관련 문서
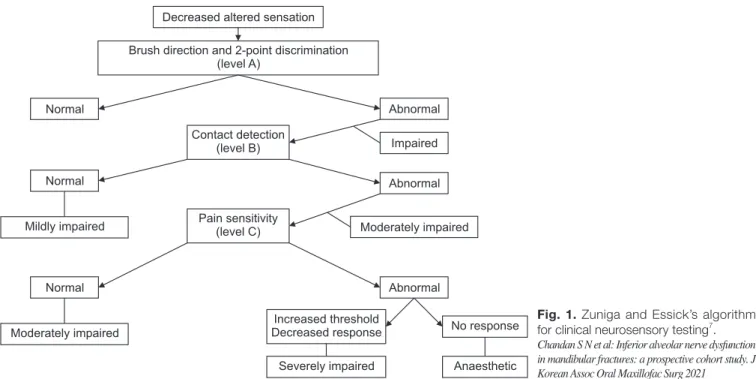
The purpose of this study was to analyze the impaction pattern of the impacted mandibular third molar and the relationship with the inferior alveolar nerve
3,4 Therefore, to date, studies have been conducted to examine the absorbable fixation plate manufactured using polymer and a fixation screw that can
The purpose of this study was to evaluate the curvature of Vertucci's type II mesial canals of mandibular molar using new method; The radius and angle
mandibular P-18 inncisor from Nfic-deficient mice (×3,000)... In this study, histological and immunohistochemical studies were carried out to investigate
The aim of this study was to develop a training program for swallowing and to test its effect on swallowing capacity and nutritional status in stroke
Abstract: This study aimed to review the oral hygiene status, oral care guidelines, and outcomes of oral care in intensive care unit (ICU) patients from a dental
UK Prospective Diabetes Study Group: Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complcaitons in patients with
A randomized prospective trial of three different 항생제 s of treatment of peritonitis in patients on continuous ambulatory peritoneal dialysis.. Ciprofloxacin and cefazolin as