Abstract
Inferior alveolar nerve (IAN) block or infiltration anesthesia can be used during the dental implant placement in the posterior mandibular region. The IAN block eliminates all somatosensory perceptions of the mandible and assures patient comfort during the placement of implants, while complications or nerve damages by implants can occur when patients cannot feel pain. Infiltrations may allow the patients to warn the surgeons when the IAN is in danger of being damaged, while it may also cause discomforts or pains during the implantation. In this study, we present a case of IAN block and infiltration in a female patient who had three teeth missing in each posterior mandibular region. Block anesthesia was used in the right side, while infiltration anesthesia used in the left side. After the surgery, the patient was instructed to record her discomfort or pain during the anesthesia or operation on the visual analogue scale. The patient preferred infiltration to IAN block as only anesthesia is being evaluated, because she considered that the acute pain by infiltration was more endurable than the dull pain by block. Nevertheless, she preferred block anesthesia when including implant placement during the evaluation because she had felt pain during preparation of the placement site under infiltration anesthesia.
Key Words: block anesthesia, cone-beam computed tomography, dental implant, inferior alveolar nerve, infiltration anesthesia
Block Anesthesia versus Infiltration Anesthesia of Inferior Alveolar Nerve When Placing Dental Implants in the Posterior Mandibular Region
Seong-June Park, Nam-Seok Chee, Min-Ho Son, Eoy-Jung Lee, Soo-Woon Lee
Department of Oral and Maxillofacial Surgery, Inje University Haeundae Paik Hospital, Busan, Korea
ISSN 1229-5418 Implantology 2014; 18(1): 30~36
Reprint requests: Soo-Woon Lee
Department of Oral and Maxillofacial Surgery, Inje University Haeundae Paik Hospital, 875, Haeun-daero, Haeundae-gu, Busan 612-896, Korea Tel: 82-51-797-2151, Fax: 82-51-797-2154
E-mail: [email protected]
Received for publication: February 17, 2014 Accepted for publication: February 22, 2014
Copyright © 2014. The Korean Academy of Oral & Maxillofacial Implantology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits
II Case Report
A 55-year-old woman underwent dental implant surgery in both sides of mandible. The patient missed the canine, the second premolar, the first molar and the second molar in the left side, and the first premo- lar, the first molar and the second molar in the right side. The patient showed good general health and had been treated for existing periodontal disease. Before the surgery, cone-beam computed tomography (CBCT) images were taken for measurement of the accurate height and width of the implant placement site.
Implant placement for the canine, the second premolar and the first molar in the left side was first planned, and infiltration anesthesia was used. Four carpules of 2% lidocaine (1.8 ml) with 1 : 100,000 epinephrine were deposited in the buccal and lingual mucosa, and the buccal and lingual periosteum. Anesthesia was per- formed according to the method described by Heller and Shankland1. After flap elevation, the implant placement site was prepared in the order of the second premolar, the first molar, and the canine. The patient experienced pain during the preparation and received additional injection into the gingiva. The length of the placed implants was all 11.5 mm which allowed more than 2 mm of space as safety margin between the implants and the IAN. After the surgery, the patient
Inferior alveolar nerve (IAN) is commonly anesthetized in dentoalveolar and implant surgery. IAN block anesthesia causes patients to lose sensation in mandible on one side, mandibular teeth on one side, ipsilateral tongue, and all but the buccal gingivae1. Total IAN block anesthesia assures patient comfort during surgical placement of mandibular implants, giving the dentist the opportunity to perform necessary surgical procedures in a pain-free environment. However, three major postoperative complications may occur with the use of block anesthesia of the IAN when placing mandibular implants: (1) prolonged mandibular anesthesia, during which time the patient may injure his or her tongue or lip in a variety of ways; (2) systemic toxicity from iatrogenic, intraarterial injection of local anesthetic solution; and, most importantly when placing mandibular implants, (3) injury to the inferior or mental nerves, unbeknown to the patient or doctor until after the effects of the block anesthesia have subsided1. As an alternative to the IAN block anesthesia for the placement of mandibular dental implants, mandibular infiltration anesthesia was discussed1,2. Etoz et al.2 concluded that supra- periosteal infiltration anesthesia is a safe and effective method for posterior mandibular implant surgery. Heller and Shankland1 considered that supraperiosteal infiltration might be useful for the patient’s being able to sense when the IAN is in
Case Reports
was instructed to note her discomfort and/or pain during the anesthesia and the implant placement on the visual analogue scale (VAS) of 0 to 10 cm, which was designed as 0 being no pain and 10 being the worst pain ever experienced.
To prevent the possible effect of the order of the anesthesia on the patient’s evaluation of the anesthe- sia method, block anesthesia and implant placement in the right side were performed after over 3 weeks of the surgery in the left side. One carpule of the same kind of lidocaine used in the right side was injected for IAN block. Another carpule was used for anesthesia of buccal nerve. After flap elevation, the implant place- ment site was prepared in the order of the first molar, the second molar, and the first premolar. The length of the placed implants was 11.5 mm for the first pre- molar, and 10 mm for the first molar and the second molar. The length of the first molar and the second
molar implants was shorter than that of the implants used in the left side because the distance between the alveolar crest and the IAN was shorter than that of the left side. The panoramic view after implant placement in both posterior regions is shown in the Fig. 1. The
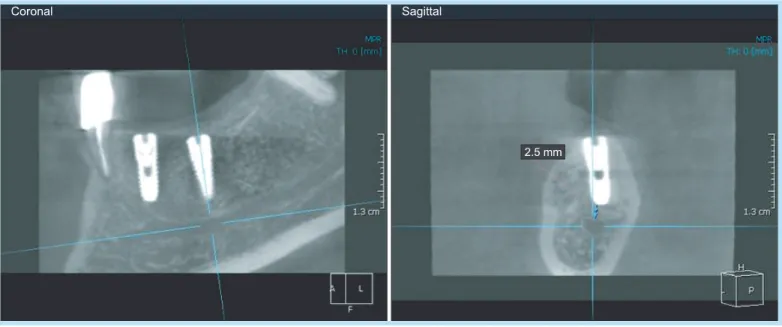
Fig. 2. Safety margin of the mandibular left second premolar.
Seong-June Park et al. : Block Anesthesia versus Infiltration Anesthesia of Inferior Alveolar Nerve When Placing Dental Implants in the Posterior Mandibular Region. Implantology 2014
Fig. 1. Panoramic radiography of the patient who underwent dental implant placement in both sides of the mandible. Infiltration anesthesia was used in the left side, while block anesthesia was used in the right side.
Seong-June Park et al. : Block Anesthesia versus Infiltration Anesthesia of Inferior Alveolar Nerve When Placing Dental Implants in the Posterior Mandibular Region.
Implantology 2014
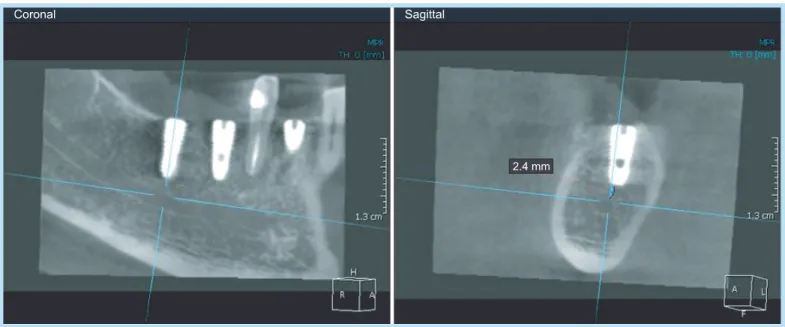
Fig. 3. Safety margin of the mandibular left first molar.
Seong-June Park et al. : Block Anesthesia versus Infiltration Anesthesia of Inferior Alveolar Nerve When Placing Dental Implants in the Posterior Mandibular Region. Implantology 2014
Fig. 4. Safety margin of the mandibular right first molar.
Seong-June Park et al. : Block Anesthesia versus Infiltration Anesthesia of Inferior Alveolar Nerve When Placing Dental Implants in the Posterior Mandibular Region. Implantology 2014
Case Reports
implant surgery after block anesthesia. Excluding the procedure of implant placement, she preferred infil- tration to block because she had felt more discomfort with the dull pain during block anesthesia although
the VAS values were the same. However, when includ- ing the procedure of implant placement, she preferred block anesthesia because there was no pain after anesthesia (Table 2).
III Discussion
Mandibular block anesthesia is normally a safe and rewarding method of pain control for interventions in Fig. 5. Safety margin of the mandibular right second molar.
Seong-June Park et al. : Block Anesthesia versus Infiltration Anesthesia of Inferior Alveolar Nerve When Placing Dental Implants in the Posterior Mandibular Region. Implantology 2014
Table 1. Visual analogue scale (cm) of discomfort and/or pain during anesthesia and implant placement
Procedure Anesthesia method Infiltration Block Anesthesia
Implant placement Left
Canine
Second premolar First molar Right
First premolar First molar Second molar
3
4 3 3
- - -
3
- - -
0 0 0
Seong-June Park et al. : Block Anesthesia versus Infiltration Anesthesia of Inferior Alveolar Nerve When Placing Dental Implants in the Posterior Mandibular Region.
Implantology 2014
Table 2. Preference for either anesthesia
Procedure Anesthesia method Infiltration Block Anesthesia only
Anesthesia+implant placement
O
O
Seong-June Park et al. : Block Anesthesia versus Infiltration Anesthesia of Inferior Alveolar Nerve When Placing Dental Implants in the Posterior Mandibular Region.
Implantology 2014
or permanent impairment of neurosensory function after mandibular block anesthesia with currently used local analgesics. According to Hillerup and Jensen3, mandibular block analgesia causes lingual nerve injury more frequently than IAN injury. All grades of loss of neurosensory and gustatory functions were found, and a range of persisting neurogenic malfunctions was reported. Subjective complaints and neurosensory function tests indicate that lingual nerve lesions are more incapacitating than IAN lesions. Besides the injury by the block anesthesia itself, there are other iatrogenic injuries of IAN4,5. Especially during dental implant surgery, IAN is prone to be damaged when the implant impinges the safety zone because the patient loses all sensory perception of the mandible under block anesthesia. Heller and Shankland1 and Etoz et al.2 support infiltration anesthesia partially because of this risk of block anesthesia. However, block anesthe- sia may be better than infiltration for patients’ comfort only if there is little possibility of damaging the IAN by implant. Furthermore, it can be avoided that the patients get injured by sudden movements due to the pain during preparation of the implant placement site.
The patient in this report felt pain after infiltration anesthesia in the left side during preparation of the implant placement site and needed more injections.
Actually, in the pre-operative planning using CBCT, the length of the implants to be placed in the left side was determined to allow enough safety margins and
cient infiltration anesthesia or other reasons.
Therefore the pain which the patient had to undergo in this case was unnecessary. As a result, the patient preferred block anesthesia to infiltration in the evalu- ation of the total procedure from anesthesia to implant placement.
With the rapid development of technology, CBCT has become available for the preoperative planning of oral implant placement6,7. CBCT scans help in the planning of oral implants; they enable measurement of the dis- tance between the alveolar crest and mandibular canal to avoid impingement of IAN, avoid perforation of the mandibular posterior lingual undercut, and assess the density and quality of bone, and help in planning of the oral implant in the maxilla with special attention to the nasopalatine canal and maxillary sinus6. Accordingly, infiltration is not necessarily better for avoiding damage to the IAN if safety is ensured in the CBCT images. However this does not mean that the safety margin in the CBCT images is the only deter- mining factor of the kind of anesthesia. The choice between block and infiltration can be also dependent on the surgeons’ preference and patients’ preference.
For the surgeons who do not have a CBCT system or feel uneasy about block anesthesia, it may be better to have patients endure a little discomfort during the procedure than to have them get nerve injury acciden- tally. Meanwhile some patients may be willing to undergo a little discomfort.
Case Reports
IV Conclusion
Anesthesia method when placing dental implants in the posterior mandibular region may be determined on a case-by-case basis depending on the anatomical evaluation of radiograph, surgeons’ preference, and patients’ preference. However, block anesthesia can be better than infiltration for patients’ comfort if the safety of IAN is guaranteed.
References
1. Heller AA, Shankland WE 2nd. Alternative to the inferior alveolar nerve block anesthesia when placing mandibular dental implants posterior to the mental foramen. J Oral Implantol. 2001; 27: 127-133.
2. Etoz OA, Er N, Demirbas AE. Is supraperiosteal infiltration anesthesia safe enough to prevent inferior alveolar nerve during posterior mandibular implant surgery? Med Oral Patol Oral Cir Bucal. 2011; 16:
e386-e389.
3. Hillerup S, Jensen R. Nerve injury caused by mandibular block analgesia. Int J Oral Maxillofac Surg. 2006; 35: 437-443.
4. Hillerup S. Iatrogenic injury to the inferior alveolar nerve: etiology, signs and symptoms, and observations on recovery. Int J Oral Maxillofac Surg. 2008; 37: 704-709.
5. Park YT, Kim SG, Moon SY. Indirect compressive injury to the inferior alveolar nerve caused by dental implant placement. J Oral Maxillofac Surg. 2012; 70: e258-e259.
6. Gupta J, Ali SP. Cone beam computed tomography in oral implants. Natl J Maxillofac Surg. 2013; 4: 2-6.
7. Guerrero ME, Jacobs R, Loubele M, et al. State-of-the-art on cone beam CT imaging for preoperative planning of implant placement. Clin Oral Investig. 2006; 10: 1-7.