- 109 -
KISEP Original Articles J Rhinol 7((((2)))), 2000
Orbital Complications of Rhinosinusitis: : : : Characteristics in Pediatric Patients*
Yong-Jae Kim, M.D.
1and Yang-Gi Min, M.D.
2ABSTRACT
To evaluate the differences in clinical features of rhinosinogenic orbital complications between the pediatric and adult groups, a multicenter survey was made on 79 cases of rhinogenic orbital complications (from January 1985 through October 1999).
The patients ranged in age between 8 months and 79 years with a mean of 28 years. Thirty-five patients were under 15 years of age (pediatric group), and 44 patients were over 15 years of age (adult group). Twenty-three of 35 pediatric patients (65.7%) had postseptal orbital inflammation, whereas 30 of 44 adult patients (68.2%) had postseptal orbital inflammation. The pediatric group had shorter symptom duration than the adult group. Pediatric OCRS also developed as various forms-inflammatory edema, orbital cellulitis, orbital abscess and subperiosteal abscess. Sixteen of 35 pediatric patients (45.7%) underwent surgical interventions. The cure rate by surgical interventions in the pediatric group (14/16, 87.4%) was higher than that in the adult group (21/26, 80.8%). The cure rate by medical treatment in the pediatric group (18/19, 94.7%) was also higher than that in the adult group (11/16, 68.7%).
KEY WORDS:Orbital complication·Pediatric rhinosinusitis.
INTRODUCTION
More than 60% of orbital inflammatory processes originate from the acutely inflammed paranasal sinu- ses.1) Since endoscopic sinus surgery (ESS) became one of the popular surgical tools along with the deve- lopment of computerized tomography (CT), a wider variety of nasal diseases has been indicated for surgical treatment. Furthermore with the advent of the markedly enhanced resolution power and magnification of rece- ntly developed surgical endoscopes, the deep operative fields with surgical risks are now a commonplace for
surgery.2)3) Enhanced endoscopic surgical technique can bring about more surgical risks. On the other hand, it can be a helpful measure to manage the rhinogenic orbital complications.
The most commonly used classification of orbital complications is;I. inflammatory (preseptal) edema, II.
orbital (postseptal) cellulitis, III. subperiosteal abscess (SPA), IV. orbital abscess, and V. cavernous sinus th- rombosis (CST).4)
To investigate the differences in clinical features of orbital complications accompanying rhinosinusitis bet- ween the pediatric (age®15 years) and adult (age>15 years) groups, we conducted a multicenter questionn- aire survey from 16 tirtiary care hospitals in Korea.
MATERIALS AND METHODS
We sent a questionnaire on orbital complications as- sociated with rhinosinusitis (OCRS) to 68 tirtiary care hospitals with otolaryngology training program in Korea.
Sixteen general hospitals replied to the questionnaire with 79 cases that occurred from January 1985 through October 1999. Each center has reported one to fifteen cases individually. Medical history, ophthalmologic and otolaryngologic findings including clinical features
*The authors agree to transfer the copyright of the manuscript
‘Oribital complications of rhinosinusitis:Characteristics in pediatric patients’ to the ‘Journal of Rhinology’.
1Department of Otolaryngology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea
2Department of Otolaryngology, College of Medicine, Seoul National University, Seoul, Korea
Address correspondence and reprint requests to Yong-Jae Kim, M.D., Department of Otolaryngology, University of Ulsan Co- llege of Medicine, Asan Medical Center 388-1 Poongnapdong, Songpagu, Seoul 138-736 Korea
Tel:82-2-2224-3712, Fax:82-2-489-2773 E-mail:[email protected]
Accepted for publication on October 17, 2000
110 / J Rhinol 7(2), 2000
and hospital courses were reviewed. About the clinical data, radiologic findings (including CT scan) were also required. Appropriate CT scan was requested for the evaluation of the involved sinuses in OCRS, but was available only in 29 pediatric patients and 39 adult patients. The informations about their hospital courses, antibiotic treatment measure, microbiologic study result for ordinary bacteria and fungus, applied surgical mo- dalities, and final outcomes were included within the questionnaire.‘Cure’as a treatment result was defined, when the patient was recovered from OCRS without permanent disabilities, or deteriorating to intracranial complications or even to death. The follow-up period ranged between 4 weeks and 3 years with a mean of 12 weeks.
RESULTS Clinical features of OCRS
Thirty-five pediatric patients ranged in age between 8 months and 15 years with a mean of 7 years. OCRS commonly occured in the patients under the age of 15 (35/79, 44.3%)(Table 1). Forty-four patients were in the adult group, but incidence was low in their 20s, 30s and 40s. A relatively small number of patients (17.2%) were between the ages of 20 and 40. Twenty-five (70%) of 35 pediatric patients and 24 (54.6%) of 44 adult patients were male.
Although 8 (22.9%) of 35 pediatric patients and 3 (6.8%) of 44 adult patients had bilateral sinusitis, no case with bilateral orbital complication was noted.
The affected paranasal sinuses underlying OCRS, both in the pediatric and adult patients were summarized in Table 2.
Incidence of orbital complications
In the pediatric patients, the incidence of inflamma- tory edema was 68.6% (24/35 cases), that of orbital cellulitis was 51.4% (18/35 cases), that of orbital abs- cess was 14.3% (5/35 cases), and that of SPA was 14.3% (5/35 cases). In the adults, 65.9% (29/44 cases) had inflammatory edema, 45.5% (20/44 cases) had or- bital cellulitis, 11.4% (5/44 cases) had orbital abscess, 9.1% (4/44 cases) had SPA (Fig. 1), and 18.2% (8/44 cases) had CST (Table 1, 3). Two cases of brain abs- cess were found in this series.
Their chief complaints were shown in Table 4. Fifty- five patients presented with the chief complaints of periorbital swelling, exophthalmos, or proptosis. The other complaints were periorbital pain, hyperrhinorrhea, postnasal drip, nasal block, headache and diplopia in order of frequency. Twenty-nine (96.7%) of 30 pediatric patients characteristically had relatively shorter duration (less than 7 days) of symptoms pertaining to orbital complications, compared with 28 (73.6%) of 38 pati- ents in the adult group (Table 5).
Bacteriologic culture was done with nasal swab from the middle meatus (Table 6). In the pediatric patients, Staphylococci were most frequently identified (10/20, 50.0%), whereas two strains of Streptococcus were
Table 1. Incidence of orbital complications
Children (N=35) Adults (N=44) Inflammatory edema 24 29 Orbital cellulitis 18 20 Orbital abscess 5 5 Subperiosteal abscess 5 4
CST* - 8
*:Cavernous sinus thrombosis
Table 2. Affected sinuses in the pediatric and adult patients Affected sinus Children (N=29) Adults (N=39) Maxillo-ethmoidal sinuses 17 12 Ethmoidal sinus alone 4 6
Maxillo-ethmoido-frontal - 4 Maxillary sinus alone 7 4
Sphenoid sinus alone - 3
Pansinusitis 1 4
Misc. 0 6
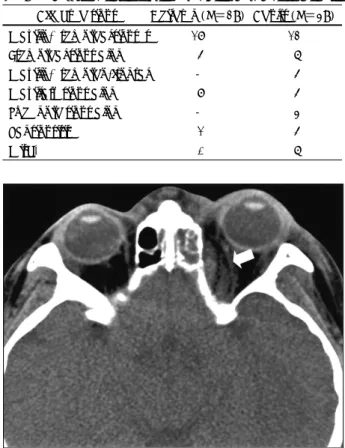
Fig. 1. Axial computerized tomography of a 3-year-old child with subperiosteal abscess on the left side (arrow).
Kim et al:Rhinogenic Orbital Complications / 111
identified, and 45% (9 of 20) of the swabs were sterile.
In the adults, Streptococci were the most frequent or- ganism identified (7/26 cases, 26.9%), but 57.7 % (15 of 26 cases) of the samples were sterile in the patients with orbital complications of rhinosinusitis.
Treatment results of OCRS
The cure rate by surgical treatment in the pediatric patients (14/16, 87.4%) was higher than in the adult patients (21/26, 80.8%). The surgical treatment moda- lities were shown in the Table 7. The cure rate by me- dical treatment in the pediatric patients (18/19, 94.7%) was also higher than in the adult patients (11/16, 68.7%).
Failure cases include 2 cases of progressive intracranial infection spread and 2 cases of mortality due to under- lying malignant lymphoma and complication of diabe- tes mellitus for each case.
DISCUSSIONS
The orbital complications of rhinosinusitis are usually first seen by pediatricians, ophthalmologists, and other physicians rendering primary patient care. Consequently, the diagnosis of OCRS, when referred to otolaryngo- logists, is often delayed, and subsequent permanent sequelae such as loss of vision can also combined with OCRS.4) Inflammatory or pre-septal edema is the most common and mildest form of orbital complications.
Spires et al. reported that inflammatory edema occurred in young children, mostly under 2 years of age and that 226 of 242 patients (93%) were diagnosed with prese- ptal edema.5) In this series, the incidence of inflammatory or pre-septal edema was statistically equivalent in the pediatric group (24/35, 68.5%) with that (29/44, 65.
8%) in the adult patients (Table 1). Many patients with inflammatory edema in the pediatric group may have been successfully treated by primary physicians.
Preseptal edema in infants with a preceding upper res- piratory infection, is usually secondary to H influenzae type B bacteremia and not a complication of sinusitis.
This process does not usually lead to the serious orbital sequelae associated with acute sinusitis, and responds quickly to appropriate antibiotic therapy.6)
It is considered that the frontal and sphenoid sinuses may become clinically significant after 6 years of age.
Accordingly, sinusitis in children under 6 years of age is confined to the maxillary and ethmoid sinuses.7) In this series, the majority of pediatric patients (28/29, 96.
6%) had maxillary and ethmoid sinusitis, but a various combinations of the paranasal sinuses were affected in the adult group (Table 2).
The symptom duration of less than 7 days reflects rapid progression of inflammatory process in the pedia-
Table 3. Age distribution of preseptal and postseptal orbital complications*
Ages Preseptal Postseptal Total 8 months - 4 years 4 7 11
5 - 9 years 4 8 12
10 - 5 years 4 8 12
*:In the adult group, postseptal complications were noted in 68.1% (30/44)
Table 4. Chief complaints of orbital complications Symptom Children
(N=35)
Adults
(N=44) Total Periorbital swelling 24 28 52
Local pain 2 8 10
Nasal obstruction 1 3 4 Hyperrhinorrhea 3 1 4
Exophthalmos 3 - 3
Diplopia - 2 2
Headache - 2 2
Fever 2 - 2
Table 5. Symptom duration of orbital complications Duration of disease Children (N=30) Adults (N=38)
Within 1 week 29 28
1 - 3 weeks 1 6
3 weeks - 3 months - 1
More than 3 months - 3
*:Cavernous sinus thrombosis
Table 6. Bacteria identified from the middle meatus Children (N=20) Adults (N=26) Staphylococci spp. 10 3 Streptococci spp. 2 7
Proteus mirabilis - 1
No growth 9 15
Table 7. Applied surgical modalities for the treatment of or- bital complications
Children (N=16) Adults (N=26) Intranasal ethmoidectomy 7 20 Orbital abscess drainage 5 2 External ethmoidectomy 4 3 Transantral procedure 2 7 Combined procedures 5 9
112 / J Rhinol 7(2), 2000
tric group. Twenty-nine (96.7%) of 30 pediatric patients had relatively shorter duration (less than 7 days) of symptoms pertaining to orbital complications, compared to 28 (73.7%) of 38 patients in the adult group (Table 5). The common chief complaints were periorbital sw- elling (52/79, 65.8%) and pain (10/79, 12.7%) in the total patient group (Table 4).
Radiologic assessment of the orbit by means of plain radiography, ultrasonography, and especially CT is of value in pediatric group for the diagnosis of underlying sinusitis and classification of rhinosinogenic orbital co- mplications.8)9) Coronal CT with enhancement is useful in improving imaging accuracy.10)11) Ultrasonography is not so helpful to evaluate the presence of an abscess, but may be useful in monitoring the amount of perior- bital edema and displacement.12) In this series, the most frequently affected sinus was the maxillary-ethmoid sinuses both in the pediatric (17/29, 58.6%) and the adult (12/39, 30.8%) groups.
Gram staining and culture for conjunctiva, nose and throat may be helpful, but are not always representative of the offending organisms.8)13) Blood culture needs 3 or more days of cultivation to yield the pathogen, and is frequently negative especially if the patients received antibiotic therapy.12) In this series, Staphylococci were the commonest pathogen identified (10/20, 50.0%) from nasal swabs in the pediatric group, whereas Streptoco- cci were in the adult group (7/26, 26.9%).
The indications for surgical drainage include abscess formation demonstrated on CT scan, progression of sy- mptoms (ophthalmoplegia, decreased vision) for more than 48 to 72 hours.14) Blindness or rapidly deteriorating vision is generally considered as an ophthalmologic emergency.12) Surgical exploration is also recommended, regardless of CT findings, for children who initially present with decreased visual acuity or demonstrate progression of orbital manifestation despite medical therapy.15) Recovery of visual acuity is believed better in cases of infectious processes secondary to nonspeci- fic inflammations or mucoceles compared with fungal diseases.16) In this series, the cure rate in the pediatric group by surgical and by medical treatment was higher than that in the adult group. It can be explained by the fact that preseptal edema with a preceding upper respi- ratory infection is not a complication of sinusitis, but usually is secondary to H influenzae bacteremia6) and
can easily resolved without serious sequelae as in the adult group.
CONCLUSION
Orbital complications in the pediatric rhinosinusitis patients have short duration of symptoms and develop as various forms-inflammatory edema, orbital cellulitis, orbital abscess and subperiosteal abscess. How-ever, early diagnosis and appropriate management usually result in better outcome in the pediatric patients than in the adult patients.
REFERENCES
1) Williamson-Noble FA. Disease of the orbit and its contents seco- ndary to pathological conditons of the nose and paranasal sinuses.
Ann Roy Surg Eng 1954;15:46-64.
2) Maniglia AJ. Fatal and major complications secondary to nasal and sinus surgery. Laryngoscope 1989;99:276-83.
3) Stankiewicz JA. Complications in endoscopic intranasal ethmoi- dectomy: An update. Laryngoscope 1989;99:686-90.
4) Chandler JR, Langenbranner DJ, Stevens ER. The pathogenesis of orbital complications in acute sinusitis. Laryngoscope 1970;80:
1414-8.
5) Spires JR, Smith RJH. Bacterial infections of the orbital and periorbital soft-tissues in children. Laryngoscope 1986;96:763-7.
6) Skedros DG, Haddad J, Bluestone CD, Curtin HD. Subperiosteal abscesses in children: Diagnosis, microbiology, and management.
Laryngoscope 1993;103:28-32.
7) Fearon B, Edmonds B, Bird R. Orbital-facial complications of si- nusitis in children. Laryngoscope 1979;78:947-53.
8) Gellady AM, Shulman ST, Ayoub EM. Periorbital and orbital cellulitis in children. Pediatrics 1978;61:272-7.
9) Goodwin WJ Jr, Weinnshall M, Chandler JR. The role of high resolution computerized tomography and standardized ultrasound in the evaluation of orbital cellulitis. Laryngoscope 1982;92:
728-31.
10) Towbin R, Bokyung KH, Kaufman RA, Burke M. Postseptal cellu- litis: CT in diagnosis and management. Radiology 1986;158:735-7.
11) Langham-Brown JJ, Rhy-Williams S. Computed tomography of the acute orbital infection: The importance of coranal section.
Clin Radiol 1989;40:471-4.
12) Harris GJ. Subperiosteal abscess of the orbit. Arch Ophthalmol 1983;101:751-7.
13) Haynes RE, Cramblett HG. Acute ethmoiditis; Its relatiionship to orbital cellulitis. Am J Dis Child 1967;114:261-7.
14) Schramm VL, Curtin HD, Kennerdell JS. Evaluation of orbital cellulitis and results of treatment. Laryngoscope 1982;80:732-8.
15) Clary RA, Cunningham MJ, Eavey RD. Orbital complications of acute sinusitis: Comparison of computed tomography scan and surgical findings. Ann Otol Rhinol Laryngol 1992;101:598-600.
16) Maniglia AJ, Kronenberg FG, Culbertson W. Visual loss asso- ciated with orbital and sinus diseases. Laryngoscope 1984;94:
1050-9.