INTRODUCTION
While the term ‘perforator’ has been used previously, the terminology and concept of ‘perforator flap’ were introduced in 1989, when Koshima and Soeda1 reported a skin flap from the abdominal wall, which did not include the rectus abdominis muscle. The authors called this a ‘paraumbilical perforator’ flap, which eventually became what is today referred to as the deep inferior epigastric perforator flap. Subsequent to the initial report, perforator flaps were found to decrease donor site morbidity while allowing for control of flap volume and shape to cover a wide variety of tissue defects. These advantages outweighed the technical challenges associated with manipulation of small vessels, and perforator flaps became a popular study subject within the microsurgical literature.
There are several types of perforators. Nakajima et al.2 divided perforator vessels into direct and indirect perforators and further divided direct perforators into 4 subtypes: direct cutaneous branch of a muscular vessel, septocutaneous perforator, direct
cutaneous perforator, and direct septocutaneous perforator, and indirect perforators into 2 subtypes: musculocutaneous perforator and perforating branch of a muscular vessel. This classification for the perforator vessels was translated into perforator flaps in the microsurgical literature, with all kinds of flaps being considered ‘perforator flaps’ for the mere fact that the flap contained a perforating vessel of some sort. To avoid confusion, Wei et al.3 suggested limiting the definition of perforator flaps to only those flaps containing vascular pedicles made of vessels that perforate through a muscular layer. It is in this historical context that the microsurgical nomenclature adopted two definitions of perforator flaps. In the wider sense, all flaps supplied by perforator vessels can be considered perforator flaps. In the narrower sense, only flaps supplied by muscle-perforating vessels are considered perforator flaps.
In hand surgery literature, the ‘perforator flap’ terminology first appears in publication by Koshima et al.,4 in which the authors introduced small digital skin flaps supplied by short branches of digital arteries and named this as ‘digital artery
Digital Artery Perforator Flaps
Kwang Seog Kim
Department of Plastic and Reconstructive Surgery, Chonnam National University Medical School, Gwangju, Korea
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2015 by the Korean Society for Microsurgery. All Rights Reserved.
Received November 19, 2015 Accepted November 19, 2015
*Correspondence to: Kwang Seog Kim Department of Plastic and Reconstructive Surgery, Chonnam National University Medical School, 42 Jebong-ro, Dong-gu, Gwangju 61469, Korea
Tel: +82-62-220-6354, 6352 Fax: +82-62-220-6357 E-mail: [email protected] Financial support: None.
Conflict of interest: None.
In the hand, few vessels can be classified as ‘perforators’. Even today, the debate continues on whether or not branches of the digital artery should be considered as perforators.
However, ‘perforator’ and ‘perforator flaps’ have become extremely popular within the microsurgery literature, and as such, the terminology has found widespread adoption across the hand surgery field. The finger is the most important sensory organ for tactile stimulation. The glabrous skin can be distinguished between the fingertip and the proximal tissue, with the fingertip having a higher functional and, therefore, reconstructive priority. Thus, sacrifice of the proximal glabrous skin can be justified in the reconstruction of fingertip defects. In this paper, the author reviews two flaps, ‘lateral digital artery perforator flap’ and ‘volar digital artery perforator flap’, both of which uses short branches of the digital artery as a vascular pedicle and are useful in fingertip construction.
Key Words: Perforator flap, Island flap, Finger, Hand, Reconstructive surgical procedure
ARMS
Archieves of Reconstructive Microsurgery http://dx.doi.org/10.15596/ARMS.2015.24.2.50perforator flap’. In hand anatomy, few vessels can qualify as true perforators of the traditional sense, and it is not clear whether the branches of digital artery can be considered as perforator vessels. However, ‘perforator’ and ‘perforator flaps’ had anointed speakers and writers with a supernatural ability to persuade any and all audience within the microsurgery literature, and as such, the terminology has found widespread adoption across the field.4-15
Fingertip amputation is one of the most common upper extremity injuries. Replantation of the amputated fingertip is the most ideal way to preserve function and shape of the digit, but replantation is not always possible. Many alternate methods have been developed to address fingertip defects – each with inherent advantages and disadvantages. Among various options, the replacement tissue that is most similar within the injured finger stump is found on the lateral and volar surfaces, and there are two digital artery perforator flaps that use this glabrous skin. Koshima et al.4 had reported a digital artery perforator flap based on small lateral branches of the digital artery (i.e.,
‘lateral digital artery perforator flap’). Our group has previously reported a volar flap based on the transverse palmar branch of the digital artery (i.e., ‘volar digital artery perforator flap’).10 In this review, the author wishes to discuss these two flaps in the reconstruction of fingertip defects.
LATERAL DIGITAL ARTERY PERFORATOR FLAP
The lateral digital artery perforator flap is indicated in several contexts within fingertip amputations. In the immediate post- injury setting, it can be used to resurface the defect, where the amputated portion is either not available or is not appropriate for replantation. This is more appropriate for patients who wish to resume social and occupational activity as early as possible. According to Koshima et al.,4 the flap also has a limited indication for temporary coverage, until a time when secondary operations can be performed to improve the aesthetic and function.
As with all flaps, the vascular anatomy determines the flap dimension and surgical design for this perforator flap. Grossly, the digital artery gives off many lateral branches. Because these branches perforate through a thin fascia and continue as arterioles into the subdermal layer, Koshima et al.4 argued for
a definition of perforator as opposed to that of a simple arterial branch. A network of arterioles and venules exists between each of these perforators, along the midlateral line and within the subcutaneous tissue. The venous outflow is divided amongst the venules in the dorsal and volar cutaneous venous systems.
The nervous system is composed of abundant vascular network and is connected to the subdermal plexus. This flap contains only the lateral digital artery perforator and the venules contained within the small cuff of fatty tissue in the perforator pedicle, but it does not contain the larger, main perforator branches such as the transverse digital palmar arch arteries.
The flap is designed along the midlateral line. One advantage of the lateral digital artery perforator flap is that primary closure of the donor site is possible for narrower flap designs. The largest dimensions reported for this flap is 2.5 cm by 4 cm.4-
9 Koshima et al.4 reported primary closure of 2-cm wide flaps raised from the third digit. In our experience, primary closure of 2-cm wide donor site defect proved difficult in average height Korean adult patients, and the tension created from such closure invariably threatened viability of the rotated flap. If primary closure is not possible, partial closure with secondary intention or skin graft is recommended.
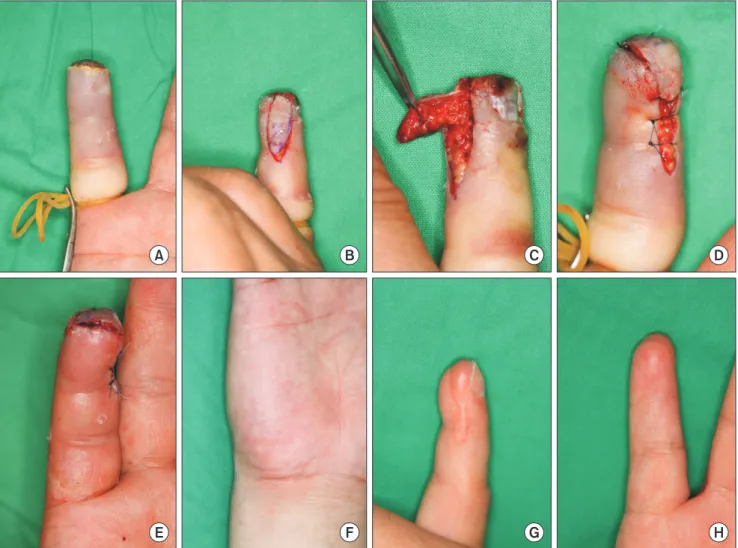
Upon digital block, the skin is incised along the design. The flap is elevated along the subcutaneous layer containing the neurovascular bundle. The perforator most distal, or closest to the defect, is preserved as the pedicle. The more proximal perforators are ligated or cauterized. The subcutaneous tissue contains superficial arterioles, which can provide sufficient blood flow to a flap. In the absence of readily identifiable perforator artery, a cuff of fatty tissue should be included in the flap base to incorporate these arterioles. The island flap is rotated about the perforator axis and inset into the distal fingertip wound. The donor site is either closed primarily or covered with a skin graft (Fig. 1).
Many of the advantages of this flap are related to its size.
Because the flap is so small, it can survive on the smallest of perforator arteries. This decreases the need for extensive neurovascular dissection and makes unnecessary the sacrifice of the digital neurovascular bundle. The smallness of the flap also leads to decreased operative time and anesthesia. Flap circulation is robust because of the short pedicle. Primary closure is possible for narrower flap designs. Other advantages include the adequate padding of the fingertip and satisfactory
sensory recovery.
The disadvantages are the need for significantly magnified view of the surgical field (to view the small perforator), potential for venous congestion after flap rotation, and the potential for postoperative pain syndrome from compression of the digital nerve. To avoid the latter problem, the flap should not be made too large. In our experience, leaving a bit of fatty tissue on the donor site surface is helpful in separating the nerve traveling just deep to this surface and the base of the skin graft.
VOLAR (or PALMAR) DIGITAL ARTERY PERFORATOR FLAP
The volar digital artery perforator flap is indicated for all
glabrous surface defects of digits, and digital surface defects not amenable to other forms of local flaps. Unlike the lateral digital artery perforator flap, this flap represents a definitive option for reconstruction of fingertip defects.
In each digit, a minimum of three vascular arches anastomose between the radial and ulnar digital arteries. These are called transverse digital palmar arches and are found in constant anatomic locations at the insertion sites of proximal cruciate ligament, middle cruciate ligament, and flexor digitorum profundus tendon.16 Among these, the distal and middle arches are similar in diameter, and both are larger than the proximal arch. From the digital arteries and these palmar arches, the perforators branch and form the vascular network that supplies blood to the skin. In most cases, the digital artery does not
A B C D
E F G H
Fig. 1. A patient with complete fingertip amputation of the right little finger. (A) Preoperative view of the defect. (B) Intraoperative view of design and skin incision of a lateral digital artery perforator flap. (C) Intraoperative view showing the elevated flap. (D) Intraoperative view showing the flap transposed to the defect and adipose tissue covering the digital artery and nerve within the donor wound after approximation. (E) Immediate postoperative view. (F) Postoperative view at 3 months. The donor site scar was aesthetically acceptable. (G, H) Postoperative views at 4 months.
accompany a vein but is surrounded by venules. The volar digital artery perforator flap is supplied by a transverse palmar arch and its branches and is drained by the venules surrounding the perforator vessels.
This flap can be raised from proximal, middle, or distal portion of the volar surface to suit the needs of the fingertip injury. Once the defect margin is debrided, the flap is designed according to the shape and size of the defect. The distal portion of the flap should incorporate the most appropriate perforator vessel. In theory, it is possible to raise the whole volar surface of a digit, for a 2.5 cm by 5.0 cm flap. However, most volar digital artery perforator flaps used for fingertip reconstruction are smaller than 2.0 cm by 3.5 cm.12
Upon digital block and tourniquet application, the skin is
incised and dissected from the side opposite from vascular pedicle. The flap is elevated under magnification. The opposite end of the digital palmar arch is revealed first during this dissection, and the arch end to be used as the pedicle base is located in a mirror location. The paratenon should be left alone, to allow skin graft take in the wound base of the donor site. The perforator is dissected where it branches off the arch.
If dissection of the perforator proves to be difficult, it is better to divert the surgeon’s attention and energy by allowing half of the arch to be buried in the flap and to ligate the arch to free the flap. In such situations, the dissection is carried out such that the arch and digital nerve are incorporated into the flap.
This dissection is continued until the arch and nerve are traced back to the main digital artery and nerve, at which point the
A B C D
E F C D
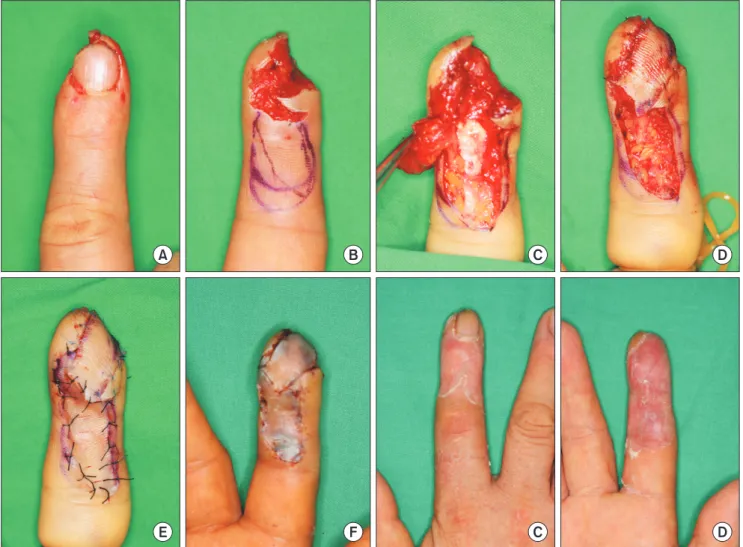
Fig. 2. A patient with a pulp defect of the right index fingertip. (A) Preoperative view of the defect. (B) Preoperative view of the volar digital artery perforator flap design. (C) Intraoperative view showing the elevated flap. (D) Intraoperative view showing the flap transposed to the defect. The adipose tissue is covering the paratenon at the flap donor site. (E) Immediate postoperative view. (F) Postoperative view at 1 week. (G, H) Postoperative views at 1 month.
Grayson’s ligament is divided. The connective fibers from the pedicle to bone and tendon are released, in order to decrease twisting and tension on the pedicle. Flap mobility can be improved by dissecting the pedicle more proximal to the point where the arch branches from the main trunk of the digital artery. While dissecting, a circumferential cuff of fatty tissue is left around the pedicle to preserve the venules within the fatty tissue. The raised flap is rotated and inset into the fingertip defect. The donor site is covered with a skin graft. To avoid compression of vascular pedicle, tie-over bolster dressing is not applied over the skin graft near the vascular pedicle (Fig. 2).
Postoperatively, the involved limb is elevated to decrease venous congestion. To allow for skin graft take, the splint is maintained for 1 week. Passive and active range of motion exercises are begun shortly after this to avoid joint stiffening.
The dressing is maintained for 2 weeks to protect the surgical site.
One advantage of this flap is that the palmar arch provides robust blood supply while the digital artery remains preserved.
Sensory recovery is satisfactory, owing to the fact that the flap incorporates branches of the digital nerve. In certain cases, near- normal sensation is recovered soon after the operation, and satisfactory level of sensory recovery is possible even in defects from severe injuries. The reconstruction can be performed within the same surgical field using a very similar tissue for resurfacing the defect. Even for a distally based pedicle, the blood flow maintains a norm grade pattern and, as such, venous congestion is not as frequent. Because the perforator branch can be traced back to the digital artery, the flap can be raised in many different configurations, shapes, and sizes.
A disadvantage of the volar digital artery perforator flap is the need for magnification. Because the volar surface of the finger is used as donor, flexion contraction is a concern. This can become more of a problem if the skin graft fails to take.
To minimize the risk of contraction, the paratenon should be protected during the operation, and self-adhesive silicone gel sheet and temporary splint are used for several months. Injury to the distal arch requires the use of a more proximal arch or its perforator vessel. In the lateral aspect of a digit, the perforator is distributed along the course of the digital artery. In the volar aspect of the digit, however, the perforators mainly originate from the arch. The rest originate directly from the digital artery and have a more random distribution. The perforators from
the arch are more reliable than these randomly distributed perforators.
PERFORATOR ROTATION
These two flaps represent procedures in which each flap is rotated about an extremely short perforator pedicle, and can be classified as perforator-based rotation island flaps.17-21 In such flaps, rotation about the pedicle can interrupt the blood flow. In rat models, rotations of less than 360 and 180 degrees did not affect flap survivability of groin island flap and perforator flap, respectively.20,21 Likewise, perforator rotation of less than 180 degrees has been reported not to affect flap survival rate.19
In the context of microanastomosed vessels, however, patency rate is known to be proportional to the degree of pedicle rotation.22 Although no microanstomosis is performed for these perforator-based rotation island flaps, the perforator pedicles are extremely short and can be twisted shut with minor flap rotation. Strategies in minimizing pedicle obstruction of larger perforator flaps include dissecting at least 1 cm of perforator pedicle, minimizing the extent of flap rotation (less than 180 degrees), and releasing the pedicle free from fibrous connections that tether the perforator to tendons and bones.19 The two flaps discussed so far have rotations less than 180 degrees, but have pedicles which are at best few millimeters long. As such, the flap must be monitored after rotation to ensure that there are no patency issues.
CONCLUSION
Fingertip is the most important tactile organ in the body and is important in maintaining digital strength. While the rest of volar and lateral surface on a digit can be considered to be a high value real estate, these two perforator-based rotation island flaps from the glabrous skin allow for reconstruction of the fingertip defect without sacrificing either the main trunk of the digital artery or the nerve. The flaps provide skin of extremely similar quality to the injury defect, with sensory recovery that is appropriate for fingertip reconstruction.
ACKNOWLEDGEMENTS
This article was presented at the 2009 Joint Symposium of
the Korean Society for Microsurgery and the Korean Society for Surgery of the Hand.
REFERENCES
1. Koshima I, Soeda S. Inferior epigastric artery skin flaps without rectus abdominis muscle. Br J Plast Surg 1989;42:645-8.
2. Nakajima H, Fujino T, Adachi S. A new concept of vascular supply to the skin and classification of skin flaps according to their vascularization. Ann Plast Surg 1986;16:1-19.
3. Wei FC, Jain V, Suominen S, Chen HC. Confusion among perforator flaps: what is a true perforator flap? Plast Reconstr Surg 2001;107:874-6.
4. Koshima I, Urushibara K, Fukuda N, Ohkochi M, Nagase T, Gonda K, et al. Digital artery perforator flaps for fingertip reconstructions. Plast Reconstr Surg 2006;118:1579-84.
5. Cho PD, Moon MS, Shin KS. Comparison between the digital artery perforator flaps and the distant flaps within hand. J Korean Soc Plast Reconstr Surg 2010;37:52-8.
6. Mitsunaga N, Mihara M, Koshima I, Gonda K, Takuya I, Kato H, et al. Digital artery perforator (DAP) flaps: modifications for fingertip and finger stump reconstruction. J Plast Reconstr Aesthet Surg 2010;63:1312-7.
7. Basat SO, Uğurlu AM, Aydın A, Aksan T. Digital artery perforator flaps: an easy and reliable choice for fingertip amputation reconstruction. Acta Orthop Traumatol Turc 2013;
47:250-4.
8. Ozcanli H, Coskunfirat OK, Bektas G, Cavit A. Innervated digital artery perforator flap. J Hand Surg Am 2013;38:350-6.
9. Özcanli H, Bektaş G, Cavit A, Duymaz A, Coşkunfırat OK.
Reconstruction of fingertip defects with digital artery perforator flap. Acta Orthop Traumatol Turc 2015;49:18-22.
10. Kim KS, Yoo SI, Kim DY, Lee SY, Cho BH. Fingertip reconstruction using a volar flap based on the transverse palmar
branch of the digital artery. Ann Plast Surg 2001;47:263-8.
11. Saint-Cyr M, Gupta A. Hand flaps. In: Blondeel PN, Morris SF, Hallock GG, Neligan PC, editors. Perforator flaps. Vol. 1. St.
Louis: Quality Medical Publishing; 2006. p. 319-56.
12. Kim KS. Modified palmar skin flap to the fingertip. In: Strauch B, Vasconez LO, Hall-Findlay EJ, Lee BT, editors. Grabb’s encyclopedia of flaps. Vol. 2. 3rd ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2009. p. 797-9.
13. Kim KS, Hwang JH. Radial midpalmar island flap. Plast Reconstr Surg 2005;116:1332-9.
14. Kim KS, Kim ES, Hwang JH, Lee SY. Thumb reconstruction using the radial midpalmar (perforator-based) island flap (distal thenar perforator-based island flap). Plast Reconstr Surg 2010;
125:601-8.
15. Kim KS, Kim ES, Hwang JH, Lee SY. Fingertip reconstruction using the hypothenar perforator free flap. J Plast Reconstr Aesthet Surg 2013;66:1263-70.
16. Strauch B, de Moura W. Arterial system of the fingers. J Hand Surg Am 1990;15:148-54.
17. Cavadas PC, Teran-Saavedra PP. Combined latissimus dorsi- thoracodorsal artery perforator free flap: the "razor flap". J Reconstr Microsurg 2002;18:29-31.
18. Hallock GG. The propeller flap version of the adductor muscle perforator flap for coverage of ischial or trochanteric pressure sores. Ann Plast Surg 2006;56:540-2.
19. Hwang JH, Kim ES, Kim KS, Kim DY, Lee SY. Latissimus dorsi muscle and its short perforator-based skin compound free flap.
Ann Plast Surg 2007;58:381-7.
20. Demirseren ME, Yenidunya MO, Yenidunya S. Island rat groin flaps with twisted pedicles. Plast Reconstr Surg 2004;114:1190-4.
21. Demir A, Acar M, Yildz L, Karacalar A. The effect of twisting on perforator flap viability: an experimental study in rats. Ann Plast Surg 2006;56:186-9.
22. Salgarello M, Lahoud P, Selvaggi G, Gentileschi S, Sturla M, Farallo E. The effect of twisting on microanastomotic patency of arteries and veins in a rat model. Ann Plast Surg 2001;47:643-6.