Original Article
Received: Jan 14, 2017; Revised: Feb 3, 2017; Accepted: Feb 6, 2017; Published online Apr 30, 2017 Correspondence to: Tommaso Cai
Department of Urology, Santa Chiara Regional Hospital, Largo Medaglie d'Oro 9, Trento, Italy.
Tel: +39-0461-903306, Fax: +39-0461-903101, E-mail: [email protected]
The Clinical Efficacy of Pollen Extract and Vitamins on Chronic Prostatitis/Chronic Pelvic Pain Syndrome Is Linked to a Decrease in the Pro-Inflammatory Cytokine Interleukin-8
Tommaso Cai1, Paolo Verze2, Roberto La Rocca2, Alessandro Palmieri2, Daniele Tiscione1, Lorenzo Giuseppe Luciani1, Sandra Mazzoli3, Vincenzo Mirone2, Gianni Malossini1
1Department of Urology, Santa Chiara Regional Hospital, Trento, 2Department of Urology, University of Naples, Federico II, Naples,
3STD Centre, Santa Maria Annunziata Hospital, Florence, Italy
Purpose: We aim to evaluate the efficacy of pollen extract in association with vitamins in patients affected by chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) and to evaluate the level of the pro-inflammatory mediators interleukin (IL)-6, IL-8, and IL-10.
Materials and Methods: Patients diagnosed with CP/CPPS between January and December 2015 were enrolled in this study.
Participants were randomly assigned to receive oral capsules of pollen extract and vitamins (group A) or bromelain (group B) for 3 months. At the enrolment time and 3 months after enrolment, all patients completed questionnaires (the National Institutes of Health Chronic Prostatitis Symptom Index [NIH-CPSI] and the Short Form-36 and underwent urological examinations and microbiological evaluation. Levels of IL-6, IL-8, and IL-10 were evaluated in seminal plasma.
Results: Sixty-five male patients (mean age of 32.7±4.7 years) were analysed (group A, n=32; group B, n=33). At the follow-up examination, 24 of the 32 patients in group A showed a significant reduction in the NIH-CPSI total score compared with 8 of the 33 patients in the bromelain group (p<0.001). Moreover, the mean level of IL-8 was significantly lower in the pollen extract and vitamins group when compared with the bromelain group (298 pg/mL vs. 736 pg/mL, respectively; p< 0.001). In group A we found a statistically significant reduction in the levels of IL-8 between enrolment and the follow-up visit (878 pg/mL vs. 298 pg/mL, respectively; p<0.001).
Conclusions: Treatment with pollen extract and vitamins improved the quality of life in CP/CPPS patients by reducing the levels of pro-inflammatory IL-8.
Key Words: Interleukin-8; Pelvic pain; Pollen; Prostatitis
https://doi.org/10.5534/wjmh.2017.35.2.120
www.wjmh.org
INTRODUCTION
Chronic prostatitis (CP) is considered to be one of the most common illnesses in men aged over 50 years, with various clinical presentations [1]. According to the classi- fication scheme of the United States National Institutes of Health (NIH), class III CP/chronic pelvic pain syndrome (CP/CPPS) is the most frequently diagnosed category of this illness [2]. Symptoms such as pelvic pain, painful void- ing and ejaculation, and disturbed sexual function are common, often resulting in a significant impact on quality of life [3]. The therapeutic efficacy of current treatments for CP/CPPS has not been considered satisfactory, which in- troduces a number of aspects for consideration and analy- sis [4]. The use of antibiotics remains controversial, espe- cially considering the fact that no bacteria have ever been isolated from the urogenital samples of CP/CPPS patients [5]. However, even if anti-inflammatory medications, can decrease pain, their high prevalence of drug-related ad- verse effects mean that these should be taken for a limited period of time only. Therefore, the standard treatment for CP/CPPS has not yet been definitively established. Given this situation, phytotherapeutics may present a viable op- tion; however, few compounds have been subjected to scientific scrutiny and prospective controlled clinical trials [6,7]. Over the past few years, there has been increased in- terest in the use of flower pollen extract for the manage- ment of CP/CPPS [8]. Several studies have shown that flower pollen extract preparations may contribute to a last- ing and marked symptom reduction in young men with CP/CPPS, with improvement in semen quality and a sig- nificant decrease in the National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI) score [8-11]. Several studies have found that patients with CP/CPPS showed higher levels of pro-inflammatory cyto- kines, such as interleukin (IL)-1b, IL-6, tumour necrosis factor a, and IL-8 [12,13] compared to controls. Moreover, IL-8 could be considered a useful biomarker in the man- agement of CP/CPPS and could potentially be applicable to disease diagnosis, prognosis, and treatment [12].
Herein, we aim to evaluate the efficacy of pollen extract in association with vitamins (Deprox 500Ⓡ; IDI Integratori Dietetici Italiani S.r.l, Sicily, Italy) in patients affected by CP/CPPS and to perform a detailed evaluation of pro-in-
flammatory mediators IL-6, IL-8, IL-10 in order to establish the mechanism of action for this treatment.
MATERIALS AND METHODS
1. Study design
This study was a prospective, randomized, unblinded, controlled phase III clinical trial aimed at evaluating the ef- ficacy of pollen extract and vitamins in patients affected by CP/CPPS and their levels of pro-inflammatory mediators.
All consecutive patients with a clinical and instrumental diagnosis of inflammatory CP/CPPS (NIH class IIIa-in- flammatory CP/CPPS) attending the same urologic centre between January and December 2015 were screened for enrolment in the study. The treatment group received pol- len extract with vitamins (Deprox 500Ⓡ), while the control group received bromelain. The choice of bromelain as control group treatment was due to the lack of a gold- standard treatment for CP/CPPS [5,7]. Bromelain was also chosen primarily for the fact that it is a phytotherapeutic compound with an anti-inflammatory effect, considered safe as a long-term therapy, with high patient compliance [14].
2. Outcome measures
The main outcome measures of our study were as fol- lows: an improvement in quality of life, defined as an im- provement in the NIH-CPSI score (i.e., a reduction of the NIH-CPSI total score by ≥25%) and a decrease in pro-in- flammatory mediators (i.e., a reduction of at least 65%
from the baseline) by the end of the complete study period.
3. Inclusion and exclusion criteria
The inclusion criteria were the presence of pelvic pain symptoms for at least 3 months during the 6 months before study enrolment in accordance with the European Asso- ciation of Urology guidelines, a score in the pain domain of the NIH-CPSI of >4 and a negative result for the Meares-Stamey 4-glass test [11,15,16]. We excluded all patients with the following characteristics: subjects <18 and >65 years of age affected by major concomitant dis- eases with known anatomical abnormalities of the urinary tract or with evidence of other urological diseases with re-
sidual urine volume >50 mL resulting from bladder outlet obstruction, subjects with a reported allergy to pollen ex- tract who had recently (within <4 weeks) undergone oral or parental treatment or who were currently using prophy- lactic antibiotic drugs, and all patients who tested positive for Chlamydia trachomatis, Ureaplasma urealyticum, Neisseria gonorrhoeae, herpesviruses (HSV 1/2), and hu- man papillomavirus (HPV).
4. Study schedule
Upon arrival at our centre, all eligible individuals pro- vided their written informed consent, completed baseline questionnaires, underwent a urological examination with the Meares-Stamey test, and provided a seminal sample on site [15,16]. All seminal plasma samples were used in the pro-inflammatory cytokine evaluation. All patients who met the inclusion criteria were randomized to either the treatment or control group by using a computer-generated allocation sequence. All patients were assigned to 1 of the 2 groups (group A: pollen extract in association with vita- mins; and group B: bromelain) according to a 1:1 ran- domization. Those patients assigned to group A ingested a daily oral administration of 2 tablets of pollen extract and vitamins in a single dose in the evening. All patients as- signed to group B underwent daily oral administration of 2 tablets of 40 mg of bromelain in a single daily dose in the evening. Neither the physicians nor the patients were blinded to the treatment type. All patients were contacted by telephone on day 30 of the therapy to ensure that they were correctly administering the drug, in order to ensure
uniform treatment interval and dosage. A follow-up visit was scheduled at 3 months from the start of therapy, with urological and microbiological examinations, question- naire collection, and pro-inflammatory cytokines evalua- tion. Fig. 1 shows the study schedule.
5. Composition and characterization of the extracts used
1) Pollen extract in association with vitamins (Deprox 500Ⓡ)
Each administration contained 1 g of pollen extract (500 mg per tablet, GRAMINEX; IDI Integratori Dietetici Italiani S.r.l) and vitamins B1, B2, B6, B9, B12, and PP, as described in the manufacturer’s instructions.
2) Bromelain
All patients in the control group received 80 mg of bro- melain per day. Bromelain is a crude, aqueous extract ob- tained from both the stem and fruit of the pineapple plant, which contains a number of proteolytic enzymes and has shown potentially beneficial effects due to its anti-in- flammatory and analgesic properties [17].
6. Questionnaires and urological examinations The validated Italian versions of the NIH-CPSI [18] and Short Form-36 (SF-36) questionnaires were self-adminis- tered to all patients [19].
www.wjmh.org Fig. 2. The flowchart for the study according to the Consolidated Stan- dards of Reporting Trials 2010 flow diagram.
7. Microbiological considerations, sample collection, and laboratory procedures
All samples from the Meares-Stamey test and seminal plasma were collected at the time of the urological visit and immediately taken to the laboratory under refriger- ated conditions, analysed for cultures, and aliquoted for DNA extraction and polymerase chain reaction for C. tra- chomatis, U. urealyticum, N. gonorrhoeae, HSV 1/2 and HPV detection [20]. All microbiological evaluations and DNA extraction and purification were carried out in ac- cordance with the methods described by Mazzoli et al [20]. In addition, natural human-produced IL-6, IL-8, and IL-10 concentrations were identified in the seminal sam- ples of all patients and controls with the solid-phase en- zyme-linked immunosorbent assay Quantikine IL-6, IL-8, and IL-10 Immunoassay (R&D Systems, Minneapolis, MN, USA) [20]. All samples were tested in duplicate by using independent analysis in accordance with the manu- facturer’s recommendations and in order to avoid errors.
The medium minimal detectable doses of the IL-6, IL-8,
and IL-10 assays were 0.70 pg/mL, 3.5 pg/mL, and 3.9 pg/mL, respectively [20].
8. Ethical and statistical considerations
The study was conducted in line with Good Clinical Practice guidelines, in compliance with the ethical princi- ples published in the latest version of the Declaration of Helsinki. Written informed consent was obtained from all patients prior to treatment. Furthermore, this study was conducted in line with the Consolidated Standards of Reporting Trials statement (URO-TN-2015). The homoge- neity of the 2 groups at the baseline evaluation was carried out by using the Student t-test and Mann-Whitney U-test for continuous variables and by the chi-square test for cat- egorical variables. General characteristics of the study par- ticipants were expressed using descriptive statistics (means, standard deviations, or ranges). Randomization based on a single sequence of random assignments (simple randomization) was performed using a pseu- do-random number generator program (Research Randomizer ver. 4.0; Social Psychology Network,
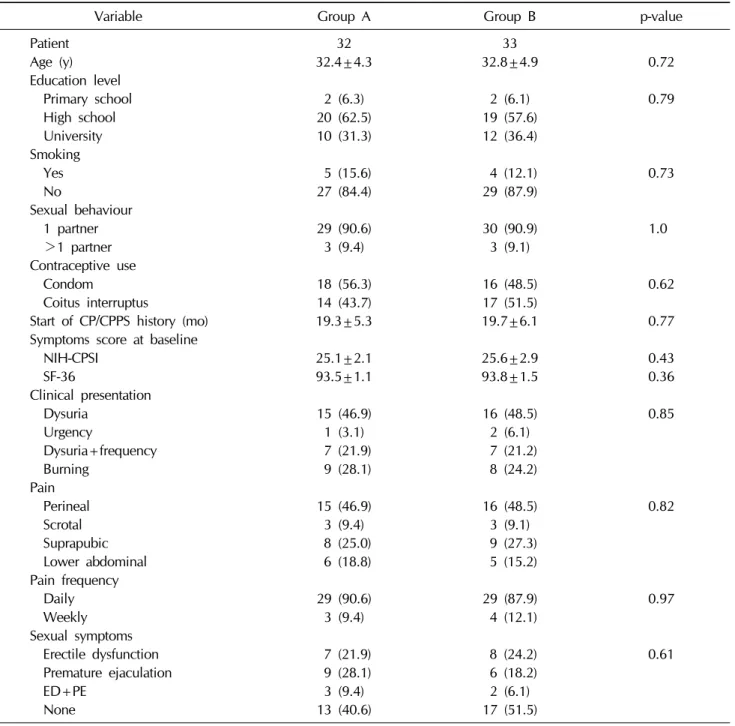
Table 1. Demographic and clinical data of the patients at the time of enrolment
Variable Group A Group B p-value
Patient 32 33
Age (y) 32.4±4.3 32.8±4.9 0.72
Education level
Primary school 2 (6.3) 2 (6.1) 0.79
High school 20 (62.5) 19 (57.6)
University 10 (31.3) 12 (36.4)
Smoking
Yes 5 (15.6) 4 (12.1) 0.73
No 27 (84.4) 29 (87.9)
Sexual behaviour
1 partner 29 (90.6) 30 (90.9) 1.0
>1 partner 3 (9.4) 3 (9.1)
Contraceptive use
Condom 18 (56.3) 16 (48.5) 0.62
Coitus interruptus 14 (43.7) 17 (51.5)
Start of CP/CPPS history (mo) 19.3±5.3 19.7±6.1 0.77
Symptoms score at baseline
NIH-CPSI 25.1±2.1 25.6±2.9 0.43
SF-36 93.5±1.1 93.8±1.5 0.36
Clinical presentation
Dysuria 15 (46.9) 16 (48.5) 0.85
Urgency 1 (3.1) 2 (6.1)
Dysuria+frequency 7 (21.9) 7 (21.2)
Burning 9 (28.1) 8 (24.2)
Pain
Perineal 15 (46.9) 16 (48.5) 0.82
Scrotal 3 (9.4) 3 (9.1)
Suprapubic 8 (25.0) 9 (27.3)
Lower abdominal 6 (18.8) 5 (15.2)
Pain frequency
Daily 29 (90.6) 29 (87.9) 0.97
Weekly 3 (9.4) 4 (12.1)
Sexual symptoms
Erectile dysfunction 7 (21.9) 8 (24.2) 0.61
Premature ejaculation 9 (28.1) 6 (18.2)
ED+PE 3 (9.4) 2 (6.1)
None 13 (40.6) 17 (51.5)
Values are presented as number only, mean±standard deviation, or number (%). The sum of the percentages does not equal 100% because of rounding.
Group A: received pollen extract with vitamins (Deprox 500Ⓡ); treatment group, Group B: received bromelain; control group, CP/CPPS: chronic prostatitis/chronic pelvic pain syndrome, NIH-CPSI: National Institutes of Health Chronic Prostatitis Wesleyan University, Middletown, CT, USA). ANOVA
was used for comparing the means. The Bonferroni adjust- ment test was also used at the second stage of the ANOVA.
The differences between the groups regarding the NIH-CPSI results and mean concentration of pro-in-
flammatory cytokines were obtained using an ANOVA test. The calculation of the sample size needed for enrol- ment was based on the first outcome measure (improvement of quality of life), due to the fact that we had no data on the effects of pollen extract in association with
www.wjmh.org Table 2. Questionnaire results at the 3-month follow-up visit
Variable Group A Group B p-value
NIH-CPSI
Before treatment 25.1±2.1 25.6±2.9 0.43
After treatment 11.7±3.2 22.5±3.7 <0.001
p-value <0.001 0.0003
NIH-CPSI pain domain
Before treatment 11.3±2.1 10.7±2.5 0.29
After treatment 6.7±1.9 8.1±2.3 0.009
p-value <0.001 <0.001
Reduction in the NIH-CPSI pain domain −4.8±0.3 −2.1±0.7 <0.001
SF-36
Before treatment 93.5±1.1 93.8±1.5 0.36
After treatment 98.6±2.1 94.9±2.9 <0.001
p-value <0.001 0.08
Values are presented as mean±standard deviation.
Group A: received pollen extract with vitamins (Deprox 500Ⓡ); treatment group, Group B: received bromelain; control group, NIH-CPSI: National Institutes of Health Chronic Prostatitis Symptom Index, SF-36: Short Form-36.
vitamins on pro-inflammatory cytokines. In this sense and in line with the literature results, the required sample size was calculated under the following conditions: difference between the groups, 35% of patients who reach a reduc- tion in 25% of the NIH-CPSI total score; α error level=
0.05, 2-sided; statistical power, 80%; and anticipated ef- fect size, Cohen d=0.5. Our calculation indicated that 32 individuals would be needed in each of 2 groups. Statistical significance was achieved when p<0.05. All reported p-values were 2-sided. Statistical analyses were performed using SPSS software ver. 11.0 (SPSS Inc., Chicago, IL, USA) for Macintosh (Apple, Cupertino, CA, USA).
RESULTS
From a group of 121 patients attending our centre dur- ing the enrolment period, 70 met the inclusion criteria and were randomly allocated as follows: 36 to group A and 34 to group B. Five patients were excluded and a final total of 65 patients were analysed (Fig. 2). No statistically sig- nificant differences between the groups were identified.
All clinical and laboratory data at enrolment are described in Table 1.
1. Clinical results at follow-up evaluation
At the end of the treatment period, 24 of 32 patients
(75.0%) in the pollen extract and vitamins group reported an improvement in quality of life, as did 8 of 33 patients (24.2%) in the bromelain group (p<0.001). The SF-36 questionnaires confirmed these results (mean SF-36 value in the treatment group: 98.6±2.1; mean SF-36 value in the control group: 94.9±2.9; p<0.001). All questionnaire re- sults at 3 months after treatment are listed in Table 2. The greater improvement in the treatment group compared with the control group was statistically significant (treat- ment difference in the NIH-CPSI pain domain: −4.8±0.3 vs. −2.1±0.7; p<0.001).
2. Laboratory and microbiological results at follow-up evaluation
The mean levels of pro-inflammatory cytokines at the follow-up evaluation are detailed in Table 3. No statisti- cally significant differences were identified between the 2 groups in terms of IL-6 and IL-10 levels (p=0.81 and p=
0.41, respectively). The mean post-treatment level of IL-8 was significantly lower in group A compared with group B (IL-8, 298 pg/mL vs. IL-8, 736 pg/mL; p<0.001). In group A we found a statistically significant reduction of IL-8 lev- els between the enrolment period and the follow-up visit (IL-8, 878 pg/mL vs. IL-8, 298 pg/mL; p<0.001) (Table 3).
A good correlation between the reduction of IL-8 (at least 65% from the pre-treatment value) and quality of life im-
Table 3. Pro-inflammatory cytokine evaluation at enrolment and at the 3-month follow-up visit
Variable Group A Group B p-value
IL-6 (pg/mL)
Before treatment 38,126 (19,000∼44,800) 39,060 (19,000∼44,800) 0.43
After treatment 34,040 (19,000∼44,800) 35,146 (19,000∼44,800) 0.81
p-value 0.78 0.52
IL-8 (pg/mL)
Before treatment 878 (346∼12,000) 912 (418∼12,000) 0.09
After treatment 298 (100∼3,460) 736 (346∼12,000) <0.001
p-value <0.001 0.07
IL-10 (pg/mL)
Before treatment 64 (34∼96) 66 (34∼96) 0.38
After treatment 48 (34∼96) 52 (34∼96) 0.41
p-value 0.56 0.79
Values are presented as median (range).
Group A: received pollen extract with vitamins; treatment group, Group B: received bromelain; control group, IL: interleukin.
provement (receiver operating characteristic, area under curve=0.83; p=0.001) was found. All patients tested neg- ative at the Meares-Stamey evaluation.
3. Adverse effects
One patient out of 32 patients (3.1%) in group A and 2 of 33 patients (6.1%) in group B had mild adverse effects (nausea).
DISCUSSION
1. Major finding
Herein, we have demonstrated the clinical efficacy of pollen extract in association with vitamins for managing patients affected by CP/CPPS, and the results of our study revealed a relationship between the reduction of IL-8 and clinical efficacy. Another important aspect that came to light is that that the reduction of IL-8 (65%) could be con- sidered a good marker for the response to treatment for CP/CPPS and improvement of patient quality of life.
2. Results in comparison with other studies The efficacy of pollen extract in the treatment of patients affected by CP/CPPS has been demonstrated by several clinical studies [8-11,16,21-24]. All authors agree that pol- len extracts significantly improved total symptoms, pain, and quality of life in patients with inflammatory CP/CPPS
Cai et al [9] in a non-randomized clinical study reported a clinical response rate of 90%, demonstrating that pollen extract in association with vitamins significantly improved total symptoms, pain, and quality of life in patients with non-inflammatory CP/CPPS without severe side effects.
Moreover, 3 studies by Japanese researchers demon- strated a high clinical response rate to pollen extract treat- ments in patients with both class IIIa and class IIIb CP/CPPS [24-26]. In a randomized control trial involving 139 patients affected by inflammatory CP/CPPS and treat- ed for 12 weeks with flower pollen extract, Wagenlehner et al [11] demonstrated a clinical response rate of 70.6%.
In addition, in a cohort of patients randomized to pollen extract or ibuprofen treatment groups, Cai et al [16] re- ported a response rate of 75.6% in the flower pollen ex- tract group with a low prevalence of adverse effects. All authors hypothesized that the clinical effect of pollen ex- tract was due to an anti-inflammatory anti-proliferative ef- fect on the basis of pre-clinical studies [21]. Up to the pres- ent, no clinical study has yet demonstrated the effect of pollen extract on pro-inflammatory cytokines. The only available data come from an animal experiment on a dose- dependent anti-inflammatory action of pollen extract in comparison with aspirin in nonbacterial prostatitis in rats.
The study findings showed an approximately 10× greater decrease in the levels of IL-1b, IL-6, and tumour necrosis factor in the pollen extract treatment group [21]. Herein,
www.wjmh.org
fect of pollen extract in association with vitamins is asso- ciated with a reduction in IL-8 levels. A few years ago, Penna et al [12] demonstrated that, among all the cyto- kines and chemokines analysed, IL-8 appears to be the most reliable and predictive surrogate marker for diagnos- ing prostate inflammatory conditions, such as CP/CPPS and benign prostatic hyperplasia. This aspect is very im- portant, because in CP/CPPS patients no biological or mo- lecular markers exist that may be used to evaluate the re- sponse to treatment [21]. In fact, Wagenlehner et al [11]
found a decrease of leukocytes in post-prostate massage urine samples in both patients and controls; however, they did not find a significant difference between the 2 groups in terms of leukocyte numbers and, for this reason, they concluded that leukocytes cannot be correlated with clin- ical success [11]. This aspect supports the hypothesis that the presence of inflammatory cells in the post-prostate massage urine sample is not a laboratory characteristic ad- equately able to predict the response to the treatment. In this sense, our study highlights the feasible role of IL-8 evaluation in predicting the response to treatment in CP/CPPS patients. However, no statistically significant dif- ference in terms of IL-6 or IL-10 levels was observed in our patient population. A few experiments have demonstrated the possible diagnostic role of IL-6 and/or IL-10 evaluation in patients affected by asymptomatic prostatitis (class IV) or benign prostate hyperplasia [27,28]. In particular, Miller et al [29] found that IL-10 levels correlated directly to measures of life interference and pain severity, thus highlighting their diagnostic role. However, no studies have ever evaluated changes to levels of IL-6 and/or IL-10 during therapy in CP/CPPS patients. As far as we are aware, ours is the first study to evaluate the changes in lev- els of IL-6 and IL-10 during treatment. On the basis of these considerations, the efficacy of pollen extract in association with vitamins in CP/CPPS patients is probably due to the anti-inflammatory effects of pollen extract and the neuro- protective role of B vitamins. The superiority of pollen ex- tract in association with vitamins in comparison with bro- melain is probably due to the additional role of B vitamins, because bromelain also shows an anti-inflammatory effect [30]. However, the neuroprotective role of B vitamins should be confirmed by future studies.
3. Strengths and limitations of the present study The present paper reveals important factors that should be taken into account in CP/CPPS treatment: the evalua- tion of the pro-inflammatory cytokines level and the corre- lation between these and clinical results. However, some limitations of our study also need to be taken into account, including the small number of enrolled patients, the short follow-up period, the selected patient population, and the non-blinded nature of the study.
CONCLUSIONS
Treatment with pollen extract and vitamins improved the quality of life of patients affected by CP/CPPS, and its clinical efficacy was associated with a decrease in pro-in- flammatory cytokine IL-8. Moreover, the reduction in IL-8 (65%) could be considered a good marker for response to the treatment.
ACKNOWLEDGEMENTS
We are grateful to Juliet Ippolito for manuscript lan- guage revision.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
1. Collins MM, Stafford RS, O'Leary MP, Barry MJ. How com- mon is prostatitis? A national survey of physician visits. J Urol 1998;159:1224-8.
2. Schaeffer AJ. Classification (traditional and National Insti- tutes of Health) and demographics of prostatitis. Urology 2002;60(6 Suppl):5-6; discussion 6-7.
3. Nickel JC. Role of alpha1-blockers in chronic prostatitis syndromes. BJU Int 2008;101 Suppl 3:11-6.
4. Tuğcu V, Taşçi AI, Fazlioğlu A, Gürbüz G, Ozbek E, Sahin S, et al. A placebo-controlled comparison of the efficiency of triple- and monotherapy in category III B chronic pelvic pain syndrome (CPPS). Eur Urol 2007;51:1113-7; discussion 1118.
5. Nickel JC, Downey J, Clark J, Casey RW, Pommerville PJ,
Barkin J, et al. Levofloxacin for chronic prostatitis/chronic pelvic pain syndrome in men: a randomized placebo-con- trolled multicenter trial. Urology 2003;62:614-7.
6. Herati AS, Moldwin RM. Alternative therapies in the man- agement of chronic prostatitis/chronic pelvic pain synd- rome. World J Urol 2013;31:761-6.
7. Shoskes DA, Zeitlin SI, Shahed A, Rajfer J. Quercetin in men with category III chronic prostatitis: a preliminary pro- spective, double-blind, placebo-controlled trial. Urology 1999;
54:960-3.
8. Rugendorff EW, Weidner W, Ebeling L, Buck AC. Results of treatment with pollen extract (Cernilton N) in chronic pros- tatitis and prostatodynia. Br J Urol 1993;71:433-8.
9. Cai T, Luciani LG, Caola I, Mondaini N, Malossini G, Lanzafame P, et al. Effects of pollen extract in association with vitamins (DEPROX 500Ⓡ) for pain relief in patients af- fected by chronic prostatitis/chronic pelvic pain syndrome:
results from a pilot study. Urologia 2013;80 Suppl 22:5-10.
10. Kamijo T, Sato S, Kitamura T. Effect of cernitin pollen-ex- tract on experimental nonbacterial prostatitis in rats. Prostate 2001;49:122-31.
11. Wagenlehner FM, Schneider H, Ludwig M, Schnitker J, Brähler E, Weidner W. A pollen extract (Cernilton) in pa- tients with inflammatory chronic prostatitis-chronic pelvic pain syndrome: a multicentre, randomised, prospective, double-blind, placebo-controlled phase 3 study. Eur Urol 2009;56:544-51.
12. Penna G, Mondaini N, Amuchastegui S, Degli Innocenti S, Carini M, Giubilei G, et al. Seminal plasma cytokines and chemokines in prostate inflammation: interleukin 8 as a pre- dictive biomarker in chronic prostatitis/chronic pelvic pain syndrome and benign prostatic hyperplasia. Eur Urol 2007;
51:524-33.
13. Khadra A, Fletcher P, Luzzi G, Shattock R, Hay P. Interleukin-8 levels in seminal plasma in chronic prostatitis/chronic pelvic pain syndrome and nonspecific urethritis. BJU Int 2006;97:
1043-6.
14. Taussig SJ, Batkin S. Bromelain, the enzyme complex of pineapple (Ananas comosus) and its clinical application. An update. J Ethnopharmacol 1988;22:191-203.
15. European Association of Urology Guidelines [Internet].
[cited 2016 Aug]. Available from: http://uroweb.org/wp-con- tent/uploads/19-Urological-infections_LR2.pdf.
16. Cai T, Wagenlehner FM, Luciani LG, Tiscione D, Malossini G, Verze P, et al. Pollen extract in association with vitamins provides early pain relief in patients affected by chronic prostatitis/chronic pelvic pain syndrome. Exp Ther Med 2014;8:1032-8.
17. Cooreman WM, Scharpé S, Demeester J, Lauwers A.
Bromelain, biochemical and pharmacological properties.
Pharm Acta Helv 1976;51:73-97.
18. Giubilei G, Mondaini N, Crisci A, Raugei A, Lombardi G, Travaglini F, et al. The Italian version of the National Insti-
tutes of Health Chronic Prostatitis Symptom Index. Eur Urol 2005;47:805-11.
19. Nickel JC, Downey J, Hunter D, Clark J. Prevalence of pros- tatitis-like symptoms in a population based study using the National Institutes of Health chronic prostatitis symptom index. J Urol 2001;165:842-5.
20. Mazzoli S, Cai T, Rupealta V, Gavazzi A, Castricchi Pagliai R, Mondaini N, et al. Interleukin 8 and anti-chlamydia tra- chomatis mucosal IgA as urogenital immunologic markers in patients with C. trachomatis prostatic infection. Eur Urol 2007;51:1385-93.
21. Wagenlehner FM, Bschleipfer T, Pilatz A, Weidner W.
Pollen extract for chronic prostatitis-chronic pelvic pain synd- rome. Urol Clin North Am 2011;38:285-92.
22. Elist J. Effects of pollen extract preparation Prostat/Poltit on lower urinary tract symptoms in patients with chronic non- bacterial prostatitis/chronic pelvic pain syndrome: a ran- domized, double-blind, placebo-controlled study. Urology 2006;67:60-3.
23. Iwamura H, Koie T, Soma O, Matsumoto T, Imai A, Hatakeyama S, et al. Eviprostat has an identical effect com- pared to pollen extract (Cernilton) in patients with chronic prostatitis/chronic pelvic pain syndrome: a randomized, prospective study. BMC Urol 2015;15:120.
24. Li NC, Na YQ, Guo HQ. Clinical study with Prostat (Poltit) for treatment for chronic nonbacterial prostatitis. Chin J Urol 2003;24:635-7.
25. Jodai A, Maruta N, Shimomae E, Sakuragi T, Shindo K, Saito Y. A long-term therapeutic experience with Cernilton in chronic prostatitis. Hinyokika Kiyo 1988;34:561-8.
26. Monden K, Tsugawa M, Ninomiya Y, Ando E, Kumon H. A Japanese version of the National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI, Okayama version) and the clinical evaluation of cernitin pollen extract for chronic non-bacterial prostatitis. Nihon Hinyokika Gakkai Zasshi 2002;93:539-47.
27. Suzuki T, Kurokawa K, Mashimo T, Takezawa Y, Kobayashi D, Kawashima K, et al. Clinical effect of Cernilton in chron- ic prostatitis. Hinyokika Kiyo 1992;38:489-94.
28. Korrovits P, Ausmees K, Mändar R, Punab M. Seminal inter- leukin-6 and serum prostate-specific antigen as possible pre- dictive biomarkers in asymptomatic inflammatory prosta- titis. Urology 2011;78:442-6.
29. Miller LJ, Fischer KA, Goralnick SJ, Litt M, Burleson JA, Albertsen P, et al. Interleukin-10 levels in seminal plasma:
implications for chronic prostatitis-chronic pelvic pain synd- rome. J Urol 2002;167:753-6.
30. Cai T, Tiscione D, Gallelli L, Verze P, Palmieri A, Mirone V, et al. Serenoa repens associated with selenium and lyco- pene extract and bromelain and methylsulfonylmethane ex- tract are able to improve the efficacy of levofloxacin in chronic bacterial prostatitis patients. Arch Ital Urol Androl 2016;88:177-82.