Original Article
Dexmedetomidine을 투여한 내과중환자실 환자의 심혈관계 부작용 발생률과 위험인자 분석
안혜림†, 김지원, 안서현, 박애령, 황보신이 가톨릭대학교 서울성모병원 약제부
Incidence and Risk Factors for Dexmedetomidine-Associated Cardiovascular Adverse Effects in Intensive Care Unit Patients
Hye Lim Ahn†, Ji Won Kim, Seo Hyun Ahn, Ae Ryoung Park, Shin-Yi Hwangbo
Department of Pharmacy, Seoul St. Mary’s Hospital, The Catholic University of Korea 222 Banpo-daero, Seocho-gu, Seoul, 06591, Republic of Korea
Background : Dexmedetomidine is a selective α2 agonist with sedative, analgesic, and sympa- tholytic properties. Dexmedetomidine has cardiovascular risks such as hypotension and brad- ycardia. For this reason, the U.S. Food and Drug Administration (FDA) recommends the short- term use of dexmedetomidine less than 24 hours. Therefore, this study was aimed at analyzing the current status and risk factors of the cardiovascular side effects of dexmedetomidine.
Methods : A retrospective chart review of all adult critically ill patients in the medical inten- sive care units who received dexmedetomidine from January 2016 to May 2017 was performed.
The incidence, risk factors and prognosis of the cardiovascular adverse effects were analyzed.
Results : The total number of patients was 135, and the mean hours of dexmedetomidine ad- ministration was 165 hours. A total of 102 patients (75.6%) developed cardiovascular side ef- fects. Among them, hypotension occurred in 99 patients (73.3%), of which 53 patients (53.5%) developed hypotension within 24 hours. Bradycardia occurred in eight patients (5.9%), of which two patients (25.0%) developed bradycardia within 24 hours.
Multivariate analysis of the risk factors for hypotension showed an association between hy- 투고일자 2020.3.24; 심사완료일자 2020.4.22; 게재확정일자 2020.7.7
†교신저자 안혜림 Tel:02-2258-2566 E-mail:[email protected]
potension and low baseline mean arterial pressure (MAP)(p=0.028), patients with acute res- piratory distress syndrome (ARDS)(p=0.030) and those given norepinephrine (p=0.017). The incidence of hypotension was lower in patients with underlying hypertension (p=0.030).
Univariate analysis of the risk factors for bradycardia showed that the incidence of brady- cardia was higher in patients with lower baseline heart rates (p=0.033), higher body weight (p=0.008), and those undergoing hemodialysis (p=0.009).
Also, there were no significant differences in the days of mechanical ventilation, the number of hospital days, and the mortality rate in patients with hypotension or bradycardia.
Conclusion : Dexmedetomidine was associated with a higher incidence of cardiovascular side effects. Specifically, patients who were diagnosed with lower MAP, ARDS, or in combination with norepinephrine use were more likely to develop hypotension. Therefore, it is necessary to closely monitor cardiovascular adverse effects in patients with these risk factors.
[Key words] Dexmedetomidine, Hypotension, Bradycardia, Cardiovascular adverse events, Critically ill patients
중환자는 기저질환과 침습적 시술, 기계환기 등으 로 인해 통증, 불안, 불편감을 경험하며,1) 이로 인한 심적, 육체적 고통은 섬망이나 혈역학적 불안정, 조 직손상, 스트레스심근병증 등을 초래할 수 있다. 이 는 궁극적으로 재원일수 증가, 사망률 증가 등의 부정 적인 임상결과로 이어질 수 있으므로,2) 환자의 스트 레스를 완화시키고 시술을 용이하게 해줄 수 있는 적 절한 진통 및 진정요법이 필수적이다.
중환자실에서 자주 사용되는 진정제로는 propo- fol, benzodiazepines (diazepam, lorazepam, midazolam), dexmedetomidine 등이 있다.3),4) Dexmedetomidine은 선택적 α2 아드레날린 효 능제로서 중추신경계에서 norepinephrine의 분비 를 억제하여 진정 및 진통 효과를 동시에 가지며, 빠 른 작용발현과 짧은 작용시간을 특징으로 하는 약 물이다.5) 또한, gamma-aminobutyric acid (G- ABA) 수용체에 작용하는 propofol이나 benzodi- azepine계 약물이 깊은 수준의 진정을 유도하여 그 에 따른 섬망, 호흡억제 등의 부작용이 발생할 수 있 는 반면에3),6) dexmedetomidine은 GABA 수용 체에 작용하지 않기 때문에 호흡억제 작용이 없고7) 섬망 발생을 감소시키며8) 진통 작용에 따른 아편양 보존 효과가 있어9) 중환자에게 사용이 적합한 진정제
로 생각되고 있다. 현재 식품의약품안전처 허가사항 에서 성인의 집중치료 관리 하 진정 요법으로 10~20 분간 1 mcg/kg의 부하용량을 주입하고, 이어서 시 간 당 0.2~0.7 mcg/kg를 유지용량으로 투여하도 록 권고하고 있다. 하지만, 약물의 작용기전에 의해 저혈압, 서맥 등의 심혈관계 부작용의 발생 가능성 이 있고,10) 장시간 사용과 관련된 연구가 부족하다는 이유로 미국 Food and Drug Administration (FDA)에서는 24시간 이내의 단시간 사용만을 권고 하고 있는 실정이다. 그럼에도 불구하고 실제 임상 현 장에서는 dexmedetomidine을 24시간 이상 사용 하는 경우가 많으며, 전 세계적으로도 2008년 처음 으로 콜롬비아에서 dexmedetomidine 장시간 사 용이 허가된 이후 우리나라를 비롯한 여러 국가에서 dexmedetomidine 장시간 사용이 승인되어 있 다.11) 이에 본 연구에서는 본원의 내과중환자실에서 dexmedetomidine을 투여한 환자를 대상으로 심 혈관계 부작용의 발생률과 발생시간을 확인하여 안전 성을 평가하고, 이상반응 발생의 위험인자를 분석하 고자 하였다.
연구방법
1. 연구대상 및 연구기간
2016년 1월부터 2017년 5월까지 가톨릭대학교 서 울성모병원 내과중환자실에 입원한 환자 중 dex- medetomidine을 투여한 환자를 대상으로 하였고, 이 중 18세 미만의 소아 및 청소년, 입실 당시 mean arterial pressure (MAP)가 60 mmHg 미만이 거나 입실 시 heart rate이 분당 50회 미만인 환자 는 제외하였다.
2. 평가항목 및 평가기준
1) 심혈관계 부작용 평가
Dexmedetomidine 투여에 따른 심혈관계 부작용 으로서 저혈압과 서맥의 발생률과 발생시간, 약제 용 량에 따른 발생률의 차이를 조사하였다. 이때, 저혈압 은 dexmedetomidine 투여 후 MAP가 60 mmHg 미만으로 감소된 경우로, 서맥은 투여 후 heart rate 이 분당 50회 미만으로 감소된 경우로 정의하였다. 심 혈관계 부작용 개선을 위해 사용한 치료방법도 확인하 였다.
2) 심혈관계 부작용 발생 위험인자 평가
부작용 발생 위험인자 분석을 위해 저혈압 발생군과 비발생군을 각각 Hypo군, Non-hypo군으로, 서맥 발생군과 비발생군을 각각 Brady군, Non-brady 군으로 명명하였다. 그리고 각 군의 성별, 연령, 키, 체중, 진단명, acute physiology and chronic health evaluation (APACHE) II score, 기저 질환, 병용약물, dexmedetomidine 투여 용량 및 투여 기간, 입실 당시 MAP, heart rate을 비교, 분석하여, 심혈관계 부작용 발생에 영향을 미치는 독 립적 위험인자가 있는지 확인하였다.
3) 예후 평가
저혈압과 서맥의 발생군과 비발생군의 기계환기 일 수 및 병원 재원일수, 중환자실 재원일수와 사망률을 비교하여, 심혈관계 부작용 발생이 예후에 미치는 영
향을 조사하였다.
3. 통계분석
연속형 변수는 Independent t test 또는 Wil- coxon rank sum test를 사용하여 분석하였고, 범 주형 변수에 대해서는 Chi-square test 또는 Fi- sher’s exact test를 사용하였다.
Dexmedetomidine 투여에 따른 심혈관계 부작 용 발생 위험인자 분석은 단변량 로지스틱 회귀분석 법을 사용하였고, 단변량 분석 결과 p<0.10인 항목 에 대하여 다변량 로지스틱 회귀분석을 시행하였다.
다변량 분석 결과 p<0.05인 경우를 통계적으로 유 의한 결과로 판단하였다.
모든 분석에는 SAS software, version 9.4 (SAS Institute Inc. Cary, NC)을 사용하였다.
본 연구는 환자의 전자의무기록 조회를 통한 후향적 관찰연구로서, 환자의 정보를 이용하기 위하여 가톨 릭대학교 서울성모병원 임상시험심사위원회로부터 연구계획서를 승인 받아 진행하였다(과제번호: KC1 7RESI0620).
연구결과 1. 대상 환자 특성
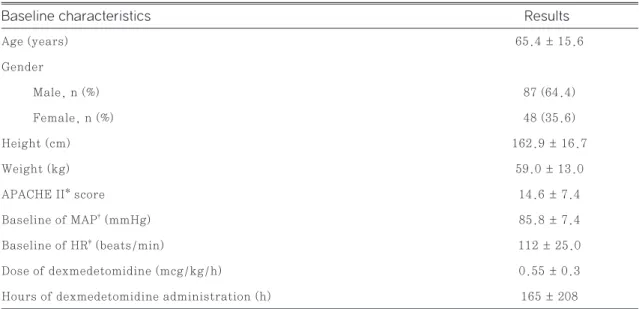
연구대상 환자는 총 135명이었고 dexmedeto- midine의 평균 투여기간은 165시간(약 6.9일)이었 다. 평균 투여 용량은 0.55 mcg/kg/h로 허가 용량 인 0.2~0.7 mcg/kg/h 이내에 해당하였다. 평균 APACHE II score는 14.6점이었고, 기저 MAP는 85.8 mmHg, 기저 heart rate은 분 당 112회 이 었다(Table 1).
2. 부작용 평가
대상 환자 총 135명 중 102명(75.6%)에서 심혈관 계 부작용이 발생하였다. 저혈압은 99명(73.3%)에 서 발생하였으며, 이 중 53명(53.5%)은 투여 24시 간 이내에 발생하였다(Fig. 1). 서맥은 8명(5.9%) 에서 발생하였으며, 이 중 2명(25.0%)은 24시간 이
내에 발생하였다(Fig. 2). 저혈압과 서맥 모두 발생 된 환자는 5명이었다.
Dexmedetomidine 투여 시작 후 평균 부작용 발 생 시간은 저혈압이 57.2±101.8시간, 서맥이 45.8
±35.7시간이었다.
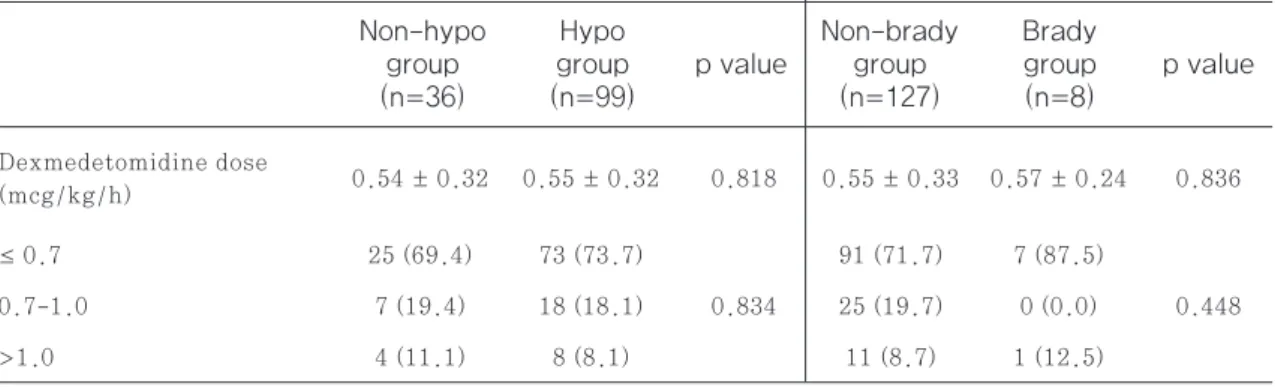
저혈압과 서맥 발생률은 dexmedetomidine 투여 용량에 따라 유의한 차이가 없었으며(p=0.834, p=
0.448)(Table 2), 부작용 개선을 위해 가장 많이 사 용된 치료방법은 수액 투여, 다음으로는 norepi- nephrine 투여 및 증량이었다(Fig. 3).
3. 부작용 발생 위험인자 평가
1) 저혈압
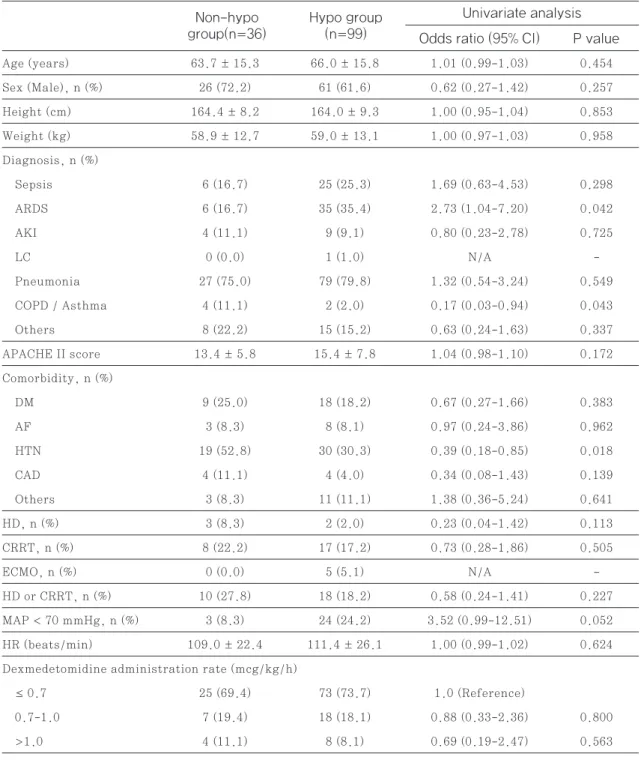
저혈압 발생군(Hypo군)과 저혈압 비발생군(Non -hypo군)의 환자 특성을 단변량 분석으로 비교한 결과, Hypo군에서 ARDS (acute respiratory distress syndrome) 환자 비율이 유의하게 높았고 (p=0.042), 고혈압을 기저질환으로 가진 비율은 유의 하게 낮았다(p=0.018). 또한, 입실 당시 MAP가 70
Age (years) 65.4 ± 15.6
Gender
Male, n (%) 87 (64.4)
Female, n (%) 48 (35.6)
Height (cm) 162.9 ± 16.7
Weight (kg) 59.0 ± 13.0
APACHE II* score 14.6 ± 7.4
Baseline of MAP† (mmHg) 85.8 ± 7.4
Baseline of HR‡ (beats/min) 112 ± 25.0
Dose of dexmedetomidine (mcg/kg/h) 0.55 ± 0.3
Hours of dexmedetomidine administration (h) 165 ± 208
Table 1 Baseline characteristics of study population (n=135)
Fig. 1 Incidence of hypotension (n=135) Fig. 2 Incidence of bradycardia (n=135) Results Baseline characteristics
Data are expressed as numbers (%) of patients or as mean ± standard deviation (SD).
*APACHE II score; acute physiology and chronic health evaluation [severity-of-illness index], †MAP; mean arterial pressure, ‡HR;
heart rate
No.
36 (26.7%) Yes.
99 (73.3%)
≤24h 53 (53.5%)
>24h 46 (46.5%)
No.
127 (94.1%) Yes.
8 (5.9%)
≤24h 2 (25.0%)
>24h 6 (75.0%)
mmHg 미만이었던 환자 비율은 저혈압 발생군에서 24.2%, 비발생군에서 8.3%이었다(p=0. 052).
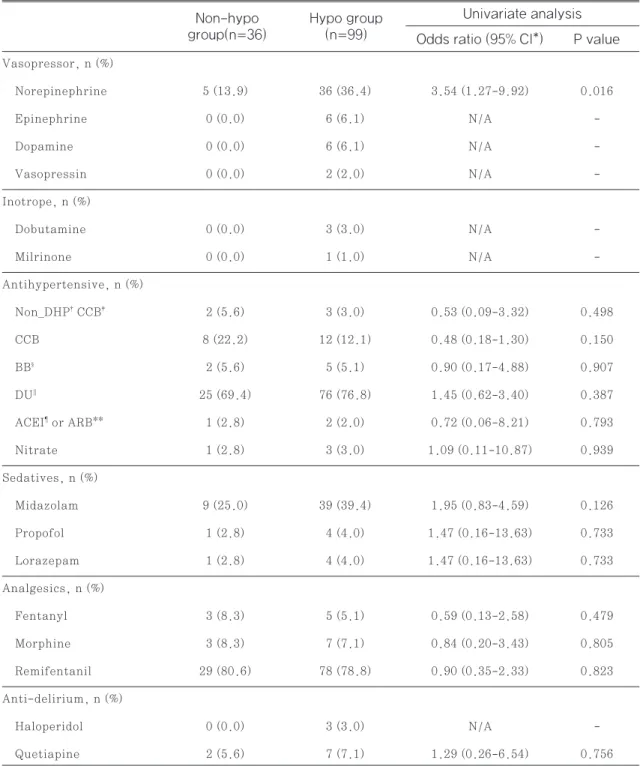
병용 약물을 조사한 결과에서는 norepinephrine 투여 환자 비율이 Hypo군에서 유의하게 높았다(p=
0.016). 그 외의 특성은 두 군에서 유의한 차이가 없 었다(Table 3, Table 4).
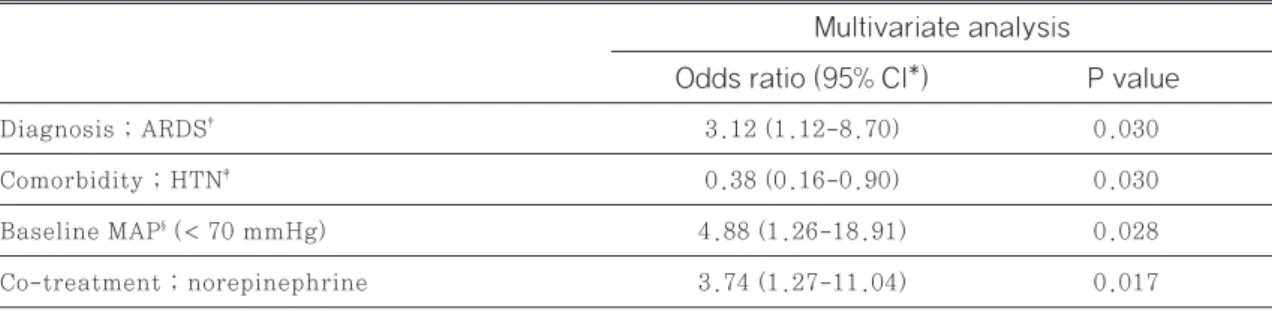
단변량 분석 결과에서 p value 0.1 미만이었던 ARDS, 고혈압, 입실 시 MAP 70 mmHg 미만, no- repinephrine 병용에 대하여 다변량 분석을 시행 한 결과, ARDS 환자의 경우(OR 3.12, 95% CI 1.12-8.70, p=0.030), 입실 시 MAP가 70 mm Hg 미만인 경우(OR 4.88, 95% CI 1.26-18.91, p=0.028), norepinephrine을 병용중인 경우(OR 3.74, 95% CI 1.27-11.04, p=0.017) 저혈압 발 생률이 유의하게 높았으며, 고혈압을 기저질환으로
가진 경우 저혈압 발생률이 유의하게 낮았다(OR 0.38, 95% CI 0.16-0.90, p=0.030)(Table 5).
2) 서맥
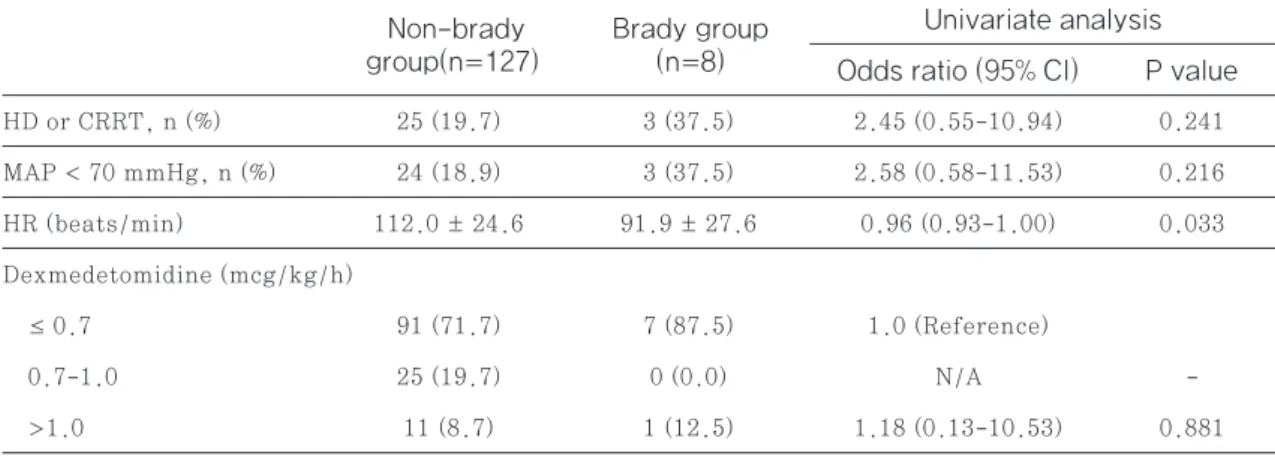
Dexmedetomidine 투여 후 서맥 발생 위험인자 에 대한 단변량 분석 결과, 체중이 무거울수록(OR 1.06 95% CI 1.02-1.11, p=0.008), 혈액 투석 을 받은 경우(OR 13.78 95% CI 1.93-98.58, p=0.009), 입실 시 heart rate이 낮을수록 (OR 0.96 95% CI 0.93-1.00, p=0.033) 서맥 발생 률이 유의하게 높았다. 하지만 서맥 발생률 자체가 낮 아 서맥 위험인자에 대한 다변량 분석은 실시하지 못 하였다(Table 6). 병용 약물을 조사한 결과 서맥 발 생에 유의한 영향을 미치는 약물은 없었다(Table 7).
Fig. 3 Treatment for dexmedetomidine-associated cardiovascular adverse effects 0.54 ± 0.32 0.55 ± 0.32 0.818 0.55 ± 0.33 0.57 ± 0.24 0.836
≤ 0.7 25 (69.4) 73 (73.7) 91 (71.7) 7 (87.5)
0.7-1.0 7 (19.4) 18 (18.1) 0.834 25 (19.7) 0 (0.0) 0.448
>1.0 4 (11.1) 8 (8.1) 11 (8.7) 1 (12.5)
Dexmedetomidine dose (mcg/kg/h)
Table 2 Comparisons of adverse effects according to dosing of dexmedetomidine
p value
p value Brady
group (n=8) groupHypo
(n=99)
Non-brady group (n=127) Non-hypo
group (n=36)
Data are expressed as numbers (%) of patients or as mean ± standard deviation (SD).
DMT; dexmedetomidine, NE; norepinephrine
Age (years) 63.7 ± 15.3 66.0 ± 15.8 1.01 (0.99-1.03) 0.454
Sex (Male), n (%) 26 (72.2) 61 (61.6) 0.62 (0.27-1.42) 0.257
Height (cm) 164.4 ± 8.2 164.0 ± 9.3 1.00 (0.95-1.04) 0.853
Weight (kg) 58.9 ± 12.7 59.0 ± 13.1 1.00 (0.97-1.03) 0.958
Diagnosis, n (%)
Sepsis 6 (16.7) 25 (25.3) 1.69 (0.63-4.53) 0.298
ARDS 6 (16.7) 35 (35.4) 2.73 (1.04-7.20) 0.042
AKI 4 (11.1) 9 (9.1) 0.80 (0.23-2.78) 0.725
LC 0 (0.0) 1 (1.0) N/A -
Pneumonia 27 (75.0) 79 (79.8) 1.32 (0.54-3.24) 0.549
COPD / Asthma 4 (11.1) 2 (2.0) 0.17 (0.03-0.94) 0.043
Others 8 (22.2) 15 (15.2) 0.63 (0.24-1.63) 0.337
APACHE II score 13.4 ± 5.8 15.4 ± 7.8 1.04 (0.98-1.10) 0.172
Comorbidity, n (%)
DM 9 (25.0) 18 (18.2) 0.67 (0.27-1.66) 0.383
AF 3 (8.3) 8 (8.1) 0.97 (0.24-3.86) 0.962
HTN 19 (52.8) 30 (30.3) 0.39 (0.18-0.85) 0.018
CAD 4 (11.1) 4 (4.0) 0.34 (0.08-1.43) 0.139
Others 3 (8.3) 11 (11.1) 1.38 (0.36-5.24) 0.641
HD, n (%) 3 (8.3) 2 (2.0) 0.23 (0.04-1.42) 0.113
CRRT, n (%) 8 (22.2) 17 (17.2) 0.73 (0.28-1.86) 0.505
ECMO, n (%) 0 (0.0) 5 (5.1) N/A -
HD or CRRT, n (%) 10 (27.8) 18 (18.2) 0.58 (0.24-1.41) 0.227
MAP < 70 mmHg, n (%) 3 (8.3) 24 (24.2) 3.52 (0.99-12.51) 0.052 HR (beats/min) 109.0 ± 22.4 111.4 ± 26.1 1.00 (0.99-1.02) 0.624 Dexmedetomidine administration rate (mcg/kg/h)
≤ 0.7 25 (69.4) 73 (73.7) 1.0 (Reference)
0.7-1.0 7 (19.4) 18 (18.1) 0.88 (0.33-2.36) 0.800
>1.0 4 (11.1) 8 (8.1) 0.69 (0.19-2.47) 0.563
Table 3 Logistic regression between hypotension and variables (Univariate analysis)
P value Odds ratio (95% CI)
Hypo group (n=99)
Univariate analysis Non-hypo
group(n=36)
Data are expressed as numbers (%) of patients or as mean ± standard deviation (SD).
CI; confidence interval, ARDS; acute renal distress syndrome, AKI; acute kidney injury, LC; liver cirrhosis, COPD; chronic obstructive pulmonary disease, DM; diabetes mellitus, AF; atrial fibrillation, HTN; hypertension, CAD; coronary artery disease, HD; hemodialysis, CRRT; continuous renal replacement therapy, ECMO; extracorporeal membrane oxygenation, MAP; mean arterial pressure, HR; heart rate
Vasopressor, n (%)
Norepinephrine 5 (13.9) 36 (36.4) 3.54 (1.27-9.92) 0.016
Epinephrine 0 (0.0) 6 (6.1) N/A -
Dopamine 0 (0.0) 6 (6.1) N/A -
Vasopressin 0 (0.0) 2 (2.0) N/A -
Inotrope, n (%)
Dobutamine 0 (0.0) 3 (3.0) N/A -
Milrinone 0 (0.0) 1 (1.0) N/A -
Antihypertensive, n (%)
Non_DHP† CCB‡ 2 (5.6) 3 (3.0) 0.53 (0.09-3.32) 0.498
CCB 8 (22.2) 12 (12.1) 0.48 (0.18-1.30) 0.150
BB§ 2 (5.6) 5 (5.1) 0.90 (0.17-4.88) 0.907
DU∥ 25 (69.4) 76 (76.8) 1.45 (0.62-3.40) 0.387
ACEI¶ or ARB** 1 (2.8) 2 (2.0) 0.72 (0.06-8.21) 0.793
Nitrate 1 (2.8) 3 (3.0) 1.09 (0.11-10.87) 0.939
Sedatives, n (%)
Midazolam 9 (25.0) 39 (39.4) 1.95 (0.83-4.59) 0.126
Propofol 1 (2.8) 4 (4.0) 1.47 (0.16-13.63) 0.733
Lorazepam 1 (2.8) 4 (4.0) 1.47 (0.16-13.63) 0.733
Analgesics, n (%)
Fentanyl 3 (8.3) 5 (5.1) 0.59 (0.13-2.58) 0.479
Morphine 3 (8.3) 7 (7.1) 0.84 (0.20-3.43) 0.805
Remifentanil 29 (80.6) 78 (78.8) 0.90 (0.35-2.33) 0.823
Anti-delirium, n (%)
Haloperidol 0 (0.0) 3 (3.0) N/A -
Quetiapine 2 (5.6) 7 (7.1) 1.29 (0.26-6.54) 0.756
Table 4 Logistic regression on co-treatment in hypotension adverse events (univariate analysis)
P value Odds ratio (95% CI*)
Hypo group (n=99)
Univariate analysis Non-hypo
group(n=36)
*CI; confidence interval, †DHP; dihydropyridine, ‡CCB; calcium channel blocker, §BB; beta blocker, ∥DU; diuretics, ¶ACEI; angioten- sin converting enzyme inhibitor, **ARB; angiotensin II receptor blocker
Age (years) 65.9 ± 15.5 56.5 ± 15.6 0.97 (0.93-1.01) 0.106
Sex (Male), n (%) 82 (64.6) 5 (62.5) 0.92 (0.21-4.01) 0.906
Height (cm) 164.1 ± 9.1 163.5 ± 6.5 0.99 (0.92-1.07) 0.832
Weight (kg) 58.2 ± 12.3 71.7 ± 17.1 1.06 (1.02-1.11) 0.008
Diagnosis, n (%)
Sepsis 31 (24.4) 0 (0.0) N/A -
ARDS 37 (29.1) 4 (50.0) 2.43 (0.58-10.24) 0.226
AKI 13 (10.2) 0 (0.0) N/A
Pneumonia 100 (78.7) 6 (75.0) 0.81 (0.16-4.24) 0.803
COPD / Asthma 6 (4.7) 0 (0.0) N/A -
Others 22 (17.3) 1 (12.5) 0.68 (0.08-5.83) 0.726
APACHE II score 15.0 ± 7.3 13.3 ± 6.7 0.97 (0.87-1.07) 0.517
Comorbidity, n (%)
DM 27 (21.3) 0 (0.0) N/A -
AF 9 (7.1) 2 (25.0) 4.37 (0.77-24.85) 0.096
HTN 47 (37.0) 2 (25.0) 0.57 (0.11-2.93) 0.498
CAD 8 (6.3) 0 (0.0) N/A -
Others 13 (10.2) 1 (12.5) 1.25 (0.14-11.00) 0.839
HD, n (%) 3 (2.4) 2 (25.0) 13.78 (1.93-98.58) 0.009
CRRT, n (%) 22 (17.3) 3 (37.5) 2.86 (0.64-12.88) 0.170
ECMO, n (%) 4 (3.2) 1 (12.5) 4.39 (0.43-44.70) 0.211
Table 6 Logistic regression on risk factors of bradycardia adverse events (Univariate analysis)
P value Odds ratio (95% CI)
Brady group (n=8)
Univariate analysis Non-brady
group(n=127)
*CI; confidence interval, †ARDS; acute renal distress syndrome, ‡HTN; hypertension, §MAP; mean arterial pressure
Diagnosis ; ARDS† 3.12 (1.12-8.70) 0.030
Comorbidity ; HTN‡ 0.38 (0.16-0.90) 0.030
Baseline MAP§ (< 70 mmHg) 4.88 (1.26-18.91) 0.028
Co-treatment ; norepinephrine 3.74 (1.27-11.04) 0.017
Table 5 Logistic regression between hypotension and variables (Multivariate analysis)
P value Odds ratio (95% CI*)
Multivariate analysis
HD or CRRT, n (%) 25 (19.7) 3 (37.5) 2.45 (0.55-10.94) 0.241 MAP < 70 mmHg, n (%) 24 (18.9) 3 (37.5) 2.58 (0.58-11.53) 0.216 HR (beats/min) 112.0 ± 24.6 91.9 ± 27.6 0.96 (0.93-1.00) 0.033 Dexmedetomidine (mcg/kg/h)
≤ 0.7 91 (71.7) 7 (87.5) 1.0 (Reference)
0.7-1.0 25 (19.7) 0 (0.0) N/A -
>1.0 11 (8.7) 1 (12.5) 1.18 (0.13-10.53) 0.881
P value Odds ratio (95% CI)
Brady group (n=8)
Univariate analysis Non-brady
group(n=127)
Data are expressed as numbers (%) of patients or as mean ± standard deviation (SD).
CI; confidence interval, ARDS; acute renal distress syndrome, AKI; acute kidney injury, LC; liver cirrhosis, COPD; chronic ob- structive pulmonary disease, DM; diabetes mellitus, AF; atrial fibrillation, HTN; hypertension, CAD; coronary artery disease, HD;
hemodialysis, CRRT; continuous renal replacement therapy, ECMO; extracorporeal membrane oxygenation, MAP; mean arterial pressure, HR; heart rate
Vasopressor, n (%)
Norepinephrine 40 (31.5) 1 (12.5) 0.31 (0.04-2.61) 0.282
Epinephrine 6 (4.7) 0 (0.0) N/A -
Dopamine 6 (4.7) 0 (0.0) N/A -
Vasopressin 2 (1.6) 0 (0.0) N/A -
Inotrope, n (%)
Dobutamine 3 (2.4) 0 (0.0) N/A -
Milrinone 1 (0.8) 0 (0.0) N/A -
Antihypertensive, n (%)
Non_DHP† CCB‡ 5 (3.9) 0 (0.0) N/A -
CCB 18 (14.2) 2 (25.0) 2.02 (0.38-10.79) 0.412
BB§ 6 (4.7) 1 (12.5) 2.88 (0.30-27.33) 0.357
DU∥ 94 (74.0) 7 (87.5) 2.46 (0.29-20.73) 0.409
ACEI¶ or ARB** 3 (2.4) 0 (0.0) N/A -
Nitrate 4 (3.2) 0 (0.0) N/A -
Sedatives, n (%)
Table 7 Logistic regression on co-treatment in bradycardia adverse events (Univariate analysis) Non-brady
group(n=127) Odds ratio (95% CI*) P value Brady group
(n=8)
Univariate analysis
4. 예후 평가
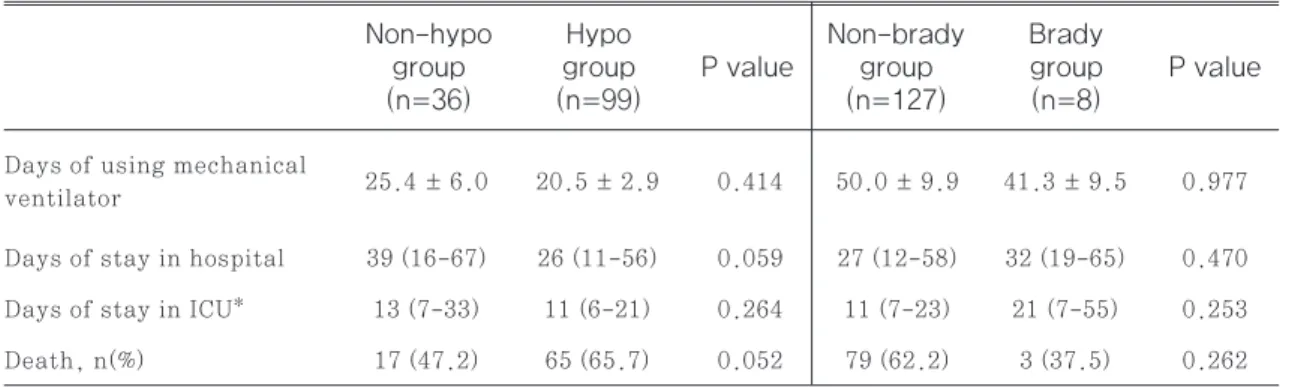
Dexmedetomidine 투여에 따른 저혈압과 서맥 의 발생군과 비발생군의 예후를 평가하였다. 그 결과 저혈압과 서맥 각각에서 부작용 발생에 따른 기계환 기 일수, 병원 및 중환자실 재원일수, 사망률 모두 유 의한 차이가 없었다(Table 8).
고찰
중환자실에서 시행되는 기계환기는 환자에게 불편 감, 통증 및 불안을 유발하게 되며 이로 인해 의식장 애를 동반한 섬망까지 초래할 수 있다.11) 중환자의 조 절되지 않는 통증과 섬망은 단기 및 장기 생존율의 저 하로 이어질 수 있으므로 적절한 진정요법이 필요하 다.12)
Dexmedetomidine은 GABA 수용체를 통해 작 용하는 propofol, benzodiazepines과 같은 기존 진정제와 달리 호흡 억제 작용 없이 약리작용을 나타 낼 수 있고,7) 섬망 유도를 최소화 할 수 있다는 점에 서8) 중환자실에서 사용하기에 적합한 진정제로 생각 되고 있다. 하지만 약물 기전에 의해 저혈압, 서맥과
같은 심혈관계 부작용이 발생할 수 있으며7) 특히 저 혈압의 경우 연구 결과에 따라 13~98%의 다양한 발 생률을 보이고 있어,13)-15) dexmedetomidine이 처음 허가된 이후 적절한 용법 용량과 투여기간에 관 한 논쟁이 계속되고 있다.16),17)
본 연구 결과 135명 중 102명(75.6%)에서 심혈관 계 부작용이 발생하였고, 특히 저혈압은 99명(73.3
%)에서 발생하여 매우 높은 부작용 발생률을 보였다.
본 연구에서 저혈압에 대한 독립적 위험인자로는 ARDS 진단, 입실 시 MAP 70 mmHg 미만, nor- epinephrine 병용 등 세가지가 도출되었다.
연구 기간 내 본원 내과중환자실에 입원한 환자의 평균 MAP는 85.8±7.4 mmHg로 비교적 낮은 평 균 동맥압을 보였다. 이는 중환자실에 입원 중인 환자 들의 경우 기저 상태로 인하여 정상보다 낮은 혈압을 보일 수 있음을 시사한다. 기저 혈압의 영향을 평가하 기 위해 입실 당시 MAP가 70 mmHg 미만인 경우 와 이상인 경우로 나누어 평가한 결과, 입실 당시 MAP가 70 mmHg 미만이었던 군에서 dexme- detomidine 투여로 인한 저혈압 발생 위험이 더 높 았다. Anthony T의 연구 결과 역시 기저 MAP가 70 mmHg 미만인 환자에서 저혈압 발생 가능성이
Midazolam 46 (36.2) 2 (25.0) 0.59 (0.11-3.03) 0.525
Propofol 4 (3.2) 1 (12.5) 4.39 (0.43-44.70) 0.211
Lorazepam 4 (3.2) 1 (12.5) 4.39 (0.43-44.70) 0.211
Analgesics, n (%)
Fentanyl 7 (5.5) 1 (12.5) 2.45 (0.26-22.77) 0.431
Morphine 10 (7.9) 0 (0.0) N/A -
Remifentanil 101 (79.5) 6 (75.0) 0.77 (0.15-4.05) 0.760
Anti-delirium, n (%)
Haloperidol 3 (2.4) 0 (0.0) N/A -
Quetiapine 9 (7.1) 0 (0.0) N/A -
Non-brady
group(n=127) Odds ratio (95% CI) P value Brady group
(n=8)
Univariate analysis
*CI; confidence interval, †DHP; dihydropyridine, ‡CCB; calcium channel blocker, §BB; beta blocker, ∥DU; diuretics, ¶ACEI; angioten- sin converting enzyme inhibitor, **ARB; angiotensin II receptor blocker
유의하게 더 높았다.18) 그러므로 입실 당시 혈압이 낮 은 환자는 dexmedetomidine 투여 시 특별한 주의 가 필요하고, 투여 중에도 면밀한 모니터링을 통하여 부작용 발생을 감지하는 것이 필요하다.
ARDS는 패혈증, 외상, 약물중독 등 다양한 내과 적, 외과적 질환과 연관되어 호흡부전, 심한 동맥혈 저산소혈증, 흉부 X-선상 양측성 미만성 폐침윤을 보이는 임상 증후군을 말한다. ARDS를 유발하는 가 장 흔한 질환으로는 패혈증이 있고, 패혈증 시 ARDS 발생 위험이 약 40%에 이르고 있다.19),20) 이번 연구 결과 내과중환자실 입실 당시 ARDS를 진단 받은 환 자에서 저혈압 발생률이 유의하게 높았다. ARDS를 진단 받은 환자는 연구 대상자 135명 중 41명(30.4
%)으로 이 중 폐렴을 함께 진단받은 환자는 35명 (85.4%), 폐렴과 패혈증을 함께 진단받은 환자는 7 명(17.1%)이었다. 중환자실 재원 환자의 경우 폐렴 에 의하여 패혈증이 발생하는 경우가 많고, 패혈증을 진단받은 경우 저혈압 가능성이 더 높아진다.21) AR DS와 저혈압의 직접적인 상관관계에 대한 연구는 많 지 않으나, 본 연구에서 ARDS 진단이 타 병존 질 환에 상관없이 dexmedetomidine에 의한 저혈압 발생을 높이는 독립적 위험인자로 평가됨에 따라 ARDS로 진단받은 경우 dexmedetomidine 투여 시 면밀한 혈압 모니터링이 필요하겠다.
Norepinephrine을 병용중인 환자에서 저혈압 발 생이 유의하게 많았으나 norepinephrine이 강력 한 승압 효과를 가진 약물이라는 점에서 약물 자체로
인한 위험으로 판단하기는 어렵다. 즉, norepi- nephrine의 투여가 필요한 환자는 혈역학적으로 불 안정한 상태이고 norepinephrine 투여로 조절되 고 있던 혈압이 dexmedetomidine 투여로 인해 다 시 낮아지는 상황이 발생된 것으로 추정할 수 있다.
당연한 결과로 고혈압을 기저질환으로 가진 환자에 서는 dexmedetomidine에 의한 저혈압 발생이 유 의하게 적었다.
서맥은 총 8명(5.9%)의 환자에서 발생하였는데, 입실 시 heart rate이 낮을수록, 체중이 무거울 수 록, 혈액투석을 실시한 환자일 수록 서맥 발생률이 더 높았으나 발생률 자체가 낮아서 다변량 회귀분석을 통한 독립적 위험인자 확인은 불가하였다.
Dexmedetomidine의 용량이 증가함에 따라 저 혈압, 서맥의 발생률이 더 증가할 가능성을 토대로 dexmedetomidine 용량에 따른 부작용 발생률을 분석하였으나, 용량에 따른 발생률의 차이는 없었다.
Dexmedetomidine은 낮은 농도에서는 α-2a 수 용체에 선택적으로 작용하여 혈관확장 작용에 의한 저혈압이 발생할 수 있지만, 용량이 증가함에 따라 수 용체에 대한 선택성을 잃고 α-2b 수용체에도 작용하 게 되는데 이 경우 혈관수축이 발생할 수 있다.18) 그 러므로 용량이 증가함에 따라 저혈압 발생률이 더 높 아지지 않는 것은 약물 기전상 합당한 결과로 보인다.
이 연구는 본원에서의 dexmedetomidine 투여 현황을 파악하고, dexmedetomidine 투여로 인해 발생하는 부작용인 저혈압, 서맥의 발생률과 위험인 25.4 ± 6.0 20.5 ± 2.9 0.414 50.0 ± 9.9 41.3 ± 9.5 0.977
Days of stay in hospital 39 (16-67) 26 (11-56) 0.059 27 (12-58) 32 (19-65) 0.470 Days of stay in ICU* 13 (7-33) 11 (6-21) 0.264 11 (7-23) 21 (7-55) 0.253 Death, n(%) 17 (47.2) 65 (65.7) 0.052 79 (62.2) 3 (37.5) 0.262 Days of using mechanical
ventilator
Table 8 Association between adverse events and outcome variables
P value
P value Brady
group (n=8) groupHypo
(n=99)
Non-brady group (n=127) Non-hypo
group (n=36)
Data are expressed as mean ± standard deviation (SD), median (range) or numbers (%) of patients.
*ICU; intensive care unit
자를 알아보기 위해 다양한 요인을 분석하였다는 데 의의가 있다. 그 결과 저혈압, 서맥이 발생할 수 있는 위험인자를 찾을 수 있었고, 특히 저혈압의 경우 다변 량 분석을 시행하여 독립적 위험인자를 도출할 수 있 었다. 기존 논문이 대부분 dexmedetomidine 투 여에 따른 저혈압 발생과 관련된 주제에만 국한되어 있었다면18) 본 연구에서는 한국인을 대상으로 하여 저혈압과 서맥의 발생률을 모두 분석하였고, 위험인 자를 찾아낸 것에 의의가 있다고 할 수 있다.
하지만 이 연구는 단일기관에서 수행되었고 전자기 록을 통한 후향적 연구인 한계점이 있다. 또한 낮은 서맥 발생률로 인하여 서맥에 대한 다변량 분석을 실 시하지 못하여 서맥에 대한 독립적 위험인자를 찾아 내지 못하였고 중환자 특성상, 부작용 발생률 및 예후 평가를 약물 단독 요인으로 판단하기 어렵다는 한계 점이 있다. 그러므로 추후 많은 환자를 대상으로 한 전향적 연구를 통해 이러한 한계점을 극복하는 것이 필요하겠다.
결론
Dexmedetomidine의 심혈관계 부작용의 발생을 조사한 결과, 저혈압 73.3%, 서맥 5.9%의 발생 빈 도를 보였으며 투여 시작으로부터 24시간 이내와 이 후에 고르게 발생하는 양상을 나타내었다. 특히 입실 시 낮은 MAP (mean arterial pressure)를 보이 는 경우, ARDS (acute respiratory distress syndrome)로 진단되거나, norepinephrine 투 여로 혈압을 유지중인 환자의 경우 저혈압 발생 가능 성이 높으므로, 이러한 위험인자를 가진 환자에서 dexmedetomidine 투여 시 면밀한 심혈관계 부작 용 모니터링이 필요하겠다.
참고문헌
1) Desbiens NA, Wu AW, Broste SK et al.
Pain and satisfaction with pain control in seriously ill hospitalized adults: find- ings from the SUPPORT research inves- tigations. For the SUPPORT investiga- tors. Study to Understand Prognoses
and Preferences for Outcomes and Risks of Treatment. Crit Care Med. 1996;24 (12):1953-61.
2) Friese RS. Sleep and recovery from crit- ical illness and injury: a review of theo- ry, current practice, and future direc- tions. Crit Care Med. 2008;36(3):697 -705.
3) Barr J, Fraser GL, Puntillo K et al. Clin- ical practice guidelines for the manage- ment of pain, agitation, and delirium in adult patients in the intensive care unit.
Crit Care Med. 2013;41(1):263-306.
4) Devlin JW, Roberts RJ. Pharmacology of commonly used analgesics and sedatives in the ICU: benzodiazepines, propofol, and opioids. Anesthesiol Clin. 2011;29 (4):567-85.
5) Weerink MAS, Struys MMRF, Hanni- voort LN et al. Clinical Pharmacokinet- ics and Pharmacodynamics of Dexme- detomidine. Clin Pharmacokinet. 2017;
56(8):893-913.
6) Wunsch H, Kahn JM, Kramer AA et al.
Use of intravenous infusion sedation among mechanically ventilated patients in the United States. Crit Care Med.
2009;37(12):3031-9.
7) Nguyen D, Abdul-Rasool I, Ward D et al.
Ventilatory effects of dexmedetomidine, atipamezole, and isoflurane in dogs.
Anesthesiology. 1992;76(4):573-9.
8) Riker RR, Shehabi Y, Paula MB et al.
Dexmedetomidine vs midazolam for se- dation of critically ill patients: a rand- omized trial. JAMA. 2009;301(5):489- 99.
9) Chrysostomou C, Schmitt CG. Dexme- detomidine: sedation, analgesia and be- yond. Expert Opin Drug Metab Toxicol.
2008;4(5):619-27.
10) Ebert TJ, Hall JE, Barney JA et al. The effects of increasing plasma concentra- tions of dexmedetomidine in humans.
Anesthesiology. 2000;93(2):382-94.
11) Maldonado JR. Delirium in the acute care setting: characteristics, diagnosis and treatment. Crit Care Clin. 2008;
24(4):657-722.
12) Ely EW, Shintani A, Truman B et al.
Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291 (14):1753-62.
13) Gerlach AT, Dasta JF, Steinberg S et al. A new dosing protocol reduces dex- medetomidine-associated hypotension in critically ill surgical patients. J Crit Care. 2009;24(4):568-74.
14) Devabhakthuni S, Pajoumand M, Wil- liams C et al. Evaluation of dexmedeto- midine: safety and clinical outcomes in critically ill trauma patients. J Trau- ma. 2011;71(5):1164-71.
15) Silva Júnior GB, Daher EF, Mota RM et al. Risk factors for death among criti- cally ill patients with acute renal fail- ure. Sao Paulo Med J. 2006;124(5):257- 63.
16) Alves GC, Silva Júnior GB, Lima RSA et al. Risk factors for death among criti- cally ill elderly patients. Rev Bras Ter Intensiva. 2010;22(2):138-43.
17) Gerlach AT, Dasta JF. Dexmedetomi- dine: an updated review. Ann Pharma- cother. 2007;41(2):245-52.
18) Gerlach AT, Blais DM, Jones GM et al.
Predictors of dexmedetomidine-associ- ated hypotension in critically ill pa- tients. Int J Crit Illn Inj Sci. 2016;
6(3):109-14.
19) Kao KC, Chang CH, Hung CY et al.
Survival predictor in patients with acute respiratory distress syndrome and diffuse alveolar damage undergo- ing open lung biopsy. PLoS One. 2017;
12(7):e0180018.
20) Hudson LD, Milberg JA, Anardi D et al.
Clinical risks for development of the acute respiratory distress syndrome.
Am J Respir Crit Care Med. 1995;151(2 Pt 1):293-301.
21) Uhle F, Lichtenstern C, Brenner T et al. Pathophysiology of Sepsis. Anas- thesiol Intensivmed Notfallmed Sch- merzther. 2015;50(2):114-22.