Korean Journal of Pediatric Urology Vol 1, No. 2: 126-129, 2009
126
CASE REPORT
Atypical Focal Xanthogranulomatous Pyelonephritis in a Child
Misdiagnosed as Renal Cell Carcinoma
Jong Kil Nam, Sung Woo Park, Sang Don Lee
From the Department of Urology, Pusan National University School of Medicine, Yangsan, Korea
남종길ㆍ박성우ㆍ이상돈 부산대학교 의과대학 비뇨기과학교실
Xanthogranulomatous (XGP) pyelonephritis is rare in children. The focal disease may be seen at computed tomogram as a focal mass of low at- tenuation with rim enhancement with an associated calculus. When these characteristic features are atypical, differentiation from renal cell carci- noma is impossible. Herein, we reported a case of a 13 year-old girl with atypical focal XGP xanthogranulomatous pyelonephritis without any cal- cification, who suspected preoperatively with a renal cell carcinoma (RCC).
Key Words: Pyeolnephritis, Xanthogranulomatous, Child 교신저자
Sang Don Lee
Department of Urology, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Beomo-ri, Mulgeum-eup, Yangsan 626-770, Korea Tel: 055-360-2134 Fax: 055-360-2931 E-mail: [email protected]
Xanthogranulomatous (XGP) pyelonephritis in children is a very rare form of chronic infection of the kidney and surrounding tissues characterized by destruction and replace- ment of renal parenchyma by lipid-laden macrophages.1 This disease is an uncommon chronic inflammatory process, frequently associated with renal calculi and chronic urinary tract infections. Although middle-aged women are pre- dominantly affected, the disease may be seen a rare in children.2 Clinically, most patients have malaise, fatigue, lethargy, flank pain, recurrent low-grade fever and recurrent urinary tract infection,3 and abdominal radiography typically demonstrates enlargement of the affected kidney with evi- dence of a staghorn calculus.1,4 But, an atypical XGP xan- thogranulomatous pyelonephritis is indistinguishable from renal cell carcinoma (RCC) or other tumors which shows small, focal mass without a staghorn calculus.1
Here we present a case of atypical focal XGP xanth- ogranulomatous pyelonephritis without calculi in child mis- diagnosed as a renal cell carcinoma RCC, with a review of the literature.
CASE REPORT
A 13-year-old female had a fever, right flank pain. Her initial body temperature was 37.7oC. A physical examination revealed tenderness of the right renal area, but no mass was palpable. Laboratory studies at first visit show an elevated erythrocyte sedimentation rate (ESR 89 mm/hr), C-reactive protein (CRP 11.37 mg/dl), anemia (Hb 10.2 g/dl), and leukocytosis (WBC 13,640/mm3). Urinalysis and other rou- tine blood biochemistry results were within normal limits.
A ultrasonography of the kidney shows a relatively demar- cated and 3.5 cm sized hypoechoeic lesion in the middle portion of the right kidney with mild contour bulging (Fig.
1A). On color doppler imaging, the renal vessel was displaced by this mass. Abdominal computerized tomogra- phy with contrast demonstrates a well demarcated, round soft tissue mass with low attenuation center at the middle portion of the right kidney (Fig. 1B). On magnetic re- sonance imaging of kidney shows 3.3×3.8 cm sized, well
Jong Kil Nam, et al: Atypical Focal XGP in a Child Misdiagnosed as a RCC 127
Fig. 1. Ultrasonography of the abdomen shows a mild contour bulging and relatively demarcated hypoechoeic lesion in the middle portion of the slightly enlarged right kidney (white arrow) (A). Abdominal computed tomography with contrast demonstrates a well demarcated, round soft tissue density mass at the middle portion of the right kidney (black arrow) (B).
Fig. 2. Magnetic resonance images of kidney show 3.3×3.8 cm sized, well defined mass in the middle portion of right kidney.
Coronal T1 (A), T2-weighted image (B) and contrast-enhanced T1-weighted image (C) demonstrate a thick-walled, peripherally enhancing, intermediated signal intensity lesion.
defined mass with the irregular, nonenhancing, low signal intensity center in the middle portion of right kidney.
Coronal T1 (Fig. 2A), T2-weighted image (Fig. 2B) and contrast-enhanced T1-weighted image (Fig. 2C) demonstra- tes a thick-walled, peripherally enhancing, intermediated signal intensity lesion. Generally, on contrast enhanced imaging, conventional RCC have dense enhancement, how- ever, this case showed a peripheral wall enhancement largely. Accordingly, we suspected the mass to be a non-conventional RCC or some other type of renal tumor with central necrosis such as oncocytoma. We decided to
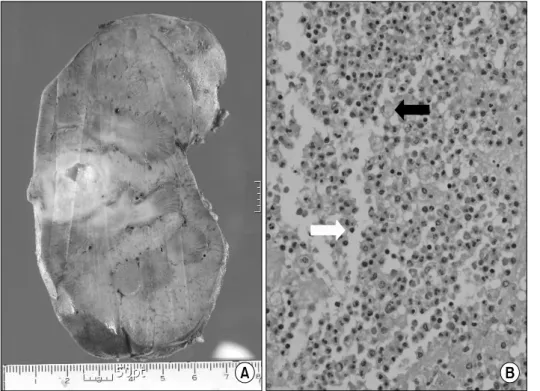
operate because we could not completely rule out the possibility of malignancy and then, patient underwent a laparoscopic radical nephrectomy. Laparoscopic partial nephrectomy was not possible because of the extensive fibrous adhesion from inflammation, and there was the potential risk of renal hilar injury. Grossly, the specimen contained a 155 gm weighted mass with yellow color, cavitary lesion. A 2.5-cm poorly demarcated mass was present in the middle portion of the kidney and involved the renal capsule (Fig 3A). Microscopic findings of the specimen shows lipid-laden macrophages (foam cells) and
128 Korean Journal of Pediatric Urology Vol. 1, 126-129, 2009
Fig. 3. On coronal section, middle portion of kidney shows an soft, yellow color and cavitary lesion respond- ing to the xanthogranulo- matous inflammation (A).
Microscopic findings of the specimen show lipid-laden macrophages (foam cells) (black arrow) and plasma cells (white arrow) (H&E,
×200) (B).
plasma cells (Fig 3B).
One months after the operation, the child has been a good general condition without any abnormal findings on follow up study.
DISCUSSION
XGP is an uncommon complication of long-standing urinary tract obstruction with a superimposed chronic infection, usually Proteus mirabilis or Escherichia coli.2,5 It can occur at any age, predominantly affects adults in the 5th through 7th decades of life. Approximately 70% of patients are women according to Anhalt and Cawood.6 XGP in children is rare, only 7 cases reported in the Korean literatures.7 Clinically, most patients have malaise, fatigue, lethargy, flank pain, palpable mass, hematuria, frequency, urgency, recurrent fever and recurrent urinary tract infection.2,8 In children, the clinical features and laboratory findings of XGP resemble those of chronic pyonephritis more closely than in adults. And this similarity may be determined by an affected immune response.4 In our case, physical findings include tenderness in the renal area with a mild fever of body temperature 37.7oC for 2 weeks but no palpable mass.
On the preoperative ultrasonogrphy and CT of abdomen, renal solid tumor was suspected primarily. Although the focal form of XGP may still be mistaken for a renal cell carcinoma, the commonly seen diffuse form (92%) has characteristic imaging features.2 In diffuse form, computed tomography frequently demonstrates characteristic features of XGP and accurately depicts extension of the inflamma- tory process beyond the kidney. On computed tomography imagings, the kidney is diffusely enlarged, and the renal parenchyma is replaced by multiple low-attenuation rounded masses. A central calcification is frequently identified within the renal pelvis and calyx. On contrast enhanced imagings, enhancement of the peripheral aspect of the rounded masses is seen, reflecting the vascularity within the granulation tissue and the compressed normal renal parenchyma sur- rounding the dilated calyces and cavities. Less common computed tomography findings include absence of calculi, massive pelvic dilatation, or a small contracted kidney with parenchymal destruction. With these less specfic findigns, an accurate preoperative diagnosis is rarely made.4 Besides, computed tomography is particularly helpful for evaluation of extension of the inflammatory process beyond the kidney and for surgical planning.
The focal disease may be seen at sonography as a hypoe-
Jong Kil Nam, et al: Atypical Focal XGP in a Child Misdiagnosed as a RCC 129
choic mass with an associated calculus or duplication. On computed tomography, a focal mass of low attenuation with rim enhancement is seen, usually with an associated cal- culus.5,7 As this case, when there are atypical findings, differential diagnosis from RCC is very difficult.
Grossly, the calyces, if preserved, are dilated or occasion- ally compressed and are lined by yellow soft tissue. Cortical atrophy is generally present and more advanced cases shows parenchymal abscesses. A renal calculus is frequently found in the renal pelvis surrounding fibrosis. The focal form has grossly similar features to those of the diffuse disease. The process is confined to small lesion containing a calculus or duplicated system with an associated calculus.9 Microscopi- cally, the inflammatory zone is associated with a pre- dominant plasma cell infiltrate and lipid-laden macrophages with a finely granular cytoplasm.9
Treatment of choice is total nephrectomy for diffuse form of XGP. In selected cases, partial nephrectomy or antibiotic therapy has been advocated for the treatment of very focal disease.10 But, it is important to differentiate atypical cases from RCC or other renal tumors.9 In this case, the pre- operative radiologic findings matched with renal cell car- cinoma or other renal tumor, but the postoperative path- ologic finding was XGP.
Focal XGP without calculus in children is a very rare, and preoperative diagnosis is very difficult. But, if renal mass is associated with recurrent urinary tract infection, renal calculus, fever and chilling, anemia, leukocytosis, we should consider a possibility of XGP.
REFERENCES
1. Hammadeh MY, Nicholls G, Calder CJ, Buick RG, Gorn- all P, Corkery JJ. Xanthogranulomatous pyelonephritis in childhood: pre-operative diagnosis is possible. Br J Urol 1994;73:83-6
2. Samuel M, Duffy P, Capps S, Mouriquand P, Williams D, Ransley P. Xanthogranulomatous pyelonephritis in childho- od. J Pediatr Surg 2001;36:598-601
3. Kural AR, Akaydin A, Oner A, Ozbay G, Solok V, Oruc N, et al. Xanthogranulomatous pyelonephritis in children and adults. Br J Urol 1987;59:383-5
4. Jung GW, Jeong MK, Yoon JB. Xanthogranulomatous pyelonephritis in childhood: a case report. Korean J Urol 1986;27:911-4
5. Elder JS, Marshall FF. Focal xanthogranulomatous pyelone- phritis in adulthood. Johns Hopkins Med J 1980;146:
141-7
6. Anhalt MA, Cawood CD. Xanthogranulomatous pyelone- phritis: a comprehensive review with report of 4 additional cases. J Urol 1971;105:10-7
7. Lee HN, Kim KH, Ryu IW, Han MC, Chung WS.
Xanthogranulomatous pyelonephritis in an infant. Korean J Urol 2006;47:1367-70
8. Kang TW, Jung SI, Jung GW. Clinical studies of xanth- ogranulomatous pyelonephritis. Korean J Urol 2001;42;
279-84
9. Kim YJ, Huh JS. Clinical characteristics of xanthogranulo- matous pyelonephritis. Korean J Urol 2004;45:935-40 10. Rasoulpour M, Banco L, Mackay IM, Hight DW, Berman
MM. Treatment of focal xanthogranulomatous pyeloneph- ritis with antibiotics. J Pediatr 1984;105:423-5