124 ISSN 0377-9556 (PRINT) ISSN 2383-9457 (ONLINE)
약학회지 제 61 권 제 2 호 124~134 (2017) Yakhak Hoeji Vol. 61, No. 2
DOI 10.17480/psk.2017.61.2.124
Efficacy and Safety of Bedaquiline and Delamanid in the Treatment of Tuberculosis: a Focus on Multidrug-resistant Tuberculosis
Young-Mo Yang and Eun Joo Choi
#Department of Pharmacy, College of Pharmacy, Chosun University, Gwangju, Korea (Received March 17, 2017; Revised April 5, 2017; Accepted April 6, 2017)
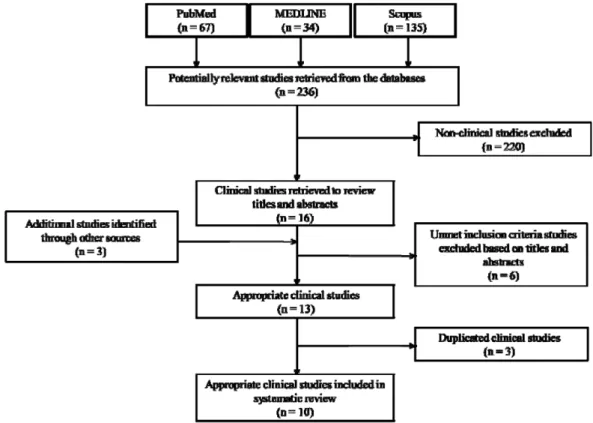
Abstract — The emergence of multi-drug resistant tuberculosis (MDR-TB) poses a major difficulty in controlling TB worldwide. More potent TB drugs, higher cost, and longer duration of treatment are necessary for MDR-TB compared with drug-sensitive TB. However, currently available TB drugs have been used for more than 40 years. Therefore, a novel anti- TB drug is required for the treatment of MDR-TB. This study was aimed at assessing the efficacy and safety of bedaquiline and delamanid and determining the therapeutic validity of them in controlling MDR-TB. A literature search of original stud- ies published in PubMed, MEDLINE, and Scopus until August 2015 was conducted using the terms ‘bedaquiline OR dela- manid’ AND ‘efficacy OR safety’ AND ‘tuberculosis’ to identify the clinical trials regarding bedaquiline or delamanid in TB.
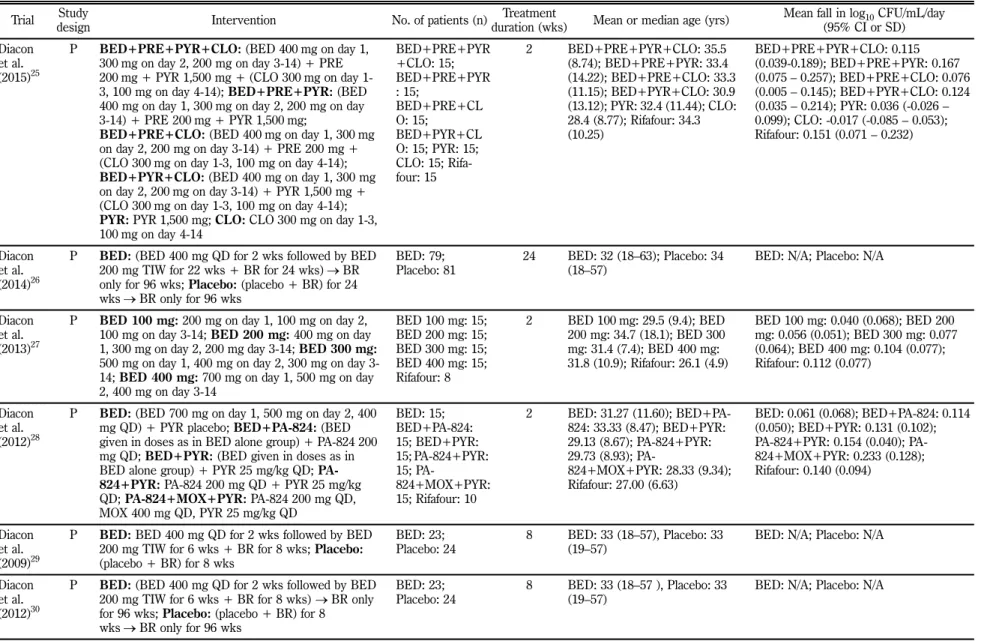
Six and four clinical studies regarding bedaquiline and delamanid, respectively, were examined in this review. The treatment durations of bedaquiline and delamanid in the selected studies were from 2 weeks to 32 weeks. The higher falls in log
10colony forming units (CFU)/mL during the treatment period were observed in the regimens including bedaquiline than in the standard anti-TB regimen. The median time to sputum-culture conversion (TTC) of the bedaquiline group was shorter than that of the placebo group. The sputum-culture conversion rate of the delamanid group was higher than that of the pla- cebo group. In the included studies, serious adverse effects were not reported due to bedaquiline or delamanid. However, their uses were more highly associated with potential QT-interval prolongation. The clinical trials suggest that the uses of bedaquiline or delamanid with other anti-TB medications were at least efficacious and safe in the treatment of MDR-TB at this point.
Keywords multidrug-resistant tuberculosis, MDR-TB, bedaquiline, delamanid, efficacy, safety
With 9 million cases and 1.5 million deaths in 2013, tubercu- losis (TB), caused by infection with Mycobacterium tuberculo- sis, is second only to the human immunodeficiency virus (HIV) in its lethal impact on humans.
1)The emergence of multidrug- resistant TB (MDR-TB), defined as TB with resistance to at least two first-line anti-TB drugs isoniazid and rifampicin, poses a major difficulty in controlling TB worldwide.
2)In 2013, approximately 480,000 new cases of MDR-TB were reported, and nearly 210,000 MDR-TB patients died.
1)However, only about 97,000 MDR-TB patients received treatment in 2013.
1)Although MDR-TB incidence rate remained stable worldwide from 2008 to 2013, serious MDR-TB epidemics threaten prog- ress in some countries, including India and China.
1)Prolonged administration of a combination of TB drugs is required to cure TB. More potent and more expensive TB drugs and longer treatment duration are necessary to cure MDR-TB compared to drug-sensitive TB.
3)Previous studies reported that the success rate of MDR-TB treatment was nearly 65% world- wide.
4-7)Studies conducted in Korea demonstrated that the treatment success rate varied from 37.1% to 66.0%.
8-14)How- ever, currently available TB drugs have been used for over 40 years.
15)Therefore, novel anti-TB drugs are required for MDR- TB treatment and should have the following characteristics: new mechanism of action, good efficacy and safety, and a suitable pharmacokinetic profile and bioavailability.
16)In December 2012, the US Food and Drug Administration (FDA) approved bedaquiline, belonging to a new class of TB
#