEF, left ventricular ejection fraction.
이루어지고 있다. Lp(a)에 대한 연구에서 유전적 요소7나 인 종 간의 차이가 대두되어 있으며 간에서 대사 과정이 이루 어진다는 견해가 있으나 정확한 결론은 내려지지 않았다.8 또한 관상동맥 질환의 위험인자들에 대해 조기부터 조절하 는 것이 혈관 질환 발생 예방에 큰 도움이 된다고 알려져 있 고 Lp(a)의 경우 데이터로 분석한 여러 연구에서 분명한 독 립적 위험인자로 제시하고 있으나,9,10 명확한 예방적 가이드 라인이 없으며 치료에 대한 관심도 크게 부족한 실정이다.
Lp(a)는 plasminogen이 plasmin으로 전환하는 것을 방해 함으로써 결과적으로 fibrinolysis를 저하시켜 혈전 형성을 용 이하게 만든다.11 이러한 과정으로 체내 fibrinogen은 상대적 으로 높은 혈중 농도를 유지하며 pre-thrombotic condition의 위험도가 증가하게 된다. Fibrinogen의 경우 역시 심혈관 질 환과 깊은 관계가 있는 위험인자로 알려져 있으며,12,13 최근 발표된 CARDIA study14에 따르면 비교적 젊은 연령에서 부터 fibrinogen의 혈중 농도가 높았던 경우에 무증상의 죽 상동맥경화증 진행 및 심혈관 질환 발현율이 높았다고 보고 하고 있다. 저자들이 시행한 연구에서도 Lp(a)와 fibrinogen 의 농도를 기준으로 정상군과 높은 혈중 농도를 보인 군 간 에 비교 분석 결과는 임상적 특성부터 진단 의학 검사, 심초 음파도 및 관상동맥 조영술 결과까지 유의한 차이가 있었다.
시술 후 합병증에서 입원기간 동안 사망률에서 유의한 차이 를 나타냈고 1개월 추적관찰 주요심장사건도 의미있는 결과 를 얻었다. 또한 개별 그룹간 비교분석 결과 우관상동맥 침 범이 Lp(a)가 높은 군이나 fibrinogen이 높은 군에서 각각
정상군보다 유의하게 많이 발견되었다. 단변량 분석을 통해 유의한 위험인자들에 대해 Cox 회귀 분석을 통한 독립적 위험도를 검사한 결과 Group IV에서 위험도가 유의하게 높 았으며 이는 두 인자 Lp(a), fibrinogen이 함께 높은 군에서 급성심근경색의 사망률이 높아짐을 나타낸다. 그러나 이번 연구에서는 Lp(a)나 fibrinogen이 각각 단독으로 작용하는 급성 심근경색증의 사망률에 위험인자인 것을 증명하지 못 했으며 좀 더 많은 환자를 분석할 경우 유의한 결과가 나올 것으로 예상된다.
또 다른 여러 연구에서 Lp(a) 와 fibrinogen가 고지혈증 과 뇌졸중 환자에서도 위험인자임을 명시하고 있어서 심뇌 혈관계 질환을 연구하는 이들의 주목을 받고 있다.15,16 많은 연구에서 Lp(a)와 fibrinogen이 심뇌혈관 질환의 위험 인자임을 지적하고 있으나 치료 방침에 대한 자료는 보기 드 물다. 한 연구에서는 급성 관상동맥증후군으로 경피적 관상 동맥 중재술을 시행받은 환자에게 statin과 함께 fenofibrate 를 추가하여 혈중 fibrinogen 농도를 낮추는 것이 위험요소 를 감소시키는데 상승 효과가 있다는 보고하였다.17 현재까지 Lp(a)나 fibrinogen에 대한 연구는 분자생물학 적인 방향18,19과 유전요소20에 대한 연구가 진행되고 있으며, 이들 대사과정에 대한 결과를 토대로 새로운 치료 등에 대 한 가이드라인이 제시될 수 있을 것으로 생각된다.21 또 Framingham Offspring Study 등22을 통해서 다른 생화학 적 표지자들과 어떤 연계관계를 나타내는 가 혹은 치료에 대한 반응은 어떠한 가에 대한 연구 등23-27도 계속 진행되고 있다. 건강한 피험자에서 혈중 지질 농도는 정상이지만 함께 측정한 Lp(a)나 fibrinogen의 혈중 농도가 높은 경우에도 관상동맥 질환의 발생을 예방하고 치료하는데 필요한 Lp(a) 와 fibrinogen의 적절한 기준치를 제시하는 것과 이러한 기 준을 유지하기 위한 표준화된 치료 지침을 만들고자 하는 노력이 필요하며, 이를 위해서는 대규모 전향적인 연구가 필 요할 것으로 사료된다.
결론적으로 본 연구에서는 Lp(a)와 fibrinogen에 동시에 증가된 급성 심근경색증 환자에서 임상경과가 불량하여 더 욱 적극적인 치료를 요함을 알 수 있었다.
알 림
본 연구는 보건복지가족부 보건의료기술진흥사업의 지원 에 의하여 이루어졌음 (과제고유번호 : A084869).
References
1. Suh I. Cardiovascular mortality in Korea: a country experiencing epidemiologic transition. Acta Cardiol 2001;56:75-81.
2. Berg K. A new serum type system in man--the Lp system. Acta pathol Microbiol Scand 1963;59:369-82.
3. Lee HB. Non-insulin-dependent diabetes mellitus, proteinuria, and Lipoprotein (a). Korean J Med 1999;57:136-8.
4. Marcovina SM, Albers JJ, Scanu AM, KennedyH, GiaculliF, BergK, et al. Use of reference material proposed by the international federation of clinical chemistry and laboratory medicine to evaluate analytical methods for the determination of plasma lipoprotein (a). Clin Chem 2000;46:1956-67.
5. Tan V, Doyle CJ, Budzynski AZ. Comparison of the kinetic fibrinogen assay with the von Clauss method and the clot recovery method in plasma of patients with conditions affecting fibrinogen coagulability.
Am J Clin Pathol 1995;104:445-62.
6. Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R, Feigenbaum H, et al. Recommendations for quantitation of the let ventricle by two-dimensional echocardiography. American society of echocardiography committee on standards, subcommittee on quantitation of two-dimensional echocardiograms. J Am Soc Echocardiogr 1989;2:358-67
7. Gambhir JK, Kaur H, Prabhu KM, Morrisett JD, Gambhir DS. Association between lipoprotein (a) levels, apo (a) isoforms and family history of premature CAD in young Asian Indians. Clin Biochem 2008;41:453-8.
8. Ebesunun MO, Agbedana EO, Taylor GO, Oladapo OO. Plasma lipoprotein (a), homocysteine, and other cardiovascular disease (CVD) risk factors in Nigerians with CVD. Appl Physiol Nutr Metab 2008;33:282-9.
9. Hartmann M, von Birgelen C, Mintz GS, Stoel MG, Eggebrecht H, Wieneke H, et al. Relation between lipoprotein(a) and fibrinogen and serial intravascular ultrasoundplaque progression in left main coronary arteries. J Am Coll Cardiol 2006;48:446-52.
10. Kamstrup PR, Benn M, Tybaerg-Hansen A, Nordestgaard BG. Extreme lipoprotein(a) levels and risk of myocardial infarction in the general population: the Copenhagen City Heart Study. Circulation 2008;117:176-84.
11. Barre DE. The molecular nature and consequences of lipoprotein (a)'s association with platelets. Protein Pept Lett 2007;14:839-42.
12. Fujii C, Sakakibara H, Kondo T, Yatsuya H, Tamakoshi K, Toyoshima H. Plasma fibrinogen levels and cardiovascular risk factors in Japanese school children. J Epidemiol 2006;16:64-70.
13. Mannila MN, Lovely RS, Kazmierczak SC, Eriksson P, Samnegård A, Farrell DH, et al. Elevated plasma fibrinogen gamma' concentration is associated with myocardial infarction: effects of variation in fibrinogen genes and environmental factors. J Thromb Haemos 2007;5:766-73.
14. Green D, Foiles N, Chan C, Schreiner PJ, Liu K. Elevated fibrinogen levels and subsequent subclinical atherosclerosis: the CARDIA Study.
Atherosclerosis 2009;202:623-31.
15. Ganotakis ES, Gazi IF, Papadakis JA, Jagroop IA, Nair DR, Mikhailidis DP. The relationship between circulating fibrinogen and lipoprotein (a) levels in patients with primary dyslipidemia. Clin Appl Thromb Hemost 2007;13:35-42.
16. Smolders B, Lemmens R, Thijs V. Lipoprotein (a) and stroke: a meta- analysis of observational studies. Stroke 2007;38:1959-66.
17. Shah HD, Parikh KH, Chag MC, Shah UG, Baxi HA, Chandarana AH, et al. Beneficial effects of the addition of fenofibrate to statin therapy in patients with acute coronary syndrome after percutaneous coronary interventions. Exp Clin Cardol 2007;12:91-6.
18. Shin MJ, Blanche PJ, Rawlings RS, Fernstrom HS, Krauss RM. Increased plasma concentrations of lipoprotein(a) during a low-fat, high-carbohydrate diet are associated with increased plasma concentrations of apolipoprotein C-III bound to apolipoprotein B-containing lipoproteins. Am J Clin Nutr 2007;85:1527-32.
19. Albahrani AI, Usher JJ, Alkindi M, Marks E, Ranganath L, Al-yahyaee S. Apolipoprotein A1-75 G/A (M1-) polymorphism and lipoprotein (a);
anti- vs. pro-atherogenic properties. Lipids Health Dis 2007;6:19.
20. Mannila MN, Lovely RS, Kazmierczak SC, Eriksson P, Samnegård A, Farrell DH, et al. Elevated plasma fibrinogen gamma' concentration is associated with myocardial infarction: effects of variation in fibrinogen genes and environmental factors. J Thromb Haemost 2007;5:766-73.
21. Joy MS, Dornbrook-Lavender KA, Chin H, Hogan SL, Denu-Ciocca C. Effects of atorvastatin on lipoprotein (a) and lipoprotein profiles in hemodialysis patients. Ann Pharmacother 2008;42:9-15.
22. Murabito JM, Keyes MJ, Guo CY, Keaney JF Jr, Vasan RS, D'Agostino RB Sr, et al. Cross-sectional relations of multiple inflammatory biomarkers to peripheral arterial disease: the framingham offspring study. Atherosclerosis 2009;203:509-14.
23. Zakai NA, Katz R, Jenny NS, Psaty BM, Reiner AP, Schwartz SM, et al. Inflammation and hemostasis biomarkers and cardiovascular risk in the elderly: the Cardiovascular Health Study. J Thromb Haemost 2007;5:1128-35.
24. Sattar N, Williams K, Sniderman AD, D'Agostino R Jr, Haffner SM.
Comparison of the associations of apolipoprotein B and non-high-density lipoprotein cholesterol with other cardiovascular risk factors in patients with the metabolic syndrome in the Insulin Resistance Atherosclerosis Study. Circulation 2004;110:2687-93.
25. Murase T, Okubo M, Amemiya-Kudo M, Hiraga T, Oka J, Shimada M, et al. Impact of markedly elevated serum lipoprotein(a) levels (>
or = 100 mg/dL) on the risk of coronary heart disease. Metabolism 2007;56:1187-91.
26. Páramo JA, Beloqui O, Roncal C, Benito A, Orbe J. Validation of plasma fibrinogen as a marker of carotid atherosclerosis in subjects free of clinical cardiovascular disease. Haematologica 2004;89:1226-31.
27. Park OY, Kim SH, Ahn YK, Yun NS, Kim JH, Sim DS, et al. Statin reduces C-reactive protein and interleukin-6 in normocholesterolemic patients with acute coronary syndrome. Chonnam Med J 2008;44:13-6.