475 서 론
혈청 전립선 특이항원 (prostate-specific antigen; PSA)을 통
한 선별검사와 초음파 유도하 확대 전립선 생검은 전립선 암의 발견을 급격히 증가시켰으며,1 또한 분화도가 좋고, 종 양 용적이 적은 임상적으로 무의미한 암의 발견도 증가시 킬 수 있다.2 병기가 낮은 환자에게 근치적 전립선적출술의
임상적 의의
Clinical Significance of a Single-Core Positive Prostate Cancers Detected on Extended Prostate Needle Biopsy
Yong Jun Kim, Sang Cheol Lee, In Ho Chang, Myung Cheol Gil, Sung Kyu Hong, Seok-Soo Byun, Sang Eun Lee
From the Department of Urology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
Purpose: The widespread use of serum prostate specific antigen and ex- tended needle biopsy of the prostate as screening procedures for prostate cancer has not only led to an increase of detecting prostate cancer as a whole, but also to an increase of detecting small low grade tumors. Still, the clinical significance of small, low grade, single-core positivity on pro- state biopsy hasn't yet been determined. So, we tried to investigate the clinicopathological features of prostate cancers that showed only single- core positivity on extended prostate needle biopsy.
Materials and Methods: 144 patients were managed with radical prosta- tectomy during 2003-2005 at our institution. Insignificant prostate cancer on biopsy specimens was defined as a single-core positive biopsy con- taining a focus of 3mm or less of moderately differentiated prostate cancer (Gleason score≤6) and clinical insignificant cancer in the radical speci- mens was defined as a low volume (<0.5cc) of moderately differentiated organ- confined prostate cancer. We analyzed the clinicopathological fea- tures and the clinical significance in regards to the number of positive cores and the biopsy significance.
Results: Of 144 patients, 46 (31.9%) patients were diagnosed on the basis on single-core positive prostate cancer. Of these 114 patients, 32 (69.6%) patients had insignificance prostate cancer on biopsy. Although the single core positive group had more favorable pathologic features than the multiple core positive group, only 5 (10.9%) were found to have clinically insignificant cancer at radical prostatectomy. Also, in the biopsy insigni- ficant group, only 5 patients (15.6%) were found to have clinically insig- nificant cancer. However, there were no features that could accurately predict insignificant prostate cancer preoperatively.
Conclusions: Although the clinicopathological features of the prostate cancers that were detected in only a single-core on prostate needle biopsy were observed to be suggestive of less advanced disease, most of such single-core positive cancers may be clinically significant disease. (Korean J Urol 2006;47:475-481)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Key Words: Prostate cancer, Biopsy, Prostatectomy
대한비뇨기과학회지 제 47 권 제 5 호 2006
서울대학교 의과대학 비뇨기과학교실
김용준․이상철․장인호․길명철 홍성규․변석수․이상은
접수일자:2005년 11월 7일 채택일자:2006년 1월 19일
교신저자: 이상은
분당서울대학교병원 비뇨기과 경기도 성남시 분당구 구미동 300번지
ꂕ 463-707 TEL: 031-787-7341 FAX: 031-787-4057 E-mail: [email protected]
시행은 사망률을 감소시킬 수 있다.3 그러나 선별검사를 통 하여 진단된 전립선암 환자는 사망률이 불과 25-33%이며, 이들에게 이용 가능한 모든 치료법은 삶의 질에 부정적인 영향을 미치게 된다.4 그러므로 낮은 위험도를 가진 국소 전립선암 환자의 장기 예후가 매우 우수하다는 점에서 최 근에는 이들의 치료와 관련된 이환율의 감소에 대한 관심 이 증가하게 되었다.
선별검사와 초음파 유도하 확대 전립선 생검은 분화도가 좋고, 종양의 용적이 적고, 생검조직에서 단일 core에서만 암이 발견되는 소견을 보이는 전립선암의 발견을 증가시켰 다. 일부 연구에서, 분화도가 좋은 적은 용적의 전립선암 환 자에 대한 치료로 대기관찰 요법을 시행할 것을 권장하고 있으나,5-7 다른 연구에서는 전립선 생검의 적은 종양 용적 은 전체 전립선에서의 적은 용적의 종양을 의미하지 않으 며 대부분 임상적으로 의미 있는 암이므로 적극적인 치료 가 필요하다고 보고하고 있다.8-12
전립선암의 치료 시행 전 임상적으로 무의미한 암을 발 견하기 위한 많은 노력이 있었으나 술 전에 이들의 정확한 구분에는 한계가 있다.13-16 또한, 생검조직에서 단일 core에 서만 암이 발견된 소견을 보이는 분화도가 좋고, 적은 용적 의 전립선암에 대한 임상적 의의에 대한 규명이 정확히 이 루어지지 않아 이들에게 대기관찰요법이나 근치적 전립선 적출술의 시행 여부에 관한 치료법 선택 시 많은 어려움을 겪게 된다. 현재까지는 실제 종양 용적을 정확히 예측할 수 있는 영상 기법이 없는 상태이므로, 전립선 생검 조직의 세 심한 분석이 임상적으로 무의미한 암을 예측하는 데 좋은 방법이 될 수 있다.
저자들은 확대 전립선 생검을 통하여 발견된 단일 core에 서만 암이 발견된 전립선암 환자 및 이들 환자 중 분화도가 좋으며, 미세 생검조직에서만 암이 발견된 환자들의 임상 적 의의에 대한 연구를 시행하였다.
재료 및 방법
2003년 11월부터 2005년 7월까지 본원에서 임상적으로 국소 전립선암으로 진단되어 근치적 후치골 전립선적출술
(radical retropubic prostatectomy; RRP)을 시행 받은 144명을 대상으로 하였다. 술 전 혈청 PSA는 radioimmunoassay 방법 으로 측정하였고, 혈청 PSA가 3ng/ml 이상으로 상승된 경 우, 비정상적인 직장수지검사 소견을 보이는 경우, 혹은 경 직장초음파검사상 비정상적인 에코 소견을 보인 경우 전립 선 생검을 시행하였다. 근치적 전립선적출술 이전에 호르 몬 치료를 받았거나 외부에서 전립선 생검을 시행 받은 환 자는 대상에서 제외하였다. 술 전 검사로 직장수지검사, 혈
청 PSA, 골반 및 전립선 자기공명영상 및 골주사 촬영을 시행하였다.
전립선 생검은 경직장초음파 유도하에 18G 생검침을 12 부위에서 시행하였으며, 직장수지검사에서 결절이 만져지 거나 경직장전립선초음파 검사에서 비정상음영이 관찰된 경우 그 부위에 추가적인 생검을 시행하였다.17 전립선 생검 은 경험이 풍부한 방사선과 전문의 1명이 시술하였다. 생검 조직의 병리학적 검사는 1명의 병리과 전문의가 시행하였 으며, 각각의 생검 조직에서 종양의 수, 위치, Gleason score, 종양 길이 등을 기록하였다.
근치적 전립선적출 조직은 1-3일간 10%의 포르말린에 고 정시킨 후 인디아 잉크로 염색한 다음 첨부와 기저부의 5mm는 횡단면으로 절제한 후, 이를 다시 3mm 간격으로 종 단면으로 절제하였다. 그 외의 전체 전립선 조직은 첨부부 터 정낭부위까지 4mm 간격으로 횡단면으로 연속 절제하 여, 각 절제면에서 Gleason score, 종양의 위치, 절단면 양성 여부, 피막 침범여부, 정낭 침범여부, 종양의 무게 및 림프 절 양성 여부에 대한 검사를 시행하였다. 임상 및 병리학적 병기는 2002년 TMN 병기 분류에 따랐다.
술 전 생검 조직에서 임상적으로 무의미한 암은 단일 core에서만 암이 발견되고, Gleason score가 6 이하이고, 종 양 길이가 3mm 미만인 경우로 정의하였으며,13,16 술 후 임 상적으로 무의미한 암은 Gleason score가 6 이하이고, 종양 의 용적이 0.5ml 미만이며, 종양이 전립선 내에 국한된 경우 로 정의하였다.14
단일 core 양성인 환자군과 다발성 core 양성인 환자군에 서 임상적, 병리학적 특성에 관한 비교를 시행하여 단일 core 양성인 환자의 임상적 의의를 분석하고, 단일 core 양 성인 환자군을 생검 조직의 임상적 의미에 따라 다시 2군으 로 구분하여 양 군의 특성을 비교하였다.
통계 분석은 Student's t-test, Chi-square test와 Man-Whitney test를 이용하였으며, p값이 0.05 미만을 통계적으로 의미 있 는 것으로 간주하였다. 통계프로그램은 SPSS version 12.0을 이용하였다.
결 과
전립선암으로 진단되어 근치적 전립선적출술을 시행 받 은 144명의 평균 연령은 65.0±6.0세였고, 평균 PSA 수치는 10.1±8.7ng/ml이었고, 평균 전립선 용적은 42.3±17.6cc였 고, 술 전 평균 전립선 생검 수는 13.4±1.7개였다. 이 중 단 일 core에서 암이 발견된 환자는 31.9% (46/144명)였고, 다 발성 core에서 암이 발견된 환자는 68.1% (98/144명)였다 (Table 1).
단일 core 양성군과 다발성 core 양성군 간에 술 전 평균 연령, 평균 PSA 수치, 임상적 병기에서는 차이가 없었으나, 단일 core 양성군에서 평균 전립선 용적은 49.02±22.96cc로 다발성 core 양성군에 비해 의미있게 큰 전립선 용적을 보 였다 (p<0.05). 단일 core 양성군은 다발성 core 양성군에 비 해 전립선 생검의 평균 종양 비율은 적고, Gleason score는 낮았다 (p<0.05) (Table 2). 단일 core 양성군과 다발성 core 양성군의 술 후 전립선절제 조직의 평균 종양 무게는 각각 3.78g (0.27-24.8g), 8.25g (0.25-37.8g)이었고, 평균 종양 비율 은 각각 10.35% (0.5-40.0%), 23.62% (0.5-90%)였고, 임상적 으로 무의미한 암은 각각 10.9% (5/46명), 1.0% (1/98명)로 Table 1. Characteristics of the patients who underwent radical retropubic prostatectomy
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Variable
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Mean age (years) 65.0±6.0
Mean PSA (ng/ml) 10.1±8.7
Mean prostate volume (cc) 42.3±17.6
No. of biopsy 13.4±1.7
No. of positive core (%)
Single 46 (31.9%)
Biopsy insignificant* 32 (69.6)
Biopsy significant 12 (30.4)
Multiple 98 (68.1%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ PSA: prostate-specific antigen, *: one single core positive biopsy containing a focus 3mm or less of moderately differentiated pro- state cancer (Gleason score≤6)
Table 2. Various preoperative parameters according to the number of positive-cores
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Single-core Multiple-core p-value ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ No. of patient (%) 46 (31.9%) 98 (68.1%)
Mean age (yrs) 65.5±5.6 64.8±6.2 0.480 Mean PSA (ng/ml) 8.2±6.1 10.9±9.6 0.082 Prostate volume (cc) 49.02±22.96 39.14±13.27 <0.001
Clinical stage 0.199
T1c 31 (67.4) 55 (56.1) ≥T2 15 (32.6) 43 (43.9)
% of core involved 17.5 30.1
<0.001 by tumor (range) (1.43-70.9) (5.32-81.25)
Biopsy Gleason score (%) <0.001
2-6 36 (78.3) 32 (32.7)
7 10 (21.7) 48 (49)
8-10 0 (0) 18 (18.4)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
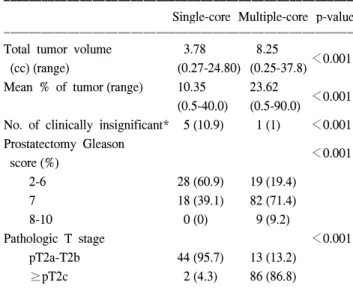
Table 3. Various postoperative parameters according to the number of positive cores
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Single-core Multiple-core p-value ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Total tumor volume 3.78 8.25
<0.001 (cc) (range) (0.27-24.80) (0.25-37.8) Mean % of tumor (range) 10.35 23.62
<0.001 (0.5-40.0) (0.5-90.0) No. of clinically insignificant* 5 (10.9) 1 (1) <0.001 Prostatectomy Gleason
<0.001 score (%)
2-6 28 (60.9) 19 (19.4)
7 18 (39.1) 82 (71.4)
8-10 0 (0) 9 (9.2)
Pathologic T stage <0.001
pT2a-T2b 44 (95.7) 13 (13.2)
≥pT2c 2 (4.3) 86 (86.8)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*: tumor volume<0.5cc, Gleason score<7, No extracapsular ex- tension
Table 4. Characteristic of patients with single-core positivity according to significance of biopsy
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Biopsy Biopsy
insignificant significant p-value
tumor* tumor
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ No. of patients (%) 32 (69.6) 14 (30.4)
Mean PSA (ng/ml) 6.9±4.0 11.1±8.9 0.120 No. of abnormal DRE (%) 7 (21.9) 3 (21.4) 0.648
% of core involved by tumor 10.5±6.5 33.4±15.9 <0.001
Clinical stage (%) 0.489
T1c 21 (65.6) 10 (71.4)
T2 11 (34.4) 4 (28.6)
% of core involved by tumor 10.5±6.5 33.4±15.9
Prostatectomy Gleason score (%) 0.040
2-6 24 (75) 4 (28.6)
7 8 (25) 10 (71.4)
Pathological stage 0.792
T2a 18 (56.3) 4 (28.6)
≥T2b 14 (43.8) 10 (71.4)
Extracapsular extension (%) 0 (0) 2 (14.3%) 0.088 No. of clinically
5 (15.6) 0 (0) 0.147 insignificance (%)
Mean % of tumor 8.7±9.5 13.9±10.6 0.028
Mean tumor volume 3.08 5.38 0.063
(cc) (range) (0.27-14.4) (1.40-24.8) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ PSA: prostate-specific antigen, DRE: digital rectal examination, *:
one single core positive biopsy containing a focus 3mm or less of moderately differentiated prostate cancer (Gleason score≤6)
양 군 간에 유의한 차이를 보였다 (p<0.05). 또한, 단일 core 양성군은 다발성 core 양성군에 비해 전립선절제술 후의 Gleason score, 병리학적 병기는 낮으며, 전립선 피막 외 침 범이 유의하게 적은 소견을 보였다 (p<0.05) (Table 2, 3).
단일 core 양성군에서 전립선 생검 조직에서 임상적으로 무의미한 암은 69.6% (32/46명)였고, 임상적으로 의미있는 암은 30.4% (14/46명)였다. 양 군 간에 평균 PSA, 직장수지 검사의 비정상 소견 및 임상적 병기의 차이는 없었다 (p>
0.05). 생검상 임상적으로 무의미한 암군은 의미있는 암군 에 비해 전립선절제술 후의 Gleason score는 낮았고, 평균 종양의 비율은 각각 8.7±9.5%, 13.9%±10.6%였고, 평균 종 양 무게는 각각 3.08g (0.27-14.4g), 5.38g (1.40-24.8g)으로, 임 상적으로 무의미한 암군에서 유의하게 적었다 (p<0.05). 전 립선 피막 외 침범은 양 군에서 각각 0% (0/32명), 14.3%
(2/14명)로, 임상적으로 무의미한 암군에서 통계적으로 유 의하지는 않았으나 낮은 피막 외 침범 경향을 보였다 (p=0.088). 양 군에서 술 후 임상적으로 무의미한 암은 생검 조직의 무의미한 암군에서 15.6% (5/32명)을 보였고 생검 조직에서 임상적으로 의미있는 암군에서는 0% (0/14명)를 보였으나 유의한 차이를 보이지 않았다 (p=0.147) (Table 4).
술 후 임상적으로 무의미한 암을 보인 6명 환자와 임상적 으로 의미있는 암 환자군에서 술 전 평균 PSA, 평균 종양 비율, 생검 Gleason score 및 임상적 병기는 차이를 보이지
않았으며 (p>0.05), 임상적으로 무의미한 암군에서 술 후 Gleason score, 병리학적 병기는 낮으며, 평균 종양 무게는 적었다 (p<0.05) (Table 5).
고 찰
혈청 PSA의 선별검사와 초음파 유도하 확대 전립선 생검 의 증가로 전립선암 발견의 급격한 증가와 더불어 진단 시 병기가 현저하게 저하되었다.1 선별 검사가 시행되면서 많 은 수의 환자들이 직장수지검사에서 촉지되지 않는 상태에 서 전립선암이 발견되었으며, 이는 직장수지검사를 통한 진단보다 전립선암이 5년에서 10년 이상 조기에 발견된 것 이다.18 또한, 전립선 생검의 적응증이 되는 PSA의 기준치 도 점차 낮아지게 되면서, 이를 통하여 발견된 환자들에게 조기에 전립선적출술을 시행한 결과 평균 종양 무게가 현 저한 감소를 보였으며, 분화도가 좋으며 종양의 용적이 0.2-0.5ml 미만인 임상적으로 무의미한 암의 발견도 증가하 게 되었다.2,19 이와 같이, PSA의 확대 실시와 생검의 적응증 이 4ng/ml에서 2.5-3.0ng/ml으로 낮아지며,20 경직장초음파 유도하 확대 전립선 생검의 시행으로 분화도가 좋은, 적은 용적의 종양의 발견이 증가함에 따라 이들 환자들에 대한 치료로 대기관찰요법에 대한 관심도 증가하게 되었다.5-7 특 히, 전립선 생검에서 단일 core에서만 암이 발견되며 분화 도가 좋은 적은 용적의 종양에 대한 비율이 증가하면서 이 들의 임상적 의의 및 치료에 대한 관심이 증가하였 다.2,10,11,13,21,22
임상적으로 무의미한 암에 대한 규명을 위한 많은 연구 가 있어 왔으나 100% 신뢰할 만한 인자를 발견하지는 못하 였다.14-16,23,24
Epstein 등14은 임상병기가 T1c인 환자에서 종 양이 0.2cc 미만이고 Gleason score가 7 미만인 경우에 임상 적으로 무의미한 암이라고 정의하고, PSA 밀도, 종양의 등 급과 단일 core에서 종양의 정도를 이용한 예측 모형을 제 시하였으나 73%에서만 임상적으로 무의미한 암을 예측할 수 있었다. Stamey 등23은 종양이 0.5ml 미만이고 Gleason score가 7 미만일 때, 이들 환자에서 PSA의 긴 두 배 상승 기간에 근거하여 임상적으로 무의미한 암이라고 정의하였 다. 그러나 이들의 다른 보고에 의하면 Gleason grade가 3 이하인 종양에서도 생화학적 재발이 5.6%에서 발생하여, 이들의 정의도 임상적으로 무의미한 암의 정의하는데 한계 가 있다.24 Gardner 등15은 좀더 엄격한 기준으로 전체 생검 에서 종양의 비율이 5% 미만이고 Gleason grade가 3 이하인 경우를 임상적으로 무의미한 암이라 정의하였다. Terris 등16 은 단일 core에서 암이 발견되고, Gleason score가 6 이하이 고, 종양 길이가 3mm 미만인 경우에 임상적으로 무의미한 Table 5. Characteristic of patients with single-core positivity
according to the clinical significance
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Insignificant Significant
p-value
tumor tumor
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ No. of patients (%) 5 (10.8) 41 (89.2)
Mean PSA (ng/ml) 8.2±3.5 8.2±6.4 0.370
% of core involved by tumor 10.5±5.3 18.4±15.2 0.284
Biopsy Gleason score (%) 0.275
2-6 6 (100) 31 (75.6)
7 0 (0) 10 (24.4)
Clinical stage 0.709
T1c 3 (60) 28 (68.3)
T2 2 (40) 13 (31.7)
RRP Gleason score (%) 0.072
2-6 5 (100) 23 (56.1)
7 0 (0) 18 (43.9)
Pathological stage 0.013
T2a 5 (100) 17 (68.3)
≥T2b 0 (0) 24 (31.7)
Mean % of tumor 0.7±0.27 11.5±10.0 <0.001 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ RRP: radical retropubic prostatectomy
암이라고 정의하였다. 저자들이 Terris 등의 정의를 임상적 으로 무의미한 암의 정의로 선택한 이유는 이에 대한 100%
신뢰할 만한 정의가 없으며, 생검에서 단일 core에서만 암 이 발견되는 환자가 많아지고, 쉽게 정의할 수 있기 때문이 었다.
경직장초음파 유도하 전립선 생검에서 전립선암으로 진 단된 환자가 분화도가 좋으며, 단일 core의 일부에서만 암 이 발견되는 경우 치료를 결정하는 데 많은 어려움에 직면 하게 된다. 최근 일부 연구에서는 이들 환자에 대한 치료로 대기관찰요법의 시행을 주장하고 있다.5-7,12 그러나 다른 연 구에서는 전립선 생검의 적은 종양 용적은 전체 전립선에 서의 적은 용적의 종양을 의미하지 않으며 대부분 임상적 으로 의미 있는 암이라 보고하고 있다.8-12 D'Amico 등11은 전립선 생검에서 단일 core의 5% 미만에서만 암이 발견된 환자 66명의 전립선적출술 시행 결과를 보고하였는데, 이 들 환자는 양호한 병리학적 특성을 보이나, 92%에서 최소 한 전립선의 한쪽 엽의 반 이상에서 종양이 발견되고, 10%
에서 5년 내에 생화학적 재발의 소견을 보이므로, 전립선 생검의 적은 종양 용적은 임상적으로 무의미한 암을 의미 하지 않는다고 주장하였다. 다른 연구에서 생검조직의 단 일 core에서 5% 미만에서 암이 발견된 경우 임상적으로 무 의미한 암은 단지 7%에 불과하고,9 단일 core의 0.5mm 미만 에서만 암이 발견된 환자의 2/3에서 임상적으로 의미있는 암이므로, 전립선 생검 소견만으로 임상적으로 무의미한 암을 보장할 수 없다고 보고하였다.12 Boccon-Gibod 등13의 최근 연구에서 단일 core의 3mm 미만에서만 암이 발견되 고, Gleason score가 6 이하인 환자에서 30%에서만 임상적 으로 무의미한 암이 발견되나, 술 전에 이를 구별할 수 있는 특성은 없다고 보고하였다. 저자들의 결과에서도 단일 core 의 3mm 미만에서 암이 발견되고, Gleason score가 6 이하인 환자에서 임상적으로 무의미한 암은 15.6%에서만 발견이 되었으며, 이는 다른 연구와도 유사한 결과를 보였다.
생검조직에서 단일 core에서만 암이 발견된 환자의 종양 용적이 적게 평가되는 것에 대한 가장 가능성 있는 설명은 경직장초음파 유도하 전립선 생검 시 발생되는 조직 채취 의 오류 발생이다. 정상적인 전립선 용적을 가지고 있는 환 자에 대한 전립선 생검을 시행한다고 가정하면, 전립선과 직장은 약 30x30mm 정도의 면적을 접하고 있으나, 전립선 생검에 사용되는 18G 침은 직경이 1mm 정도로 12부위 생 검을 시행하여도 3x4mm의 면적에서만 조직의 채취가 가능 하고, 또한 생검 침은 길이가 일반적으로 1.0-1.5cm의 길이 이므로, 침이 도달하지 못하는 전립선 전방에 대한 생검 시 행에 제한이 있어 실제 종양의 무게와 차이를 보일 수 있다.
또한 고등급의 전립선암은 적은 종양 용적에서도 증가된
PSA를 보일 수 있는데, 이러한 환자들에서 PSA 선별검사를 통한 전립선 생검을 시행할 경우 종양을 발견하지 못할 수 있다.11 이러한 조직 채취의 오류로 인하여 생검조직에서 단 일 core에서만 암이 발견된 경우, 적은 양의 종양이라 할지 라도 반드시 임상적으로 무의미한 암이라고 구별하는 데 어려움이 발생하게 된다.
종양의 무게는 전립선암의 예후 인자 중의 하나로 알려 져 있다.24 전립선 생검 조직을 이용한 여러 연구에서 생검 중 최대 종양길이,25 전체 생검에서 양성 검체 수의 비율26 및 양성 생검 중 종양 비율27 등은 전립선적출술 후 병리학 적 병기, 생화학적 재발 및 예후 등과 관련이 있는 것으로 알려져 있다. 여러 연구에서 생검조직에서 단일 core에서만 암이 발견된 환자군은 많은 수에서 Gleason score는 6 이하 이고, 종양은 전립선 내에 국한되고, 절개면 음성 소견을 보 이며, 생화학적으로 재발 소견을 보이는 경우는 낮은 것으 로 보고하고 있다.9,11,28 단일 core에서 암이 발견된 환자군은 선별검사를 통하여 전립선암이 진행되기 전에 조기 발견되 고, 종양의 무게가 적어 다발성 core에서 암이 발견된 환자 군에 비해 술 후 양호한 병리학적 소견을 보이는 것으로 생각된다. 저자들의 결과에서도 단일 core에서 암이 발견된 환자군은 다발성 core에서 암이 발견된 환자군에 비해 술 후 Gleason score와 병리학적 병기는 낮았으며 전립선 피막 외 침윤이 있는 경우는 4.3%에 불과한 양호한 병리학적 소 견을 보였다.
저자들의 연구결과 전립선 생검을 통하여 발견된 단일 core에서 암이 발견된 환자의 10.9%에서만 임상적으로 무 의미한 암이 발견되었다. 또한 단일 core의 3mm 미만에서 만 암이 발견되고, Gleason score가 6 미만인 환자에서도 임 상적으로 무의미한 암은 15.6%에 불과하였으며, 술 전에 이 를 예측하는 데 어려움이 있었다. 그러나 이들 환자들은 다 발성 core에서 암이 발견된 환자군에 비하여 양호한 병리학 적 소견을 보이므로, 단일 core에서 암이 발견된 환자에게 적극적인 치료를 시행할 경우 보다 좋은 결과를 얻을 수 있으리라 생각한다. 향후 이들 환자를 대상으로 한 장기 추 적 관찰에 대한 연구가 추가적으로 필요하리라 생각한다.
결 론
혈청 PSA의 선별검사와 초음파 유도하 확대 전립선 생검 을 통하여 발견된 단일 core에서만 암이 발견된 전립선암은 대부분이 임상적으로 의미있는 암이다. 또한 단일 core의 일부에서만 암이 발견되고, 저등급의 Gleason core를 보이 는 경우에도 임상적으로 무의미한 암은 15.6%에 불과하였 다. 그러나 단일 core에서 암이 발견된 경우 Gleason score,
종양의 무게, 병리학적 병기 및 전립선 피막 외 침윤 등의 측면에서 다발성 core에서 암이 발견된 환자군에 비해 양호 한 결과를 보인다. 그러므로 전립선 생검의 일부에서만 암 이 발견되었다 하더라도 임상적으로 무의미한 암을 의미하 지 않으므로 적극적인 치료가 필요할 것으로 생각한다.
REFERENCES
1. Brawer MK. Prostate-specific antigen: current status. CA Cancer J Clin 1999;49:264-81
2. Cooperberg MR, Broering JM, Litwin MS, Lubeck DP, Mehta SS, Henning JM, et al. The contemporary management of prostate cancer in the United States: lessons from the cancer of the prostate strategic urologic research endeavor (CapSURE), a national disease registry. J Urol 2004;171:1393-401 3. Holmberg L, Bill-Axelson A, Helgesen F, Salo JO, Folmerz
P, Haggman M, et al. A randomized trial comparing radical prostatectomy with watchful waiting in early prostate cancer.
N Engl J Med 2002;347:781-9
4. Wei JT, Dunn RL, Sandler HM, McLaughlin PW, Montie JE, Litwin MS, et al. Comprehensive comparison of health-related quality of life after contemporary therapies for localized pros- tate cancer. J Clin Oncol 2002;20:557-66
5. Khan MA, Partin AW, Carter HB. Expectant management of localized prostate cancer. Urology 2003;62:793-9
6. Klotz L. Active surveillance with selective delayed interven- tion using PSA doubling time for good risk prostate cancer.
Eur Urol 2005;47:16-21
7. Parker C. Active surveillance: towards a new paradigm in the management of early prostate cancer. Lancet Oncol 2004;5:
101-6
8. Anast JW, Andriole GL, Bismar TA, Yan Y, Humphrey PA.
Relating biopsy and clinical variables to radical prostatectomy findings: can insignificant and advanced prostate cancer be predicted in a screening population? Urology 2004;64:544-50 9. Lee AK, Doytchinova T, Chen MH, Renshaw AA, Weinstein
M, Richie JP, et al. Can the core length involved with prostate cancer identify clinically insignificant disease in low risk patients diagnosed on the basis of a single positive core? Urol Oncol 2003;21:123-7
10. Ravery V, Szabo J, Toublanc M, Boccon-Gibod LA, Billebaud T, Hermieu JF, et al. A single positive prostate biopsy in six does not predict a low-volume prostate tumour. Br J Urol 1996;77:724-8
11. D'Amico AV, Wu Y, Chen MH, Nash M, Renshaw AA, Richie JP. Pathologic findings and prostate specific antigen outcome after radical prostatectomy for patients diagnosed on the basis of a single microscopic focus of prostate carcinoma with a gleason score </=7. Cancer 2000;89:1810-7 12. Allan RW, Sanderson H, Epstein JI. Correlation of minute (0.5
MM or less) focus of prostate adenocarcinoma on needle
biopsy with radical prostatectomy specimen: role of prostate specific antigen density. J Urol 2003;170:370-2
13. Boccon-Gibod LM, Dumonceau O, Toublanc M, Ravery V, Boccon-Gibod LA. Micro-focal prostate cancer: a comparison of biopsy and radical prostatectomy specimen features. Eur Urol 2005;48:895-9
14. Epstein JI, Walsh PC, Carmichael M, Brendler CB. Pathologic and clinical findings to predict tumor extent of nonpalpable (stage T1c) prostate cancer. JAMA 1994;271:368-74 15. Gardner TA, Lemer ML, Schlegel PN, Waldbaum RS, Vaug-
han ED Jr, Steckel J. Microfocal prostate cancer: biopsy cancer volume does not predict actual tumour volume. Br J Urol 1998;81:839-43
16. Terris MK, McNeal JE, Stamey TA. Detection of clinically significant prostate cancer by transrectal ultrasound-guided systematic biopsies. J Urol 1992;148:829-32
17. Gore JL, Shariat SF, Miles BJ, Kadmon D, Jiang N, Wheeler TM, et al. Optimal combinations of systematic sextant and laterally directed biopsies for the detection of prostate cancer.
J Urol 2001;165:1554-9
18. Gann PH, Hennekens CH, Stampfer MJ. A prospective evalua- tion of plasma prostate-specific antigen for detection of pro- static cancer. JAMA 1995;273:289-94
19. Hoedemaeker RF, Rietbergen JB, Kranse R, Schroder FH, van der Kwast TH. Histopathological prostate cancer characteri- stics at radical prostatectomy after population based screening.
J Urol 2000;164:411-5
20. Lee SE. Diagnosis of prostate cancer. Korean J Urol 2004;
45:197-208
21. Wang X, Brannigan RE, Rademaker AW, McVary KT, Oyasu R. One core positive prostate biopsy is a poor predictor of cancer volume in the radical prostatectomy specimen. J Urol 1997;158:1431-5
22. Hoedemaeker RF, Van der Kwast TH, Schroder FH. The clinical significance of a small focus of well-differentiated carcinoma at prostate biopsy. BJU Int 2003;92(Suppl 2):92-6 23. Stamey TA, Freiha FS, McNeal JE, Redwine EA, Whittemore AS, Schmid HP. Localized prostate cancer. Relationship of tumor volume to clinical significance for treatment of prostate cancer. Cancer 1993;71(3 Suppl):933-8
24. Stamey TA, McNeal JE, Yemoto CM, Sigal BM, Johnstone IM. Biological determinants of cancer progression in men with prostate cancer. JAMA 1999;281:1395-400
25. Nelson CP, Rubin MA, Strawderman M, Montie JE, Sanda MG. Preoperative parameters for predicting early prostate can- cer recurrence after radical prostatectomy. Urology 2002;59:
740-5
26. D'Amico AV, Whittington R, Malkowicz SB, Schultz D, Fondurulia J, Chen MH, et al. Clinical utility of the percentage of positive prostate biopsies in defining biochemical outcome after radical prostatectomy for patients with clinically localized prostate cancer. J Clin Oncol 2000;18:1164-72
27. Grossklaus DJ, Coffey CS, Shappell SB, Jack GS, Chang SS, Cookson MS. Percent of cancer in the biopsy set predicts pathological findings after prostatectomy. J Urol 2002;167:
2032-5
28. Miyake H, Ono Y, Park SJ, Hara I, Eto H. Pathological findings of radical prostatectomy specimens in Japanese men diagnosed on single core positive prostate biopsy in eight with a Gleason score less than 4. Int J Urol 2003;10:383-6